Download presentation
Presentation is loading. Please wait.

1
Multivariate analyses in clinical populations: General factors & neuroimaging Joseph Callicott, MD fMRI/MRI Summer Course 6/20/14

2
Introduction The ‘Age of Big Data’ Lohr, “GOOD with numbers? Fascinated by data? The sound you hear is opportunity knocking…” (NY Times, 2/22/2012) We routinely collect ‘multimodal data’ E.g., mood rating scale and structural MRI Compile or compare, but typically without multimodal analysis Projects classified as ‘geno-,’ ‘proteo-,’ or ‘pheno-’ already connotes ‘big data:’ Each fMRI image presents ~20K analyses GWAS model = strict correction for multiple comparisons Current model = parallel correlation/association per dataset Proposed model = multivariate approach w/data reduction Simplified analyses Smaller statistical ‘cost’ Some current theoretical approaches become testable’ (RDoC)
 We routinely collect ‘multimodal data’ E.g., mood rating scale and structural MRI Compile or compare, but typically without multimodal analysis Projects classified as ‘geno-,’ ‘proteo-,’ or ‘pheno-’ already connotes ‘big data:’ Each fMRI image presents ~20K analyses GWAS model = strict correction for multiple comparisons Current model = parallel correlation/association per dataset Proposed model = multivariate approach w/data reduction Simplified analyses Smaller statistical ‘cost’ Some current theoretical approaches become testable’ (RDoC).")
3
Outline A Tale of Two Lectures: I. Imaging genetics & schizophrenia I. Relevant issues for clinical populations II. Why imaging genetics? III. Imaging genetics 101 IV. Multivariate analyses of fMRI: within experimental dataset II. General vs specific factors in data I. g II. “i” : factor analytic solution of general factors in fMRI task data III. Multivariate analyses of fMRI redux: across experimental dataset

4
Issues of special interest to clinical studies… BOLD fMRI in clinical populations: BOLD fMRI is not, strictly speaking, a clinically informative measure No pathognomic findings, to date Performance likely to differ fundamentally in tasks that HVs will perform near ceiling I.e., ~100% accuracy and faster RT than patients BOLD fMRI in healthy subjects ‘predictive relationships’ between behavior and BOLD implicit in design, perhaps not strongly correlated with group map activation Genetic associations to BOLD (the bulk of the imaging genetics literature) do not necessarily connote a ‘real’ effect of a given polymorphism Is the phenotype heritable? In past, twin or sibling studies Currently, within ‘only’ HV = GCTA (Visscher) (Callicott et. al. 2000; Manoach et al., 2000; Callicott et al. 2003; others) (Van Snellenberg et al. 2006)
 (Callicott et. al. 2000; Manoach et al., 2000; Callicott et al. 2003; others) (Van Snellenberg et al. 2006).")
5
So, then, why imaging genetics? Crass commercial message: o Simple plan, high impact o Have an fMRI task in a relatively large sample? o Healthy controls preferable o N > 40 o Draw blood or swab cheek o Genotyping at most resolutions fast & cheap* o In SPM: ANCOVA or regression suffice and seem reasonably powered COMT led from primate to human imaging, and then to drugs targeting cognitive impairments

