Download presentation
Presentation is loading. Please wait.

1
FDG-PET in Aggressive Lymphoma Chen Shih-Wei, SKH

2
Nuclear medicine has a well-established role in the management of malignant lymphomas. 67 Ga-Citrate has been widely used for the evaluation of HD and NHL. Many studies have proved FDG-PET is superior to Gallium scan for both initial staging and follow-up of lymphoma. J Nucl Med 2006; 47:1326–1334 The Role of NM in Lymphoma

3
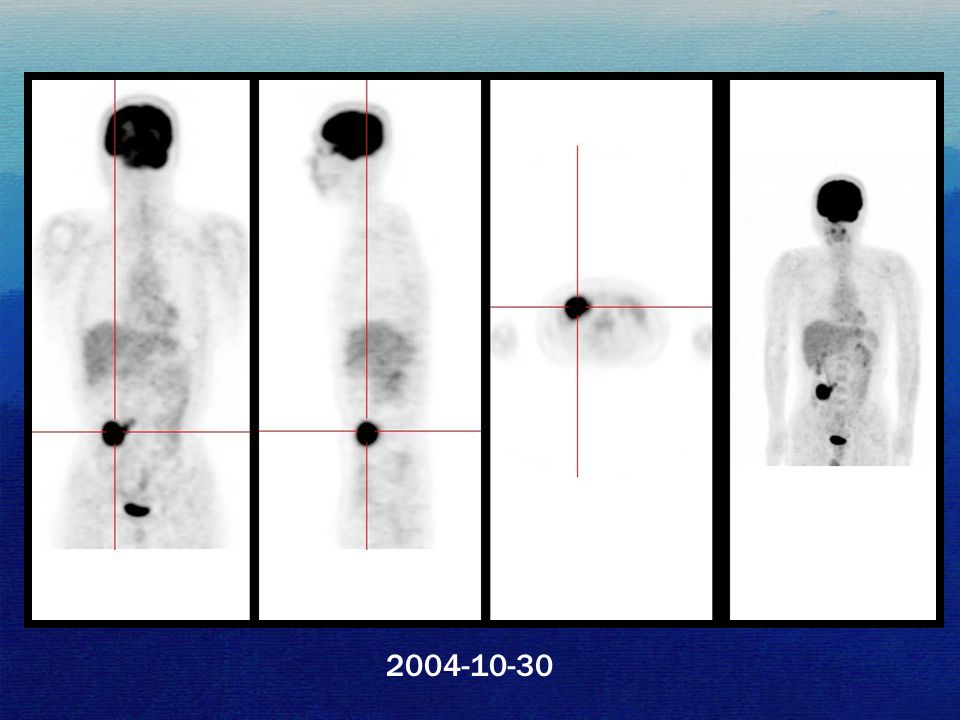
Case 1 36 y/o male PET for cancer screening on 2004-10-30 No specific complaint

4
2004-10-30
8
max SUV: 18.1 4.2 x 3.5 x 3.4 cm

9
D/D Colon cancer ? Small intestine cancer ? Gastrointestinal stromal tumor ? Castleman’s disease Lymphoma ?

11
He received operation at NTUH: Mesentery lymphoma, Diffuse large B cell type. Chemotherapy (Jan to May, 2005) Result
 Result.")
12
2006-8-12

13
DLBL Diffuse large B-cell lymphoma (DLBL) is a type of aggressive lymphoma. It accounts for approximately 40% of lymphomas among adults.

14
Initial Staging Evaluate response of treatment Follow-up (detect recurrence) The Role of PET in Lymphoma
 The Role of PET in Lymphoma")
15
J of Nucl Med, 2006;47(8): 1326-1334
:")
16
(29.7%) (24.4%) (27.3%) (7.0%) (4.1%) (1.2%) (2.9%) (1.2%) (0.6%) Blood, 15 May 2003, Vol. 101, No. 10, pp. 3875-3876

17
Utility of FDG-PET Scanning in Lymphoma 172 patients with lymphoma. Diffuse large B-cell lymphoma ( LBCL; n=51, 29.7% ) Hodgkin lymphoma (HL; n=47, 27.3%) Follicular lymphoma (FL; n=42, 24.4%) Marginal zone lymphoma (MZL; n=12, 7%) Mantle cell lymphoma (MCL; n=7, 4%) Peripheral T-cell lymphoma (PTCL; n=5, 2.9%) Blood, 15 May 2003, Vol. 101, No. 10, pp. 3875-3876
 Hodgkin lymphoma (HL; n=47, 27.3%) Follicular lymphoma (FL; n=42, 24.4%) Marginal zone lymphoma (MZL; n=12, 7%) Mantle cell lymphoma (MCL; n=7, 4%) Peripheral T-cell lymphoma (PTCL; n=5, 2.9%) Blood, 15 May 2003, Vol. 101, No. 10, pp")
18
FDG-PET detected disease in at least one site in 161 patients (94%) and failed to detect disease in 11 patients (6%). 100% of patients with LBCL and MCL and in 98% of patients with HL and FL. In contrast, FDG-PET detected disease in only 67% of MZL and 40% of PTCL. Blood, 15 May 2003, Vol. 101, No. 10, pp. 3875-3876

