Download presentation
Presentation is loading. Please wait.

1
The Respiratory System
22 P A R T B The Respiratory System

2
External Respiration versus Internal Respiration
External Respiration is the exchange of gases between the outside atmosphere and the blood (from outside air into pulmonary capillaries) Internal Respiration is the exchange of gases between the blood and the tissue cells (from capillaries into tissue cells)
 Internal Respiration is the exchange of gases between the blood and the tissue cells (from capillaries into tissue cells)")
4
External Respiration Internal Respiration Figure 22.17

5
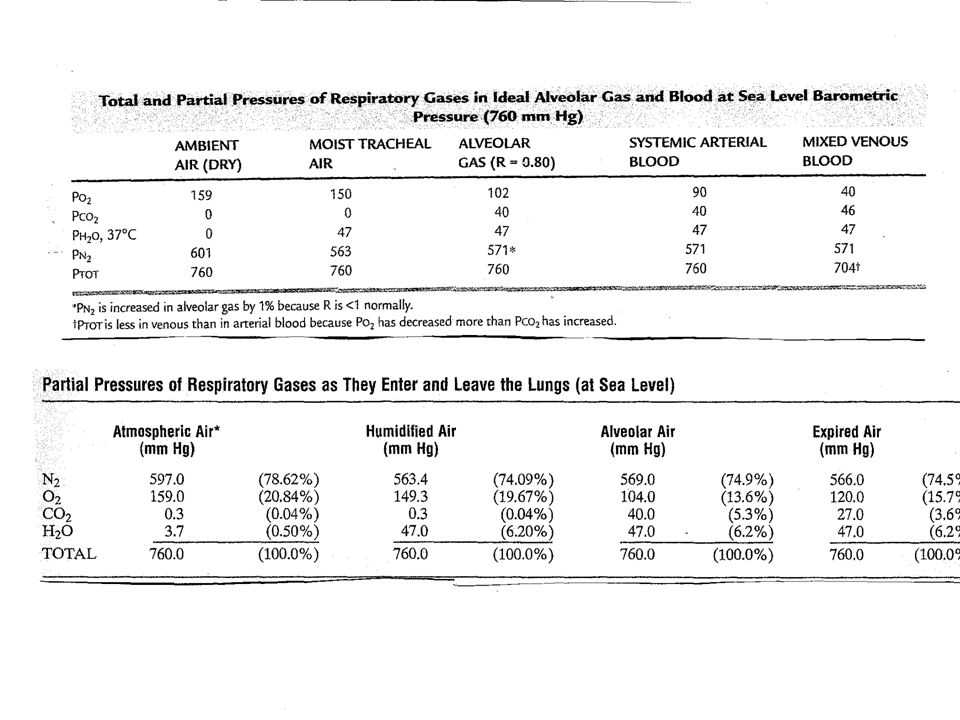
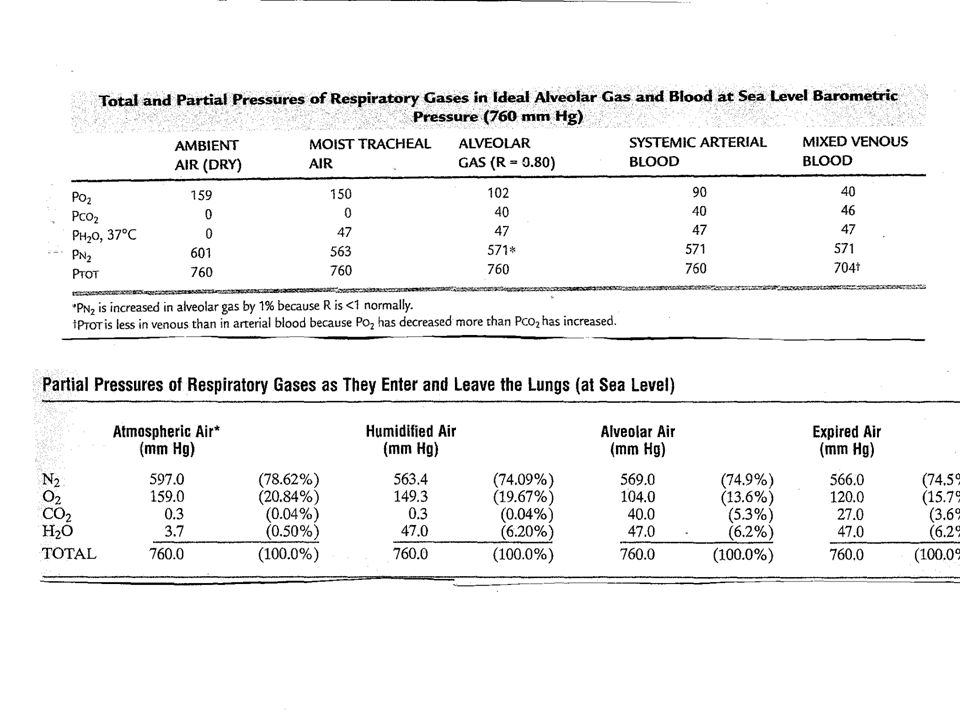
Pv – Partial Pressure of venous gas PATMO2 – 159 mmHg PAO2 – 104 mmHg
PATM – Partial Pressure of Gas in Atmosphere PA – Partial Pressure of alveolar gas Pa – Partial Pressure of arterial gas Pv – Partial Pressure of venous gas PATMO2 – 159 mmHg PAO2 – 104 mmHg PaO mmHg PvO2 – 40 mmHg _________________________________ PATM CO2 – 0.3 mmHg PACO2 – 40 mmHg PaCO mmHg PvCO2 – 45 mmHg

6
Composition of Alveolar Gas
The atmosphere is mostly oxygen and nitrogen, while alveoli contain more carbon dioxide and water vapor These differences result from: Nitrogen has a poor solubility coefficient – thus does not want to mix with blood easily Carbon Dioxide has an excellent solubility coefficient Humidification (watering the air) of air by conducting passages – airways have water on the surfaces.
 of air by conducting passages – airways have water on the surfaces.")
7
External Respiration: Pulmonary Gas Exchange
Factors influencing the movement of oxygen and carbon dioxide across the respiratory membrane 1. Partial pressure gradients and gas solubilities 2. Matching of alveolar ventilation and pulmonary blood perfusion 3. Structural characteristics of the respiratory membrane

8
Discussion of Oxygen Transport

9
Partial Pressure Gradients and Gas Solubilities
The partial pressure oxygen (PO2) of venous blood is 40 mm Hg; the partial pressure in the alveoli is 104 mm Hg This steep gradient allows oxygen partial pressures to rapidly reach equilibrium (in 0.25 seconds), and thus blood can move three times as quickly (0.75 seconds) through the pulmonary capillary and still be adequately oxygenated
 of venous blood is 40 mm Hg; the partial pressure in the alveoli is 104 mm Hg. This steep gradient allows oxygen partial pressures to rapidly reach equilibrium (in 0.25 seconds), and thus blood can move three times as quickly (0.75 seconds) through the pulmonary capillary and still be adequately oxygenated.")
10
Oxygenation of Blood Figure 22.18