6
Seriously, though, why imaging genetics? o Few routes to neural mechanism using in vivo human data o Animal model o Drug study o BOLD fMRI (MRSI, MEG, EEG) o Genes do not code for mental illness, per se o Genes code for heritable aspects of brain function, intermediate- or endo- phenotypes o Genetic risk for illnesses like schizophrenia is polygenic, heterogeneous o Gene interact with each other and the environment o BOLD fMRI, as an alternate metric of specific or general cognitive systems, offers ‘real world validation’ o Putative genetic mutations (including private mutations (CNVs) o In spite of growing sample sizes, association studies risk false positives o RDoC domains and constructs o If these do not correspond to brain systems we can map, then may be as doomed as DSM
 o Genes do not code for mental illness, per se o Genes code for heritable aspects of brain function, intermediate- or endo- phenotypes o Genetic risk for illnesses like schizophrenia is polygenic, heterogeneous o Gene interact with each other and the environment o BOLD fMRI, as an alternate metric of specific or general cognitive systems, offers ‘real world validation’ o Putative genetic mutations (including private mutations (CNVs) o In spite of growing sample sizes, association studies risk false positives o RDoC domains and constructs o If these do not correspond to brain systems we can map, then may be as doomed as DSM.")
7
Take home message… Larger samples needed (GWAS), typically via collaboration across centers (ENIGMA) BIG DATA is here Multivariate or non-hypothesis- driven analyses offer the potential for novel, highly informative findings CNV & cognition Very good software often freely available: PLINK AFNI GingerALE-SLEUTH-MANGO R (many) (Stefansson et al., Nature, 2014)
, typically via collaboration across centers (ENIGMA) BIG DATA is here Multivariate or non-hypothesis- driven analyses offer the potential for novel, highly informative findings CNV & cognition Very good software often freely available: PLINK AFNI GingerALE-SLEUTH-MANGO R (many) (Stefansson et al., Nature, 2014)")
8
(*Visscher et al., 2010; Nan et al. 2012**; Postuma et al. 2002***; McGue & Bouchard, 1998#;^Burmeister et al., 2008)
.")
9
Interest in imaging genetics predicated on heritability of phenotypes… Callicott et al. Cereb Cortex 2000 Patients > Controls (N=13) (N=18) Callicott et al. Am J Psychiatry 2003 Healthy Siblings > Controls (N=48) (N=33) PFC BOLD during our Nback h2 = 0.4-0.5 Blokland et al. Biol Psych 2009, J Neurosci 2011; Koten et al. Science 2009
 (N=18) Callicott et al. Am J Psychiatry 2003 Healthy Siblings > Controls (N=48) (N=33) PFC BOLD during our Nback h2 = Blokland et al. Biol Psych 2009, J Neurosci 2011; Koten et al. Science")
10
Finding genes for highly heritable, but complex diseases affected person unaffected “nonpenetrant” (Goldman et al. Nat Rev Genet 2006) Remains difficult, even when n=100K 1.Caused by many (100-1000s) of genes 2.The effects of a mutation vary between people Has all the genes (note this doesn’t mean the exact same set) May still carry some genes (like a parent of a sick person) Has all of the genes but is NOT sick for reasons we can’t explain
 Remains difficult, even when n=100K 1.Caused by many ( s) of genes 2.The effects of a mutation vary between people Has all the genes (note this doesn’t mean the exact same set) May still carry some genes (like a parent of a sick person) Has all of the genes but is NOT sick for reasons we can’t explain.")
11
Catechol O-methyltransferase (COMT): NIMH Intramural Success Story (Apud et al. 2006) (Egan et al. 2001) (Meyer-Lindenberg et al. 2006)
 (Egan et al. 2001) (Meyer-Lindenberg et al. 2006).")
12
Functional impact COMT Val 105/158 Met val/met rs4680 5’ Now validated at multiple levels: Animal models: Reduced enzymatic activity Altered synaptic dopamine levels Human data: Reduced enzymatic activity in vitro lymphoblastoid cell lines Altered transcription/reduced activity post mortem Altered D1 but not D2 receptor density in PFC PFC efficiency in BOLD fMRI Combined: Sex effects mostly in males ((Papaleo et al., 2014) striatum mammalian PFC
 striatum mammalian PFC")
13