19
Table. Positive rate of FDG-PET in T/NK-cell neoplasms Annals of Oncology 18: 1685 -1690, 2007

20
The Role of PET in Lymphoma Many studies revealed overlap between the SUVs of indolent and aggressive lymphomas. Generally, aggressive disease had a higher FDG uptake than indolent lymphomas. J Nucl Med 2006; 47:1326–1334

21
Case 2 62 y / o female Right parotid cancer (adenoid cystic carcinoma) s / p operation and radiotherapy in 2001 PET for follow up examination on 2004-1-15
 s / p operation and radiotherapy in 2001 PET for follow up examination on")
22
2004-1-15

23
Diffusely increased FDG uptake in bilateral thyroid lobes, more intense on the right side. Possibly due to chronic thyroiditis.

24
2005-7-14

25
2005-08-20 Ultrasound: Multinodular goiter 2006-10-27 Ultrasound: Multinodular goiter

26
(2005-07-24) Thyroglobulin : 66.3 (2005-08-20) US: Multinodular goiter (2006-10-27) US: Multinodular goiter (2006-12-12) T3, T4, TSH: Normal Thyroglobulin : 102.3 (2007-04-11) TSH: 0.008 Thyroglobulin : 80.5 (2007-07-02) TSH: 0.013 Thyroglobulin : 45.7
 Thyroglobulin : 66.3 ( ) US: Multinodular goiter ( ) US: Multinodular goiter ( ) T3, T4, TSH: Normal Thyroglobulin : ( ) TSH: Thyroglobulin : 80.5 ( ) TSH: Thyroglobulin : 45.7")
27
2007-11-5

28
2004-1-15 2005-7-14 2007-11-5 max SUV: 4.5 max SUV: 5.8 max SUV: 64.1

29
D/D Papillary cancer ? Medullary cancer ? Anaplastic cancer ? Thyroid Lymphoma ? Anaplastic cancer ?

30
( 2007-11-23 ) US: MNG, right > left. FNA : Negative for malignancy ( 2007-12-10 ) FNA : Atypical cell present Malignancy still cannot be ruled out, so she received operation on 96-12-14.
 FNA : Atypical cell present Malignancy still cannot be ruled out, so she received operation on")
31
Result Right total thyroidectomy: - Diffuse large B cell lymphoma - Lymphocytic thyroiditis Left near total thyroidectomy: - Lymphocytic thyroiditis Right neck LNs dissection: - Negative for malignancy = Hashimoto’s thyroiditis

32
Thyroid Lymphoma Rare: about 2 % of extranodal lymphomas & < 5 % of all thyroid cancers. Typically found in older woman. Almost always B-cell lineage. Large cell type predominance ( 70–80 %). The main ones are diffuse large B-cell lymphoma and MALT lymphoma. Thyroid Cancer, 2nd Edition, 2007, p615-623 J of Clin Oncol, 2007 ASCO, Vol.25, No.18S
. The main ones are diffuse large B-cell lymphoma and MALT lymphoma. Thyroid Cancer, 2nd Edition, 2007, p J of Clin Oncol, 2007 ASCO, Vol.25, No.18S.")
33
Thyroid Lymphoma About half limited to the thyroid gland (stage IE). Pre-existing Hashimoto’s thyroiditis is the only known risk factor (about 60 -fold relative risk). Thyroid gland enlarges rapidly, compressive symptoms. Diagnosis is made by fine-needle aspiration. Thyroid Cancer, 2nd Edition, 2007, p615-623 J of Clin Oncol, 2007 ASCO, Vol.25, No.18S
. Thyroid gland enlarges rapidly, compressive symptoms. Diagnosis is made by fine-needle aspiration. Thyroid Cancer, 2nd Edition, 2007, p J of Clin Oncol, 2007 ASCO, Vol.25, No.18S.")
34
Hashimoto’s thyroiditis & Thyroid Lymphoma The cause has not been adequately explained. One potential mechanism may be the result of chronic antigenic stimulation in thyroiditis, enhancing the probability of neoplastic transformation.