11
Partial Pressure Gradients and Gas Solubilities
Although carbon dioxide has a lower partial pressure gradient: It is 20 times more soluble in plasma than oxygen It diffuses in equal amounts with oxygen Oxygen Carbon Dioxide (likes to dissolve in water the best) Nitrogen – 0.012 Carbon Monoxide – 0.018
 Nitrogen – Carbon Monoxide –")
13
Formulas of Importance
Diffusion – net movement of certain particles from a region of high concentration of those certain particles to region of low concentration of those certain particles D = A x Dc /t (Co – Ci) A is the area of the membrane being diffused through, Dc is the diffusion coefficient, t- is the thickness of the membrane being diffused through, Co – Ci is the concentration difference between the o (outside) and I (inside) of the container The diffusion coefficient = solubility coefficient divided by the square root of the molecular weight of the substance diffusing (this applies more to gases) Analysis- the greater the area and/or diffusion coefficient – the faster the rate of diffusion. The more the concentration difference the faster the rate of diffusion. However, the thicker the membrane to diffuse through the slower the rate of diffusion.
 A is the area of the membrane being diffused through, Dc is the diffusion coefficient, t- is the thickness of the membrane being diffused through, Co – Ci is the concentration difference between the o (outside) and I (inside) of the container. The diffusion coefficient = solubility coefficient divided by the square root of the molecular weight of the substance diffusing (this applies more to gases) Analysis- the greater the area and/or diffusion coefficient – the faster the rate of diffusion. The more the concentration difference the faster the rate of diffusion. However, the thicker the membrane to diffuse through the slower the rate of diffusion.")
14
Henry’s Law The amount of gas that will dissolve in a liquid depends on the partial pressure of the gas above the liquid (push down force) and the solubility coefficient of the gas for the liquid (pull down force). Solubility Coefficients of Gases in H2O (Determination of how much a certain gas likes a certain liquid) Oxygen Carbon Dioxide (likes to dissolve in water the best) Nitrogen – 0.012 Carbon Monoxide – 0.018
 and the solubility coefficient of the gas for the liquid (pull down force). Solubility Coefficients of Gases in H2O. (Determination of how much a certain gas likes a certain liquid) Oxygen Carbon Dioxide (likes to dissolve in water the best) Nitrogen – Carbon Monoxide –")
15
A tissue cell generally needs only 1 – 3mmHg
The pp of O2 in tissue cells ranges from 5mm Hg to 40 mmHg with an average of 23 mm Hg. A tissue cell generally needs only 1 – 3mmHg to fully support all of its oxygen requiring chemical processes The pp of CO2 in tissue cells is generally 46 mmHg Figure 22.17

16
A tissue cell should ideally be
20 – 30 micromillimeters from a capillary and at absolute maximum 100 micromillimeters. The intracellular oxygen partial pressure averages 23 mm Hg and the interstitial fluid oxygen partial pressure averages 40 mm Hg.. Thus oxygen can easily diffuse down this steep concentration gradient from the 95 – 104 mm Hg in the arterial end of the capillary to the 23 mm Hg in the cell.

17
The intracellular carbon dioxide partial pressure averages 46 mm Hg and the
interstitial fluid oxygen partial pressure averages 45 mm Hg. With the arterial end of the capillary having a partial pressure of 40 mmHg. Thus carbon dioxide has less of concentration gradient difference than oxygen. However, its diffusion is as good as oxygen due to its excellent solubility coefficients for both water (blood) and lipids (cell membranes). cell.
 and lipids (cell membranes). cell.")
18
Oxygen Delivery Oxygen in the atmosphere is 20.84% with a partial pressure of 159 mm Hg. When air enters the airways the water vapor concentration increases from 0.50% (pp of 3.7 %) in the atmosphere to 6.2 % (pp 47) in the mouth and respiratory pipes thus squeezing down the percentage of O2 to 9.6% (pp of mm Hg). When air enters the alveolus the O2 percentage drops even more due to increased partial pressure of CO2 in the alveolus. This squeezes the partial pressure of O2 to 104 mm Hg.
 in the atmosphere to 6.2 % (pp 47) in the mouth and respiratory pipes thus squeezing down the percentage of O2 to 9.6% (pp of mm Hg). When air enters the alveolus the O2 percentage drops even more due to increased partial pressure of CO2 in the alveolus. This squeezes the partial pressure of O2 to 104 mm Hg.")
20
O2 diffuses (pp 104 mm Hg) across the exchange membranes – then into the capillaries – where the O2 partial pressure is 40 mm Hg.
 across the exchange membranes – then into the capillaries – where the O2 partial pressure is 40 mm Hg.")
21
Oxygen Loading into the blood
Oxygen is carried in the blood in two ways 97% - 98% is carried on Hemoglobin and 2% – 3% is dissolved in the plasma Oxygen in hemoglobin is carried on the iron as long as the iron is in the +2 oxidation state (Fe ++ ferrous) – but if it is oxidized to the + 3 oxidation state (ferric) Fe +++ it will not carry oxygen Amount of Oxygen carried on a gram of hemoglobin is between 1.32 to 1.39 ml.
 – but if it is oxidized to the + 3 oxidation state (ferric) Fe +++ it will not carry oxygen. Amount of Oxygen carried on a gram of hemoglobin is between 1.32 to 1.39 ml.")
22
Oxygen Transport: Role of Hemoglobin
Each Hb molecule binds four oxygen atoms in a rapid and reversible process The hemoglobin-oxygen combination is called oxyhemoglobin (HbO2) Hemoglobin that has released oxygen is called reduced hemoglobin (HHb) Lungs HHb + O2 HbO2 + H+ Tissues
 Hemoglobin that has released oxygen is called reduced hemoglobin (HHb) Lungs. HHb + O2. HbO2 + H+ Tissues.")
23
The rate that hemoglobin binds and releases oxygen is regulated by:
Hemoglobin (Hb) Saturated hemoglobin – when all four hemes of the molecule are bound to oxygen Partially saturated hemoglobin – when one to three hemes are bound to oxygen The rate that hemoglobin binds and releases oxygen is regulated by: PO2, temperature, blood pH, PCO2, and the concentration of BPG (an organic chemical) These factors ensure adequate delivery of oxygen to tissue cells
 Saturated hemoglobin – when all four hemes of the molecule are bound to oxygen. Partially saturated hemoglobin – when one to three hemes are bound to oxygen. The rate that hemoglobin binds and releases oxygen is regulated by: PO2, temperature, blood pH, PCO2, and the concentration of BPG (an organic chemical) These factors ensure adequate delivery of oxygen to tissue cells.")
24
Influence of PO2 on Hemoglobin Saturation
Hemoglobin saturation plotted against PO2 produces a oxygen-hemoglobin dissociation curve 98% saturated arterial blood contains 20 ml oxygen per 100 ml blood (20 vol %) – 19.6 ml. bound to Hgb and .04 ml dissolved in the plasma (14.6 grams of Hgb/dl x 1.34 ml of O2 per gram) As arterial blood flows through capillaries, 5 ml oxygen are released The saturation of hemoglobin in arterial blood explains why breathing deeply increases the PO2 but has little effect on oxygen saturation in hemoglobin
 – 19.6 ml. bound to Hgb and .04 ml dissolved in the plasma (14.6 grams of Hgb/dl x 1.34 ml of O2 per gram) As arterial blood flows through capillaries, 5 ml oxygen are released. The saturation of hemoglobin in arterial blood explains why breathing deeply increases the PO2 but has little effect on oxygen saturation in hemoglobin.")
25
Hemoglobin O2 Association/ Dissociation Curve
Loading Unloading Explanation of the dynamics of O2 carriage on Hgb Allosteric Effect of Hgb. Figure 22.20

26
Hemoglobin Association/Dissociation (Saturation) Curve
Hemoglobin is almost completely saturated at a PO2 of 70 mm Hg Further increases in PO2 produce only small increases in oxygen binding Oxygen loading and delivery to tissue is adequate when PO2 is below normal levels

27
Hemoglobin Association/Dissociation (Saturation) Curve
Only 20–25% of bound oxygen is unloaded during one systemic circulation If oxygen levels in tissues drop: More oxygen dissociates from hemoglobin and is used by cells Respiratory rate or cardiac output need not increase

28
Hemoglobin O2 Association/ Dissociation Curve
Loading Unloading Explanation of the dynamics of O2 carriage on Hgb Figure 22.20