genotype effect F=5.41, df= 2, 449; p<.005. Executive cognition Effect of rs4680 on frontal lobe function (Egan et al PNAS 2001) n = 218 n = 181 n = 58 vv>vm>mm, SPM 99, p vm>mm, SPM 99, p<.005 Physiological efficiency Circa 2014: How have these findings held up? Replicated but n’s ~20
 n = 218 n = 181 n = 58 vv>vm>mm, SPM 99, p vm>mm, SPM 99, p<.005 Physiological efficiency Circa 2014: How have these findings held up. Replicated but n’s ~20.")
14
BOLD phenotypes in simple association: COMT and PFC 14 (Mier, Kirsch, Meyer-Lindenberg; 2009)
")
15
BOLD phenotypes in simple association: 5-HTTP and Amygdala 15 (Munafo, Brown, and Hariri; 2007))
)")
16
BOLD phenotypes in simple association: Power? 16 (Barnett et al, 2008)
")
17
1 st generation imaging genetics: simple association o Candidate genes o KIBRA impaired memory & expressed in hippocampus (Papassotiropoulos et al., Science 2006) o Replication in 3 independent populations in behavioral memory measures o In 30 healthy subjects, KIBRA associated with reduced hippo activation
 o Replication in 3 independent populations in behavioral memory measures o In 30 healthy subjects, KIBRA associated with reduced hippo activation")
18
o Genetic mutations modeled in cell culture or animals o Association based on disease GWAS (ZNF804A) o Esslinger et al. 2009 (Science) o Rasetti et al. (Arch Gen Psychiatry) 2 nd generation imaging genetics: GWAS era
 o Rasetti et al. (Arch Gen Psychiatry) 2 nd generation imaging genetics: GWAS era.")
19
PFC neuronal function: ‘optimized’ by dopamine & GABA interactions (Goldman-Rakic & Selemon 1997) (Seamans et al., 2001) 2 nd generation imaging genetics: Epistasis and pathways
 (Seamans et al., 2001) 2 nd generation imaging genetics: Epistasis and pathways")
20
(Straub et al., 2007) 2 nd generation imaging genetics: Epistasis
 2 nd generation imaging genetics: Epistasis")
21
COMT : V/VV/ M M/ M Bray Hap: - /- +/- V/ V V/ M M/ M V/ V V/MM/M +/++/+ +/++/+ +/++/+ BOLD fMRI Left DLPFC (a.u.) COMT x Dysbindin interaction o Epistasis (gene-gene interaction) o Initially based on candidate-by-candidate o Buckholtz et al., Mol Psychiatry 2007 o Data-driven (machine learning) o Nicodemus et al., Hum Genet 2010 o Now predicated on detailed cellular or animal modeling o COMT x DTNBP1 (Papaleo et al., 2013) o DISC1 x NKCC1 (Kim et al., Cell 2012 & Callicott et al. J Clin Invest 2013) 2 nd generation imaging genetics: Translational neuroscience
 2 nd generation imaging genetics: Translational neuroscience.")
22
22 More of the same (‘sophisticated univariate’)? Network/connectivity? Hypothesis-free? Hypothesis-free pattern detection (random forest) ICA/PCA/CPCA networks Next generation imaging genetics? Novel phenotypes (processing speed)
 ICA/PCA/CPCA networks Next generation imaging genetics. Novel phenotypes (processing speed).")
23
Sophisticated univariate: Imaging GWAS o BOLD fMRI GWAS o Nback (n = 364) o Illumina 650K chip genotyping o Automated extraction of AAL ROIs o First GWAS + using BOLD fMRI (Callicott, Spencer, et al., in prep)
 o Illumina 650K chip genotyping o Automated extraction of AAL ROIs o First GWAS + using BOLD fMRI (Callicott, Spencer, et al., in prep)")
24
As a heritable trait, BOLD fMRI phenotypes show other sensitivities….. o Long history within animal literature showing significant effects of environment on brain structure & function o Beneficial effects of ‘enrichment’ (toys, limit isolation) (Hebb, Am J Psychiatry, 1955) o fMRI during social stress task influenced by environment o Urban upbringing or urbanicity linked to increased risk for mental illness (Van Os et al., Nature, 2010) (Lederbogen et al., Nature, 2012) Sophisticated univariate: Novel questions
 (Hebb, Am J Psychiatry, 1955) o fMRI during social stress task influenced by environment o Urban upbringing or urbanicity linked to increased risk for mental illness (Van Os et al., Nature, 2010) (Lederbogen et al., Nature, 2012) Sophisticated univariate: Novel questions.")
25
As a heritable trait, BOLD fMRI phenotypes show other sensitivities….. o fMRI during WM ( 3 cohorts (USA1 = 124; USA2 =92; Italy1=226 ) o Sensitivity to childhood environment (Urbanicity) (Ihne et al., in submission) Sophisticated univariate: Imaging G x E