35
FDG-PET in Thyroid Cancer Well-differentiated cancers can trap radioiodine, but not FDG. Poorly differentiated cancers show avid uptake of FDG, but they do not tend to trap iodine. When showing focal high FDG uptake should be regarded as a possible malignancy that needs further assessment. Thyroid Cancer, 2nd Edition, 2007, p639 In Vivo. 2008 Jan-Feb;22(1):109-14
:")
36
Bilateral Thyroid FDG Uptake Bilateral thyroidal uptake of FDG could be normal variants and subjects with various thyroid disorders Diffuse intense uptake and higher SUV levels are a clue to a diagnosis of chronic thyroiditis, especially for those with hypothyroidism. Focally intense uptake suggests the possibility of a thyroid carcinoma. Nucl Med Commun; 2007; 28:117–122

37
Case 3 26 y/o female. Right shoulder mass with swelling. Biopsy on 2006-7-15 : - Shoulder: Lymphoma, diffuse large type - iliac crest: Negative for malignancy PET scan on 2006-7-26.

38
2006-7-26

41
S/P chemotherapy with CHOP x 6 courses. Follow-up PET on 2006-12-21.

42
2006-12-21

44
Bone Marrow Involve Bone marrow involvement in patients with lymphoma is considered a sign of less favorable prognosis. Bone marrow biopsy (BMB) represents the standard diagnostic procedure. However, BMB has a high rate of false-negative, which may lead to errors in management.
 represents the standard diagnostic procedure. However, BMB has a high rate of false-negative, which may lead to errors in management..")
45
PET in Detecting Bone Marrow Involvement 78 patients (NHL= 39, HD= 39 ) Sensitivity= 81 %, Specificity= 100 % for detecting bone marrow disease, with only 4 cases not being seen on PET. J of Clin Oncol, 1998; 16: 603-609 75710478 8 patients were confirmed and 2 cases remained unresolved.

46
PET vs. BMB Blood, 15 May 2003, Vol. 101, No. 10, pp. 3875-3876 Total777516105

47
J of Nucl Med, 2005;46(6): 958-963 504493553587 Sensitivity Specificity HD (191) NHL (191) Both/not separable (121) 76% 92% 43% 88% 52% 97% PET vs. BMB 76.2% High Grade 30.2% Low Grade 13 studies, 587 patients Total51% 91%

48
5335245 SKH, from 2001 to 2008 High grade lymphomaLow grade lymphoma

49
Hodgkin lymphoma; bone involve & biopsy(-) 2004-9-14 2004-8-11 2004-9-15 Ga ScanBone Scan
 Ga ScanBone Scan")
50
83y, F, Diffuse large B Cell Lymphoma; bone involve & biopsy(-)
")
51
77y, M, Diffuse large B Cell Lymphoma; bone involve & biopsy(-) 2008-5-30 2008-5-26
")
52
PET has good, but not excellent for the detection of bone marrow infiltration of lymphoma. PET may complement the results of BMB. Its performance may vary according to the type of lymphoma. PET vs. BMB

53
Post-C/T Marrow Hyperplasia Marrow hyperplasia as a consequence of recovery from a chemotherapeutic insult may also cause a generalized increase in FDG uptake in marrow. This increased uptake generally returns to baseline levels by 1 mo (usually within 3 wk), suggesting that clinicians should wait at least 1 mo after completion of therapy before obtaining a PET scan. J of Nucl Med, 2006;47(8): 1326-1334
, suggesting that clinicians should wait at least 1 mo after completion of therapy before obtaining a PET scan. J of Nucl Med, 2006;47(8):")
54
FIGURE 1. Pretherapy (A) and posttherapy (B) PET scans of patient with Burkitt's lymphoma involving multiple vertebrae (arrows). Follow-up scan demonstrates diffuse bone marrow uptake secondary to administration of growth factor, with decreased uptake seen in areas of previous bone marrow involvement.
 and posttherapy (B) PET scans of patient with Burkitt s lymphoma involving multiple vertebrae (arrows). Follow-up scan demonstrates diffuse bone marrow uptake secondary to administration of growth factor, with decreased uptake seen in areas of previous bone marrow involvement..")
55
Conclusion Many studies concluded that aggressive diseases had a higher FDG uptake than indolent lymphomas. The role of FDG-PET is not to make a specific diagnosis but to determine the stage and response to treatment. PET cannot replace BMB but may complement it, esp. in the aggressive type.

56
J Nucl Med 2006; 47:1326–1334

57
~ the End ~

58
Kunishima S et al., Clini Nucl Med 2001:26:789-790 Castleman’s disease

59
Blockmans D et al., CLINI NUCL MED 2001:26:975-976 Castleman’s disease

60
Blockmans D et al., CLINI NUCL MED 2001:26:975-976 Castleman’s disease

Similar presentations


















 AND HODGKIN LYMPHOMA (HL) Figure.>")


>")