29
Structure of Hemoglobin
O2 locations Allosteric explanation When O2 loads or unloads on one heme (iron)– due to the structure of Hgb -it slightly twists the molecule affecting the other hemes. Figure 17.4
– due to the structure. of Hgb -it slightly twists the molecule affecting the other hemes. Figure")
30
Shifting of The Curve Certain factors (pH change, Temp change, 2,3 BPG concentration change, PaCO2 change) can cause the Oxygen Association/Dissociation Curve to shift to the right or left If the curve shifts to the right it means that hemoglobin has a decreased affinity for O2- thus O2 will unload (dissociate) easier from Hgb. This shift is termed the Bohr shift (Christian Bohr, Danish physiologist father of Niels Bohr, famous physicist). If the curve shifts to the left it means that hemoglobin has an increased affinity for O2- thus O2 will load easier onto Hgb and be held onto tighter by Hgb.
 can cause the Oxygen Association/Dissociation Curve to shift to the right or left. If the curve shifts to the right it means that hemoglobin has a decreased affinity for O2- thus O2 will unload (dissociate) easier from Hgb. This shift is termed the Bohr shift (Christian Bohr, Danish physiologist father of Niels Bohr, famous physicist). If the curve shifts to the left it means that hemoglobin has an increased affinity for O2- thus O2 will load easier onto Hgb and be held onto tighter by Hgb.")
32
Explanation of Curve Shift (use p50 value)
The red curve (more leftward) represents a higher O2/Hgb affinity. Notice that even if the partial pressure of O2 around Hgb is down as low as a partial pressure of 8 mm Hg – only 50% of the oxygen molecules on Hgb will unload (2 out of 4). However the blue curve (more rightward) represents a lower O2/Hgb affinity. Notice that at a higher (30 mm hg) partial pressure of O2 around Hgb – the Hgb is willing to unload 50% of its oxygen. Thus it is not holding onto O2 as tightly.
 represents a higher O2/Hgb. affinity. Notice that even if the. partial pressure of O2 around. Hgb is down as low as a partial. pressure of 8 mm Hg – only 50% of the oxygen molecules on Hgb. will unload (2 out of 4). However. the blue curve (more rightward) represents a lower O2/Hgb. affinity. Notice that at a. higher (30 mm hg) partial pressure of O2 around Hgb – the Hgb is willing to unload 50% of its. oxygen. Thus it is not holding. onto O2 as tightly.")
33
Right Shift (less affinity shift) factors (Bohr Shift)
1. Increase in PaCO2 2. Increase in [2,3 BPG] 3. Increase in [H+] – thus more acidic pH 4. Increase in Temp – some suggest that an increased temp increases the 2,3 BPG concentration Left Shift (Increased affinity shift) factors 1. Decrease in PaCO2 2. Decrease in [2,3 BPG] 3. Decrease in [H+ ] – thus more acidic pH 4. Decrease in Temp – some suggest that a decreased temp decreases the 2,3 BPG concentration
 factors. 1. Decrease in PaCO2. 2. Decrease in [2,3 BPG] 3. Decrease in [H+ ] – thus more acidic pH. 4. Decrease in Temp – some suggest that a decreased temp decreases the 2,3 BPG concentration.")
34
Factors Shifting the Curve
Figure 22.21

35
2,3-Bisphosphoglycerate (2,3-BPG, also known as 2,3-diphosphoglycerate or 2,3-DPG) is a three-carbon isomer of the glycolytic intermediate 1,3-bisphosphoglycerate. 2,3-BPG is present in human red blood cells (RBC; erythrocyte) at approximately 5 mmol/L. It binds with greater affinity to deoxygenated hemoglobin (e.g., when the red cell is near respiring tissue) than it does to oxygenated hemoglobin (e.g., in the lungs). In binding to partially deoxygenated hemoglobin, it allosterically up-regulates the release of the remaining oxygen molecules bound to the hemoglobin, thus enhancing the ability of RBCs to release oxygen near tissues that need it most.
 at approximately 5 mmol/L. It binds with greater affinity to deoxygenated hemoglobin (e.g., when the red cell is near respiring tissue) than it does to oxygenated hemoglobin (e.g., in the lungs). In binding to partially deoxygenated hemoglobin, it allosterically up-regulates the release of the remaining oxygen molecules bound to the hemoglobin, thus enhancing the ability of RBCs to release oxygen near tissues that need it most..")
36
2,3-BPG is formed from 1,3-BPG by an enzyme called bisphosphoglycerate mutase. It is broken down by a phosphatase to form 3-phosphoglycerate. Its synthesis and breakdown are, therefore, a way around a step of glycolysis. glycolysis 1,3-BPG > 2, 3-PG

37
2,3 BPG

39
Questions Where would you position the fetal hemoglobin curve – A. to the right of the adult curve B. to the left of the adult curve C. superimposed on top of the adult curve Where would you position the myoglobin curve (red chemical in muscle that holds reserve oxygen) - A. to the right of the adult curve B. to the left of the adult curve C. superimposed on top of the adult curve
 - A. to the right of the adult curve B. to the left of the adult curve C. superimposed on top of the adult curve.")
41
Internal Respiration (Unloading) O2 to the tissues
O2 is delivered to tissue cells – some from the dissolved form in the plasma and some from the Hgb. The partial pressure in the tissue cells is generally around 40 mm Hg (Krebs cycle use of O2). The partial pressure of O2 in the arteriole end of the capillary (PaO2) is around 104 mm Hg. Thus O2 diffuses from the blood into the interstitial fluids then into the tissue cells. Under normal conditions only 1 out of 4 O2 molecules will diffuse from Hgb in the capillaries if the tissue (interstitial fluid) partial pressure is 40 mm Hg. However, if the tissue (interstitial fluid) partial pressure of O2 is lower than 40 mm Hg more O2 molecules will dissociate off the Hgb – and dissociate quicker (shown by the parabolic nature of the O2 curve.
. The partial pressure of O2 in the arteriole end of the capillary (PaO2) is around 104 mm Hg. Thus O2 diffuses from the blood into the interstitial fluids then into the tissue cells. Under normal conditions only 1 out of 4 O2 molecules will diffuse from Hgb in the capillaries if the tissue (interstitial fluid) partial pressure is 40 mm Hg. However, if the tissue (interstitial fluid) partial pressure of O2 is lower than 40 mm Hg more O2 molecules will dissociate off the Hgb – and dissociate quicker (shown by the parabolic nature of the O2 curve.")
42
Tissue Cell Pressures of O2 - 23 mm Hg
Interstitial Fluid pp of 40 mm Hg Arteriole Pressures Arteriole PP of O2 – 104 mm Hg Oxygen diffuses into tissue cells due to the difference in partial pressures

43
Hemoglobin O2 Association/ Dissociation Curve
75% Only 1 O2 dissociates from Hgb if the partial pressure of the tissues is 40 mm Hg. If lower more will unload and quicker Unloading Utilization Coefficient How many unload divided by how many present = 1/4 Figure 22.20

44
Reason why unloading needs to be faster if 1 O2 molecule unloaded did not bring tissue cells partial pressures to 40 mm Hg Blood in a capillary is only there for less than a second (around .75 seconds or less). Capillaries are only 0.25 μm – 1 μm in length. When hemoglobin has unloaded one O2 molecule – it is a third of the way in the capillary – if this one O2 did not return the tissue O2 partial pressures to the physiologic level of 40 mm Hg – then another O2 must be loaded and if still not enough another one. Each must be unloaded quicker than the previous one – since the blood is constantly reaching the end of the capillary where no further diffusion can occur. Thus the downward slope (dissociation direction) of the O2 curve must get steeper (rate getting faster) as O2 molecules are released from Hgb into the tissues.
. Capillaries are only 0.25 μm – 1 μm in length. When hemoglobin has unloaded one O2 molecule – it is a third of the way in the capillary – if this one O2 did not return the tissue O2 partial pressures to the physiologic level of 40 mm Hg – then another O2 must be loaded and if still not enough another one. Each must be unloaded quicker than the previous one – since the blood is constantly reaching the end of the capillary where no further diffusion can occur. Thus the downward slope (dissociation direction) of the O2 curve must get steeper (rate getting faster) as O2 molecules are released from Hgb into the tissues.")
45
Hemoglobin O2 Association/ Dissociation Curve
75% Only 1 O2 dissociates from Hgb if the partial pressure of the tissues is 40 mm Hg. If lower more will unload and quicker Unloading Steeper slope down after one O2 unloaded Figure 22.20