 o Sensitivity to childhood environment (Urbanicity) (Ihne et al., in submission) Sophisticated univariate: Imaging G x E.")
26
o fMRI during WM ( 3 cohorts (USA1 = 124; USA2 =112; Italy1=226 ) o Gene-by-environment interaction (COMT x Urbanicity) (Ihne et al., in submission) Ihne et al., in preparation Sophisticated univariate: Imaging G x E
 o Gene-by-environment interaction (COMT x Urbanicity) (Ihne et al., in submission) Ihne et al., in preparation Sophisticated univariate: Imaging G x E")
27
Constrained principle component analysis (CPCA) (David AA Baranger – Wash U) 27 http://www.nitrc.org/projects/fmricpca Todd Woodward and colleagues, University of British Columbia: CPCA provides a “unified framework [for]… regression analysis and principal component analysis.” To identify functional systems using from singular-value decomposition of BOLD time series, These systems are imaged by constraining analyzed BOLD signal from a particular interval of time against all other scans (i.e., all others are baseline) Multivariate network analysis: ICA/PCA/CPCA banish ‘blob-ology’
![Constrained principle component analysis (CPCA) (David AA Baranger – Wash U) 27 Todd Woodward and colleagues, University of British Columbia: CPCA provides a unified framework [for]… regression analysis and principal component analysis. To identify functional systems using from singular-value decomposition of BOLD time series, These systems are imaged by constraining analyzed BOLD signal from a particular interval of time against all other scans (i.e., all others are baseline) Multivariate network analysis: ICA/PCA/CPCA banish ‘blob-ology’](http://images.slideplayer.com/12/3390609/slides/slide_27.jpg "Constrained principle component analysis (CPCA) (David AA Baranger – Wash U) 27 Todd Woodward and colleagues, University of British Columbia: CPCA provides a unified framework [for]… regression analysis and principal component analysis. To identify functional systems using from singular-value decomposition of BOLD time series, These systems are imaged by constraining analyzed BOLD signal from a particular interval of time against all other scans (i.e., all others are baseline) Multivariate network analysis: ICA/PCA/CPCA banish ‘blob-ology’")
28
CPCA 28 Z or ‘activation’ matrix = individual time series for all subjects (rows) for all voxels in the brain (columns) Our standard SPM5 via XNAT first level processing of 0B alternating with 2B G or ‘design’ matrix = a model to predict BOLD signal changes (columns) over all fMRI scans (rows) SPM5 often uses a canonical hemodynamic response function (HRF) to deconvolve signal, fMRI-CPCA uses finite impulse response function (FIR) http://www.nitrc.org/projects/fmricpca
 for all voxels in the brain (columns) Our standard SPM5 via XNAT first level processing of 0B alternating with 2B G or ‘design’ matrix = a model to predict BOLD signal changes (columns) over all fMRI scans (rows) SPM5 often uses a canonical hemodynamic response function (HRF) to deconvolve signal, fMRI-CPCA uses finite impulse response function (FIR)")
29
CPCA 29 N-back model not complicated: Simply provide onset and offset of 0B and 2B task epochs Components = extracted components represent networks Component loadings= loosely, correlation coefficients between component scores and BOLD signal that was predicted from imposed constraints (design) http://www.nitrc.org/projects/fmricpca
")
30
30 Identify and then display components using MRICon for anatomical localization (http://www.nitrc.org/projects/mricron)http://www.nitrc.org/projects/mricron In this case, not really using estimated hemodynamics Rather, we wish to compare effect of diagnosis or genotype using component scores and predictor weights Predictor weight = contribution of G matrix to changes in components over the fMRI time series (~ correlation of component score and g) CPCA
 CPCA")
31
CPCA: Confusing Problematic Conflicting Agonizing Unspecified error required recalculation of component weights Same networks found with addition of a fourth DMN Differentiates NC and SIBs from SCZ No longer appears to be identifying intermediate phenotype