46
Unloading of Oxygen into Tissues
Figure 22.22a

47
PaO2 - 104 mmHg (clinical range 80 – 100)
Pa – Partial Pressure of arterial gas PaO mmHg (clinical range 80 – 100) Hypoxia – too low oxygen in the tissues Hypoxemia – too low oxygen in the blood Normoxia – normal oxygen level in the tissues Hyperoxia – too high oxygen concentration in the tissues – can cause bronchopulmonary dysplasia and/or be a contributing cause of retrolental fibroplasia in the newborn.
 Hypoxia – too low oxygen in the tissues. Hypoxemia – too low oxygen in the blood. Normoxia – normal oxygen level in the tissues. Hyperoxia – too high oxygen concentration in the tissues – can cause bronchopulmonary dysplasia and/or be a contributing cause of retrolental fibroplasia in the newborn.")
48
Types of Hypoxia Anemic Hypoxia – not enough hemoglobin to properly carry oxygen Ischemic (stagnant) Hypoxia – some blockage in the circulation to an area Histologic Hypoxia – the oxygen is getting to the tissues but cannot be utilized. Examples are poisons such as cyanide. Hypoxemic Hypoxia – something causing the blood not be able to pick up enough oxygen from the atmosphere (in a low oxygen environment, suffocation, CO poisoning, etc.)
 Hypoxia – some blockage in the circulation to an area. Histologic Hypoxia – the oxygen is getting to the tissues but cannot be utilized. Examples are poisons such as cyanide. Hypoxemic Hypoxia – something causing the blood not be able to pick up enough oxygen from the atmosphere (in a low oxygen environment, suffocation, CO poisoning, etc.)")
49
Histologic Hypoxia The oxygen gets to the tissues – but cannot be utilized 1. Mitochondrial Diseases – mitochondria which have their own DNA provided by the individuals mother has some genetic defect disallowing proper usage of oxygen in the electron transport chain 2. Cyanide Poisoning - The cyanide ion halts cellular respiration by inhibiting an enzyme in mitochondria called cytochrome c oxidase. This enzyme is needed to transfer electrons so as to make ATP.

50
Cytochrome C oxidase is the last enzyme in the respiratory electron transport chain of mitochondria located in the mitochondrial membrane. It receives an electron from each of four cytochrome c molecules, and transfers them to one oxygen molecule. In this complex hydrogens are transported to oxygen making water (H2O). Cytochrome Oxidase

51
Carbon Monoxide Poisoning
The affinity between hemoglobin and carbon monoxide is approximately 230 times stronger than the affinity between hemoglobin and oxygen so carbon monoxide binds to hemoglobin in preference to oxygen. Carbon monoxide can also bind to a myoglobin. It has a high affinity for myoglobin, about 60 times greater than that of oxygen. Carbon monoxide bound to myoglobin may impair its ability to utilize oxygen. Carbon monoxide can also bind to Cytochrome oxidase disturbing its function in the mitochondria in the production of ATP.

52
Carbon Monoxide Hemoglobin is a tetramer with four oxygen binding sites. The binding of carbon monoxide at one of these sites increases the oxygen affinity of the remaining three sites, which causes the hemoglobin molecule to retain oxygen that would otherwise be delivered to the tissue. This situation is described as carbon monoxide shifting the oxygen dissociation curve to the left. Because of the increased affinity between hemoglobin and oxygen during carbon monoxide poisoning, the blood oxygen content is increased. But because all the oxygen stays in the hemoglobin, none is delivered to the tissues. This causes hypoxic tissue injury. Carbon monoxide bound to hemoglobin make the hemoglobin look redder – thus the patient may have a cherry red appearance.

53
Hyperoxia conditions Bronchopulmonary dysplasia (BPD; formerly Chronic Lung Disease of Infancy) is a chronic lung disorder that is most common among children who were born prematurely, with low birth weights and who received prolonged mechanical ventilation to treat respiratory distress syndrome. BPD is clinically defined as oxygen dependence at 36 weeks' postmenstrual age. BPD is characterized by inflammation and scarring in the lungs. More specifically, the high pressures of oxygen delivery result in necrotizing bronchiolitis and alveolar septal injury, further compromising oxygenation of blood.
 is a chronic lung disorder that is most common among children who were born prematurely, with low birth weights and who received prolonged mechanical ventilation to treat respiratory distress syndrome. BPD is clinically defined as oxygen dependence at 36 weeks postmenstrual age. BPD is characterized by inflammation and scarring in the lungs. More specifically, the high pressures of oxygen delivery result in necrotizing bronchiolitis and alveolar septal injury, further compromising oxygenation of blood.")
54
Hyperoxia conditions Retinopathy of prematurity (ROP), previously known as retrolental fibroplasia (RLF), is an eye disease that affects prematurely born babies. It is thought to be caused by disorganized growth of retinal blood vessels which may result in scarring and retinal detachment. ROP can be mild and may resolve spontaneously, but may lead to blindness in serious cases. As such, all preterm babies are at risk for ROP, and very low birth weight is an additional risk factor. Both oxygen toxicity and relative hypoxia can contribute to the development of ROP.
, previously known as retrolental fibroplasia (RLF), is an eye disease that affects prematurely born babies. It is thought to be caused by disorganized growth of retinal blood vessels which may result in scarring and retinal detachment. ROP can be mild and may resolve spontaneously, but may lead to blindness in serious cases. As such, all preterm babies are at risk for ROP, and very low birth weight is an additional risk factor. Both oxygen toxicity and relative hypoxia can contribute to the development of ROP.")
55
Retinopathy Normally, maturation of the retina proceeds in-utero and at term, the mature infant has fully vascularized retina. However, in preterm infants, the retina is often not fully vascularized. ROP occurs when the development of the retinal vasculature is arrested and then proceeds abnormally. The key disease element is fibrovascular proliferation. Associated with the growth of these new vessels is fibrous tissue (scar tissue) that may contract to cause retinal detachment. Supplemental oxygen exposure, while a risk factor, is not the main risk factor for development of this disease. Restricting supplemental oxygen use does not necessarily reduce the rate of ROP, and may raise the risk of other hypoxia-related systemic complications.
 that may contract to cause retinal detachment. Supplemental oxygen exposure, while a risk factor, is not the main risk factor for development of this disease. Restricting supplemental oxygen use does not necessarily reduce the rate of ROP, and may raise the risk of other hypoxia-related systemic complications.")
56
Discussion of Nitric Oxide (NO) as it Relates to Hemoglobin
 as it Relates to Hemoglobin")
57
Hemoglobin-Nitric Oxide Partnership
Nitric oxide (NO) also known as endothelial derived relaxing factor (EDRF) is a vasodilator synthesized by the endothelial cells from L-arginine and oxygen by various nitric oxide synthase enzymes. Nitric oxide lasts only a few seconds – let diffuses freely from the endothelial cells to relax the smooth muscles of the blood vessel walls – resulting in vasodilation. Thus it plays a role in blood pressure regulation Nitric oxide (NO) also contributes to vessel homeostasis by inhibiting platelet aggregation, and leukocyte adhesion to the endothelium.
 also known as endothelial derived relaxing factor (EDRF) is a vasodilator synthesized by the endothelial cells from L-arginine and oxygen by various nitric oxide synthase enzymes. Nitric oxide lasts only a few seconds – let diffuses freely from the endothelial cells to relax the smooth muscles of the blood vessel walls – resulting in vasodilation. Thus it plays a role in blood pressure regulation. Nitric oxide (NO) also contributes to vessel homeostasis by inhibiting platelet aggregation, and leukocyte adhesion to the endothelium.")
58
Some special NO (termed SNO for S-nitrous thiols) is produced in the lung. This NO is attached to a cysteine amino acid on globin. Cysteine has a sulfhydryl R-group – thus it is called a thiol. O = N – S – R (amino acid cysteine) The NO attached to cysteine is protected from hemoglobin which gobbles up free NO produced by endothelial cells. When Hemoglobin unloads O2 in the tissues it also unloads SNO and picks up free NO made by the local endothelial cells as well as CO2. The picked up NO is carried on the Heme attached to the iron – this NO is not active thus cannot maintain vasodilation. However the SNO left behind maintains adequate vasodilation. But it has a short life – thus new NO needs to be produced in order to maintain the vasodilation. The excess NO carried on hemoglobin is taken to the lungs for exhalation.
 The NO attached to cysteine is protected from hemoglobin which gobbles up free NO produced by endothelial cells. When Hemoglobin unloads O2 in the tissues it also unloads SNO and picks up free NO made by the local endothelial cells as well as CO2. The picked up NO is carried on the Heme attached to the iron – this NO is not active thus cannot maintain vasodilation. However the SNO left behind maintains adequate vasodilation. But it has a short life – thus new NO needs to be produced in order to maintain the vasodilation. The excess NO carried on hemoglobin is taken to the lungs for exhalation.")
59
Discussion of Carbon Dioxide Transport

60
CO2 Transport CO2 transport originates in internal respiration (product of the Krebs cycle) – whereas O2 transport originated in external respiration – acquisition of O2 from the atmosphere.
 – whereas O2 transport originated in external respiration – acquisition of O2 from the atmosphere.")
61
CO2 diffuses from the tissue cells (CO2 formed in Krebs Cycle) that generally have an intracellular partial pressure of 45 mmHg. The CO2 then diffuses down its concentration first into the interstitial fluids – then into the capillaries (that under usual circumstances has a partial pressure of 40 mm Hg). Note: the partial pressure differences between CO2 is lower (45 mm Hg to 40 mm Hg) than that of O2 (104 mm Hg to 40 mm Hg) yet it can diffuse just as quickly. Why? Because CO2 has a much better solubility coefficient than O2 – thus water and lipid membranes likes it better. Solubility coefficient of Oxygen versus Carbon Dioxide D = A x Dc /t (Co – Ci)
. Note: the partial pressure differences between CO2 is lower (45 mm Hg to 40 mm Hg) than that of O2 (104 mm Hg to 40 mm Hg) yet it can diffuse just as quickly. Why Because CO2 has a much better solubility coefficient than O2 – thus water and lipid membranes likes it better. Solubility coefficient of Oxygen versus Carbon Dioxide D = A x Dc /t (Co – Ci)")
62
CO2 entrance into the blood
Once carbon dioxide enters the bloodstream it is carried in three forms 1. Dissolved in plasma – 7 to 10% 2. Chemically bound to hemoglobin – 20% - 23% is carried in RBCs as carbaminohemoglobin 3.Bicarbonate ion in plasma – 70% is transported as bicarbonate (HCO3–)
")
63
Transport and Exchange of Carbon Dioxide
2 1 3 Figure 22.22a

64
Transport and Exchange of Carbon Dioxide
Most (70%) of the carbon dioxide diffuses into RBCs and combines with water to form carbonic acid (H2CO3), which quickly dissociates into hydrogen ions and bicarbonate ions – In RBCs, carbonic anhydrase (enzyme produced in RBCs) reversibly catalyzes the conversion of carbon dioxide and water to carbonic acid NOTE: The reason so much CO2 is carried in the bicarbonate form is that while it is being carried it can act as a pH buffer – thus two tasks are accomplished at the same time – 1.eliminating CO2 and assisting in pH balance of the blood (discussed later) CO2 + H2O H2CO3 H+ HCO3– Carbon dioxide Water Carbonic acid Hydrogen ion Bicarbonate ion
 of the carbon dioxide diffuses into RBCs and combines with water to form carbonic acid (H2CO3), which quickly dissociates into hydrogen ions and bicarbonate ions – In RBCs, carbonic anhydrase (enzyme produced in RBCs) reversibly catalyzes the conversion of carbon dioxide and water to carbonic acid. NOTE: The reason so much CO2 is carried in the bicarbonate form is that while it is being carried it can act as a pH buffer – thus two tasks are accomplished at the same time – 1.eliminating CO2 and 2. assisting in pH balance of the blood (discussed later) CO2. + H2O. H2CO3. H+ HCO3– Carbon dioxide. Water. Carbonic acid. Hydrogen ion. Bicarbonate ion.")
65
Chloride Shift In order to maintain the balance of charges (Bulk Electro neutrality) in the RBC – when the negatively charged bicarbonate (HCO3- ) molecule moves out of the RBC into the plasma so as to assist in pH buffering the blood – the negatively charged chloride (Cl- ) ion enters into the RBC through a special integral protein in the RBC membrane known as the chloride transporter This action is termed the chloride shift (Hamburger shift) – named after Hartog Jakob Hamburger (1859–1924), a Dutch physiologist
 in the RBC – when the negatively charged bicarbonate (HCO3- ) molecule moves out of the RBC into the plasma so as to assist in pH buffering the blood – the negatively charged chloride (Cl- ) ion enters into the RBC through a special integral protein in the RBC membrane known as the chloride transporter. This action is termed the chloride shift (Hamburger shift) – named after Hartog Jakob Hamburger (1859–1924), a Dutch physiologist.")
66
Chloride Shift Figure 22.22a

67
Carbon dioxide carriage on Hemoglobin
Oxygen is carried on the heme portion of hemoglobin attached to iron in the +2 (ferrous) oxidation state. Carbon dioxide is carried on the protein globin component of hemoglobin. Carbon dioxide can bind to amino groups, creating carbamino compounds. Amino groups are available for binding at the N-terminals and at side-chains of arginine and lysine residues in hemoglobin. This forms carbaminohemoglobin.
 oxidation state. Carbon dioxide is carried on the protein globin component of hemoglobin. Carbon dioxide can bind to amino groups, creating carbamino compounds. Amino groups are available for binding at the N-terminals and at side-chains of arginine and lysine residues in hemoglobin. This forms carbaminohemoglobin.")
68
CO2 Association/Dissociation Curve
Not as curved (parabolic) as the O2 curve Not as much allosteric effect with Hgb Oxygen Curve
 as the O2 curve. Not as much. allosteric effect. with Hgb. Oxygen Curve.")
69
Haldane Effect (Shifting of the CO2 curve)
At the tissues, as more carbon dioxide enters the blood: More oxygen dissociates from hemoglobin (Bohr effect) rightward shift of the oxygen dissociation curve – partly caused by the allosteric effect caused by increased amounts of CO2 loading onto Hgb on globin – pushing off some O2 on the heme. This increased affinity of CO2 for globin on Hgb pushes the CO2 curve to the left – Haldane shift. This situation is reversed in pulmonary circulation
 rightward shift of the oxygen dissociation curve – partly caused by the allosteric effect caused by increased amounts of CO2 loading onto Hgb on globin – pushing off some O2 on the heme. This increased affinity of CO2 for globin on Hgb pushes the CO2 curve to the left – Haldane shift. This situation is reversed in pulmonary circulation.")
70
Haldane Effect The decreased saturation of Hgb by
O2 leads to an increased affinity of Hgb for CO2 (Haldane Shift) – leftward shift Figure 22.23
 – leftward shift. Figure")
71
Haldane Shift Bohr Shift The Haldane Shift is the leftward shift of the CO2 dissociation curve –which signifies increased affinity of Hgb for CO2. The rightward shift of the oxygen dissociation curve is the Bohr shift which signifies decreased affinity of Hgb for O2. Combining the curves together shows the allosteric effect of CO2 on O2 in Hgb and vice-versa the effect of O2 on CO2. In an environment where CO2 concentration predominates it pushes the O2 curve to the right and the CO2 curve to the left and vice versa where O2 concentration dominates.