32
CPCA: Nback systems Anti-task Network resembles cingulate from DMN + hippocampus WM Network DLPFC +parietal Motor system Anti-task #2 resembles parietal From DMN + cerebellum

33
CPCA: Factors sensitive to disease, not genetics p<0.05 Unspecified error required recalculation of component weights Same networks found with addition of a fourth DMN Differentiates NC and SIBs from SCZ No longer appeared to identify intermediate phenotype

34
CPCA: Not particularly sensitive in general 420 HV CPCA (2back) = 4 factors Neuro- = 6 cognitive factors 2B as measured in lab g estimates
 = 4 factors Neuro- = 6 cognitive factors 2B as measured in lab g estimates")
35
Big data benefits reproducibility…

36
ENIGMA: first GWAS+ sMRI (Stein et al. 2009, 2010; Thompson et al., 2014) Big data benefits reproducibility… Heritability for novel phenesReplication on large scale
 Big data benefits reproducibility… Heritability for novel phenesReplication on large scale.")
37
Outline A Tale of Two Lectures: I. Imaging genetics & schizophrenia I. Why imaging genetics? II. Imaging genetics 101 III. Multivariate analyses of fMRI: within experimental dataset II. General vs specific factors in data I. g II. “i” : factor analytic solution of general factors in fMRI task data III. Multivariate analyses of fMRI redux: across experimental dataset

38
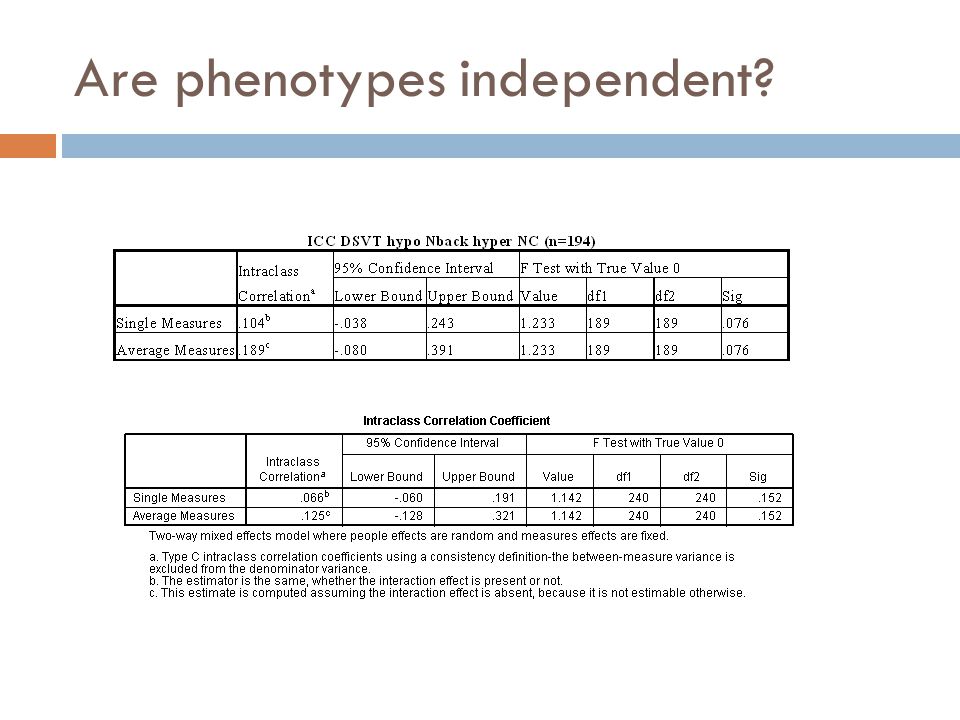
Are phenotypes independent?

41
The general cognitive factor (Spearman’s g) (Dickinson et al., 2008)(Jensen, 1998)
 (Dickinson et al., 2008)(Jensen, 1998)")
42
Where is g? ‘Lesion maps’ from 241 patients w/ focal brain damage and g (Gläscher et al. PNAS 2010). Barbey et al. (Brain 2012) found similar results in 182 focal brain lesion patients Various conceptual, functional and structural support for PFC and PAR (at minimum)
. Barbey et al. (Brain 2012) found similar results in 182 focal brain lesion patients Various conceptual, functional and structural support for PFC and PAR (at minimum).")
43
Is g associated with fMRI activation? Nback (n= 161) higher g greater efficiency Replication (n= 582) higher g greater efficiency Exact overlap Notes: 1.Analysis: SPM5 multiple regression controlling for age, sex 2.2B accuracy g (r = 0.3, p < 0.001)
 higher g greater efficiency Replication (n= 582) higher g greater efficiency Exact overlap Notes: 1.Analysis: SPM5 multiple regression controlling for age, sex 2.2B accuracy g (r = 0.3, p < 0.001).")
44
Replication…cont’d Replication 3 (n= 211) Areas within replication exactly overlapping discovery… discovery Replication 5 (n= 306) Replication 4 (n= 393) Replication 4 Replication 3 Replication 5
 Areas within replication exactly overlapping discovery… discovery Replication 5 (n= 306) Replication 4 (n= 393) Replication 4 Replication 3 Replication 5")
45
DSVT v g But… Faces v g MTL v g