72
External Respiration of Carbon Dioxide
At the lungs, these processes are reversed Bicarbonate ions move into the RBCs and bind with hydrogen ions to re-form carbonic acid. In exchange for the negatively bicarbonate moving in the negatively charged chloride moves out (reverse the chloride shift) Carbonic acid is then split by carbonic anhydrase to release carbon dioxide and water Carbon dioxide then diffuses from the blood into the alveoli (plasma unloading of CO2 into alveoli)
 Carbonic acid is then split by carbonic anhydrase to release carbon dioxide and water. Carbon dioxide then diffuses from the blood into the alveoli (plasma unloading of CO2 into alveoli)")
73
External Respiration of Carbon Dioxide
The CO2 dissolved in the plasma diffuses from the venous blood (45 mm Hg) into the alveolus (40 mm Hg) The CO2 attached to the globin portion of Hgb detaches from the Hgb and diffuses into the alveolus
 into the alveolus (40 mm Hg) The CO2 attached to the globin portion of Hgb detaches from the Hgb and diffuses into the alveolus.")
74
Transport and Exchange of Carbon Dioxide
Figure 22.22b

75
What controls Respiration
1. Discuss Reticular Activating Formation 2. Brain Centers (VRG, DRG, Pneumotaxic, Apneustic) 3. Central and Peripheral Chemoreceptors 4. Cortical Control 5. Limbic Control 6. Lung Stretch Receptors 7. Irritant Gases 8. Pain 9. Muscle stretch receptors
 3. Central and Peripheral Chemoreceptors 4. Cortical Control 5. Limbic Control 6. Lung Stretch Receptors 7. Irritant Gases 8. Pain 9. Muscle stretch receptors")
76
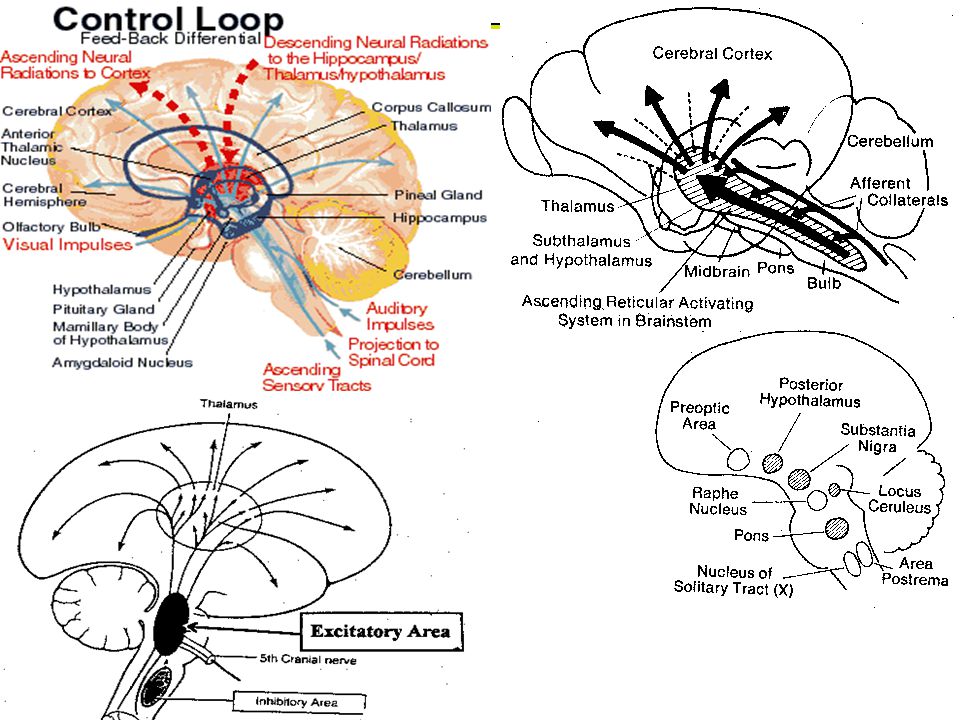
Reticular System in CNS
The reticular formation is a part of the brain that is involved in actions such as awaking/sleeping cycle, and filtering incoming stimuli to discriminate irrelevant background stimuli. It is essential for governing some of the basic functions of higher organisms, and is one of the phylogenetically oldest portions of the brain. The reticular formation is a poorly-differentiated area of the brain stem, centered roughly in the pons. The reticular formation is the core of the brainstem running through the mid-brain, pons and medulla. The ascending reticular activating system connects to areas in the thalamus, hypothalamus, and cortex, while the descending reticular activating system connects to the cerebellum and sensory nerves. The reticular activating system is a portion of the reticular formation – concerned with sleep/wake, arousal and alertness.

77
Reticular System (Functions)
1. Somatic motor control - Some motor neurons send their axons to the reticular formation nuclei, giving rise to the reticulospinal tracts of the spinal cord. These tracts function in maintaining tone, balance, and posture--especially during body movements. Other motor nuclei include gaze centers, which enable the eyes to track and fixate objects, and central pattern generators, which produce rhythmic signals to the muscles of breathing and swallowing

78
Reticular System (Functions)
2. Cardiovascular control - The reticular formation includes the cardiac and vasomotor centers of the medulla oblongata. 3. Pain modulation - The reticular formation is one means by which pain signals from the lower body reach the cerebral cortex. It is also the origin of the descending analgesic pathways. The nerve fibers in these pathways act in the spinal cord to block the transmission of some pain signals to the brain. 4. Sleep and consciousness - The reticular formation has projections to the thalamus and cerebral cortex that allow it to exert some control over which sensory signals reach the cerebrum and come to our conscious attention. It plays a central role in states of consciousness like alertness and sleep. Injury to the reticular formation can result in irreversible coma.

79
Reticular System (Functions)
5. Habituation - This is a process in which the brain learns to ignore repetitive, meaningless stimuli while remaining sensitive to others. A good example of this is when a person can sleep through loud traffic in a large city, but is awakened promptly due to the sound of an alarm or crying baby. Reticular formation nuclei that modulate activity of the cerebral cortex are called the reticular activating system or extrathalamic control modulatory system.

81
Brain Centers that Control of Respiration
Breathing is a somatic motor controlled action. There are nuclei in the brain that control the respiration – known as the respiratory centers. Medullary Centers 1.DRG (Dorsal Respiratory Group) 2.VRG (Ventral Respiratory Group) Pontine Centers 3. Pneumotaxic Center 4. Apneustic Center
 2.VRG (Ventral Respiratory Group) Pontine Centers. 3. Pneumotaxic Center. 4. Apneustic Center.")
82
Dorsal Respiratory Group (Controversy)
The dorsal respiratory group (DRG) is located in the dorsomedial region of the medulla, and is composed of cells in the solitary tract nucleus. The DRG is considered by most researchers to be involved in the generation of respiratory rhythm, and is primarily responsible for the generation of inspiration. However, there is some controversy now as to whether the VRG (Ventral Respiratory Group) initiates most of the signaling for inspiration. Newer thoughts state that the DRG receives the inputs from the peripheral stretch receptors and chemoreceptors and communicate this information to the VRG.
 is located in the dorsomedial region of the medulla, and is composed of cells in the solitary tract nucleus. The DRG is considered by most researchers to be involved in the generation of respiratory rhythm, and is primarily responsible for the generation of inspiration. However, there is some controversy now as to whether the VRG (Ventral Respiratory Group) initiates most of the signaling for inspiration. Newer thoughts state that the DRG receives the inputs from the peripheral stretch receptors and chemoreceptors and communicate this information to the VRG.")
83
Ventral Respiratory Group
The ventral respiratory group (VRG) is a column of neurons located in the ventrolateral region of the medulla The four cell groups of the VRG are the rostral nucleus retrofacialis, caudal nucleus retroambiguus, nucleus para-ambiguus, and the pre-Bötzinger complex. The VRG contains both inspiratory and expiratory neurons. Most researchers feel that the VRG is secondarily responsible for initiation of inspiratory activity, after the dorsal respiratory group. New thought is that the VRG may be the primary rhythm –generating and integrative center. New theory feels that the cyclic on/off switch between the inspiratory and expiratory neurons in the VRG – produce inhalation and exhalation – also setting the frequency at 12 – 15 breaths per minute – inspiration 2 seconds and expiration 3 seconds.
 is a column of neurons located in the ventrolateral region of the medulla The four cell groups of the VRG are the rostral nucleus retrofacialis, caudal nucleus retroambiguus, nucleus para-ambiguus, and the pre-Bötzinger complex. The VRG contains both inspiratory and expiratory neurons. Most researchers feel that the VRG is secondarily responsible for initiation of inspiratory activity, after the dorsal respiratory group. New thought is that the VRG may be the primary rhythm –generating and integrative center. New theory feels that the cyclic on/off switch between the inspiratory and expiratory neurons in the VRG – produce inhalation and exhalation – also setting the frequency at 12 – 15 breaths per minute – inspiration 2 seconds and expiration 3 seconds.")
84
Which ever nuclei that initiates inspiration (VRG or DRG) – its actions are a steady increase in action firing frequency, leading to contraction of the respiratory muscles. The impulses travel down the phrenic and intercostal nerves to stimulate the diaphragm and external intercostal muscles. The rhythmic intermittent spontaneous firing of the DRG (or VRG) produces a normal respiratory rate of breaths per minute in humans. Inspiration usually lasts approximately 2 seconds, and expiration lasts about 3 seconds (I/E ratio earlier discussed) . The normal inspiration rate and rhythm is called eupnea.
 produces a normal respiratory rate of breaths per minute in humans. Inspiration usually lasts approximately 2 seconds, and expiration lasts about 3 seconds (I/E ratio earlier discussed) . The normal inspiration rate and rhythm is called eupnea.")
85
Pneumotaxic Center The pneumotaxic center, also known as the pontine respiratory group (PRG), is a network of neurons in the rostral dorsal lateral pons. The PRG antagonizes the DRG and VRG cyclically inhibiting the depth of inspiration. The PRG limits the burst of action potentials in the phrenic nerve, effectively decreasing the tidal volume and regulating the respiratory rate. Absence of the PRG results in an increase in depth of respiration and a decrease in respiratory rate.
, is a network of neurons in the rostral dorsal lateral pons. The PRG antagonizes the DRG and VRG cyclically inhibiting the depth of inspiration. The PRG limits the burst of action potentials in the phrenic nerve, effectively decreasing the tidal volume and regulating the respiratory rate. Absence of the PRG results in an increase in depth of respiration and a decrease in respiratory rate.")
86
Apneustic Center Controversy as to if it exists in the human – if it does it is located in the lower pons as appears to promote inspiration by stimulation of the neurons in the medulla oblongata – (VRG and DRG).
.")
87
Figure 22.24

88
Control of Respiratory Rhythm
According to recent research – the VRG (earlier thought was the DRG) has pacemaker cells that spontaneously but intermittently fire a cluster of action potentials initiating inspiration. However, if these neurons are suppressed – that does not abolish breathing – thus it is felt that normal respiratory rhythm is a result of reciprocal inhibition of the interconnected neuronal networks in the medulla Other theories include Inspiratory neurons are pacemakers and have intrinsic automaticity and rhythmicity Stretch receptors in the lungs establish respiratory rhythm
 has pacemaker cells that spontaneously but intermittently fire a cluster of action potentials initiating inspiration. However, if these neurons are suppressed – that does not abolish breathing – thus it is felt that normal respiratory rhythm is a result of reciprocal inhibition of the interconnected neuronal networks in the medulla. Other theories include. Inspiratory neurons are pacemakers and have intrinsic automaticity and rhythmicity. Stretch receptors in the lungs establish respiratory rhythm.")
89
Intercostal nerves Phrenic Nerve Figure 22.24

90
Chemoreceptors affecting Breathing
Central – located 1mm below the ventral medullary surface Peripheral – located in the aorta (aortic body) and the carotids (carotid body) Sensory input from aortic body via cranial nerve X (Vagus) goes into breathing centers (DRG) ; sensory input from the carotids travel via cranial nerve IX (glossopharyngeal) goes into same areas in the brain
 and the carotids (carotid body) Sensory input from aortic body via cranial nerve X (Vagus) goes into breathing centers (DRG) ; sensory input from the carotids travel via cranial nerve IX (glossopharyngeal) goes into same areas in the brain.")
91
Central chemoreceptors of the central nervous system, located on the ventrolateral medullary surface, are sensitive to the pH of their environment. These act to detect a change in pH of the cerebral spinal fluid (CSF) that are indicative of a change in oxygen or carbon dioxide concentration available to brain tissues. An increase in carbon dioxide tension of the arteries, often resulting from increased CO2 intake (hypercapnia) indirectly cause the blood to become more acidic; the cerebral spinal fluid pH is closely comparable to the plasma pH, as carbon dioxide easily diffuses across the blood/brain barrier. However, a change in plasma pH will not stimulate central chemoreceptors as H+ will not be able to diffuse into the CSF. Only CO2 levels affect this as it can diffuse across into the CSF, forming H+ and decreasing pH. Central chemoreception remains, in this way, distinct from peripheral chemoreceptors.
 that are indicative of a change in oxygen or carbon dioxide concentration available to brain tissues. An increase in carbon dioxide tension of the arteries, often resulting from increased CO2 intake (hypercapnia) indirectly cause the blood to become more acidic; the cerebral spinal fluid pH is closely comparable to the plasma pH, as carbon dioxide easily diffuses across the blood/brain barrier. However, a change in plasma pH will not stimulate central chemoreceptors as H+ will not be able to diffuse into the CSF. Only CO2 levels affect this as it can diffuse across into the CSF, forming H+ and decreasing pH. Central chemoreception remains, in this way, distinct from peripheral chemoreceptors.")
92
Central chemoreceptors are most sensitive to H+ but it has trouble going across the blood-brain barrier. CO2 easily transverses the BBB – then gets into CSF and interstitial fluids converting to carbonic acid which dissociates to H+ and HCO3-. Thus the H+ gets in indirectly based on the concentration of CO2. Thus CO2 is the main stimulus for breathing – except in those with longstanding Chronic Obstructive Pulmonary Disease (COPD) where O2 is the main stimulus for breathing. With constant high levels of CO2 the chemoreceptors decrease sensitivity to CO2.
 where O2 is the main stimulus for breathing. With constant high levels of CO2 the chemoreceptors decrease sensitivity to CO2..")
93
Depth and Rate of Breathing
Inspiratory depth is determined by how actively the respiratory center stimulates the respiratory muscles Rate of respiration is determined by how long the inspiratory center is active Respiratory centers in the pons and medulla are sensitive to both excitatory and inhibitory stimuli

94
Sensory Inputs that affect Breathing
Figure 22.25

95
Depth and Rate of Breathing: Reflexes
1. Pulmonary irritant reflexes – irritants promote reflexive constriction of air passages (via Vagus) 2. Inflation reflex (Hering-Breuer) – stretch receptors in the lungs are stimulated by lung inflation Upon inflation, inhibitory signals are sent to the medullary inspiration center to end inhalation and allow expiration
 2. Inflation reflex (Hering-Breuer) – stretch receptors in the lungs are stimulated by lung inflation. Upon inflation, inhibitory signals are sent to the medullary inspiration center to end inhalation and allow expiration.")
96
Depth and Rate of Breathing: Higher Brain Centers (Non-homeostatic)
Hypothalamic (Emotional) controls act through the limbic system to modify rate and depth of respiration Example: breath holding that occurs in anger A rise in body temperature acts to increase respiratory rate Cortical controls are direct signals from the cerebral motor cortex that bypass medullary controls Examples: voluntary breath holding, taking a deep breath
 controls act through the limbic system to modify rate and depth of respiration. Example: breath holding that occurs in anger. A rise in body temperature acts to increase respiratory rate. Cortical controls are direct signals from the cerebral motor cortex that bypass medullary controls. Examples: voluntary breath holding, taking a deep breath.")
97
Figure 22.26

98
Hyperventilation Hyperventilation – increased depth and rate of breathing that results in drop in the PaCO2: Quickly flushes carbon dioxide from the blood Can physiologically occur in in response to hypercapnia Though a rise CO2 acts as the original stimulus, control of breathing at rest is regulated by the hydrogen ion concentration in the brain A dramatic non-physiologic (anxiety) drop in PaCO2 can cause vasoconstriction in the brain – thus fainting (re-breath through paper bag)
 drop in PaCO2 can cause vasoconstriction in the brain – thus fainting (re-breath through paper bag)")
99
Depth and Rate of Breathing: PCO2
Hypoventilation – slow and shallow breathing due to abnormally low PCO2 levels Apnea (breathing cessation) may occur until PCO2 levels rise
 may occur until PCO2 levels rise.")
100
Depth and Rate of Breathing: PCO2
Arterial oxygen levels are monitored by the aortic and carotid bodies Substantial drops in arterial PO2 (to 60 mm Hg) are needed before oxygen levels become a major stimulus for increased ventilation If carbon dioxide is not removed (e.g., as in emphysema and chronic bronchitis), chemoreceptors become unresponsive to PCO2 chemical stimuli In such cases, PO2 levels become the principal respiratory stimulus (hypoxic drive)
 are needed before oxygen levels become a major stimulus for increased ventilation. If carbon dioxide is not removed (e.g., as in emphysema and chronic bronchitis), chemoreceptors become unresponsive to PCO2 chemical stimuli. In such cases, PO2 levels become the principal respiratory stimulus (hypoxic drive)")
101
Depth and Rate of Breathing: Arterial pH
Changes in arterial pH can modify respiratory rate even if carbon dioxide and oxygen levels are normal Increased ventilation in response to falling pH is mediated by peripheral chemoreceptors

102
Peripheral Chemoreceptors
act most importantly to detect variation of the oxygen in the arterial blood, in addition to detecting arterial carbon dioxide and pH. These nodes, called the aortic body and carotid body, are located on the arch of the aorta and on the common carotid artery, respectively. The carotids bodies are most sensitive to changes in partial pressure of arterial oxygen and pH. The aortic bodies are most sensitive to the content of arterial oxygen. A continual signal is sent, via cranial nerves IX and X, from the peripheral chemoreceptors Figure 22.27

103
See Acid Base PowerPoint

104
Respiratory Adjustments: Exercise
Respiratory adjustments are geared to both the intensity and duration of exercise During vigorous exercise: Ventilation can increase 20 fold Breathing becomes deeper and more vigorous, but respiratory rate may not be significantly changed (hyperpnea) Exercise-enhanced breathing is not prompted by an increase in PCO2 or a decrease in PO2 or pH These levels remain surprisingly constant during exercise – PaCO2 may even decrease and PaO2 increase
 Exercise-enhanced breathing is not prompted by an increase in PCO2 or a decrease in PO2 or pH. These levels remain surprisingly constant during exercise – PaCO2 may even decrease and PaO2 increase.")
105
Respiratory Adjustments: Exercise
As exercise begins: Ventilation increases abruptly, rises slowly, and reaches a steady state When exercise stops: Ventilation declines suddenly, then gradually decreases to normal

106
Respiratory Adjustments: Exercise
Neural factors bring about the above changes, including: Psychic stimuli Cortical motor activation Excitatory impulses from proprioceptors in muscles

107
Post - Exercise It appears that the blood gases are normal post exercise along with ventilatory functions It appears that the lactic acid buildup in muscles is not due to failure to get enough oxygen into the blood – but (1) inadequate cardiac output to pump the blood at the higher exercise rate and (2) inadequate vasculature in the skeletal muscles. Thus increasing the intake of O2 as seen by athletes after performance does not do anything since the blood is already saturated with enough oxygen.
 inadequate cardiac output to pump the blood at the higher exercise rate and (2) inadequate vasculature in the skeletal muscles. Thus increasing the intake of O2 as seen by athletes after performance does not do anything since the blood is already saturated with enough oxygen.")
108
Respiratory Adjustments: High Altitude
The body responds to quick movement to high altitude (above 8000 ft) with symptoms of acute mountain sickness – headache, shortness of breath, nausea, and dizziness
 with symptoms of acute mountain sickness – headache, shortness of breath, nausea, and dizziness.")
109
Respiratory Adjustments: High Altitude
Acclimatization – respiratory and hematopoietic adjustments to altitude include: Increased ventilation – 2-3 L/min higher than at sea level Chemoreceptors become more responsive to PCO2 Substantial decline in PO2 stimulates peripheral chemoreceptors

110
See Respiratory Diseases PowerPoint

111
Chronic Obstructive Pulmonary Disease (COPD)
Exemplified by chronic bronchitis and obstructive emphysema Patients have a history of: Smoking Dyspnea, where labored breathing occurs and gets progressively worse Coughing and frequent pulmonary infections COPD victims develop respiratory failure accompanied by hypoxemia, carbon dioxide retention, and respiratory acidosis

112
Pathogenesis of COPD Figure 22.28

113
Asthma Characterized by dyspnea, wheezing, and chest tightness Active inflammation of the airways precedes bronchospasms Airway inflammation is an immune response caused by release of IL-4 and IL-5, which stimulate IgE and recruit inflammatory cells Airways thickened with inflammatory exudates magnify the effect of bronchospasms

114
Tuberculosis Infectious disease caused by the bacterium Mycobacterium tuberculosis Symptoms include fever, night sweats, weight loss, a racking cough, and splitting headache Treatment entails a 12-month course of antibiotics

115
Accounts for 1/3 of all cancer deaths in the U.S.
Lung Cancer Accounts for 1/3 of all cancer deaths in the U.S. 90% of all patients with lung cancer were smokers The three most common types are: Squamous cell carcinoma (20-40% of cases) arises in bronchial epithelium Adenocarcinoma (25-35% of cases) originates in peripheral lung area Small cell carcinoma (20-25% of cases) contains lymphocyte-like cells that originate in the primary bronchi and subsequently metastasize
 arises in bronchial epithelium. Adenocarcinoma (25-35% of cases) originates in peripheral lung area. Small cell carcinoma (20-25% of cases) contains lymphocyte-like cells that originate in the primary bronchi and subsequently metastasize.")
116
Developmental Aspects
Olfactory placodes invaginate into olfactory pits by the 4th week Laryngotracheal buds are present by the 5th week Mucosae of the bronchi and lung alveoli are present by the 8th week

117
Developmental Aspects
By the 28th week, a baby born prematurely can breathe on its own During fetal life, the lungs are filled with fluid and blood bypasses the lungs Gas exchange takes place via the placenta

118
Respiratory System Development
Figure 22.29

119
Developmental Aspects
At birth, respiratory centers are activated, alveoli inflate, and lungs begin to function Respiratory rate is highest in newborns and slows until adulthood Lungs continue to mature and more alveoli are formed until young adulthood Respiratory efficiency decreases in old age

Similar presentations










 & CARBONDIOXIDE(CO2)>")