46
g correlates with similar areas across 4 tasks in same 161 HVs Nback (n= 161) Notes: 1.Analysis: SPM5 multiple regression controlling for age, sex 2.161 with QC+ NB, MTL, Faces, DSVT 3.NB as discovery ROI, others queried at p < 0.05
 Notes: 1.Analysis: SPM5 multiple regression controlling for age, sex with QC+ NB, MTL, Faces, DSVT 3.NB as discovery ROI, others queried at p < 0.05")
47
Is there a general solution for fMRI? 161 HVs with QC+ Nback, MTL (incidental encoding), Faces (response to aversive faces), and DSVT (processing speed) Individual 1 st level maps created for each task Sue Tong: automated script to extract parameter estimates in Automated Anatomical Labeling (AAL) ROIs Mean fMRI ‘signal” transformed to Z score Factor analysis: Principle component extraction Orthogonal and oblique rotations Factor scores estimated i (fMRI g) = sum of factor scores Comparison across task and against cognitive measures (big g)
, Faces (response to aversive faces), and DSVT (processing speed) Individual 1 st level maps created for each task Sue Tong: automated script to extract parameter estimates in Automated Anatomical Labeling (AAL) ROIs Mean fMRI ‘signal transformed to Z score Factor analysis: Principle component extraction Orthogonal and oblique rotations Factor scores estimated i (fMRI g) = sum of factor scores Comparison across task and against cognitive measures (big g).")
48
i F1 Motor (R) Operculum (13) Cingulate (32) SMA (R) Postcentral Superior temporal gyrus (41,42) Middle temporal gyrus (motion) F2 Insula Caudate Putamen Pallidum F3 Cuneus (18) Sup Occipital (19/7) Mid Occipital (39 & 19/37) Inf Occipital (V5/MT) F4 Cerebellum (8-9) Cerebellar vermis F7 SFG (8/9/6) (R) MFG (R) IFG (44/45) (R) Angular (R) (39) F6 SFG (8/9/6) (L) Medial SFG (8) Ant Cingulate (24,32) Mid Cingulate (24,31) F5 MFG (L) Sup Parietal (7) Inf Parietal (40) Supramarginal (40) fMRI (Nback) i (161 HVs, max likelihood extraction w/ varimax rotation, 60.1% total variance explained, goodness-of-fit p < 1e-5).50.41.40.42.26.42.30.13.11.13.16.10
 Operculum (13) Cingulate (32) SMA (R) Postcentral Superior temporal gyrus (41,42) Middle temporal gyrus (motion) F2 Insula Caudate Putamen Pallidum F3 Cuneus (18) Sup Occipital (19/7) Mid Occipital (39 & 19/37) Inf Occipital (V5/MT) F4 Cerebellum (8-9) Cerebellar vermis F7 SFG (8/9/6) (R) MFG (R) IFG (44/45) (R) Angular (R) (39) F6 SFG (8/9/6) (L) Medial SFG (8) Ant Cingulate (24,32) Mid Cingulate (24,31) F5 MFG (L) Sup Parietal (7) Inf Parietal (40) Supramarginal (40) fMRI (Nback) i (161 HVs, max likelihood extraction w/ varimax rotation, 60.1% total variance explained, goodness-of-fit p < 1e-5)")
49
fMRI (Nback) i F7 SFG (8/9/6) (R) MFG (R) IFG (44/45) (R) Angular (R) (39) SFG (R) MFG (R) IFG (R) Angular (R) (161 HVs, max likelihood extraction w/ varimax rotation, 60.1% total variance explained, goodness-of-fit p < 1e-5).79.90.59.54.7.36.43.56.52.27
 i F7 SFG (8/9/6) (R) MFG (R) IFG (44/45) (R) Angular (R) (39) SFG (R) MFG (R) IFG (R) Angular (R) (161 HVs, max likelihood extraction w/ varimax rotation, 60.1% total variance explained, goodness-of-fit p < 1e-5)")
50
i F1 Motor (R) Operculum (13) Cingulate (32) SMA (R)F Postcentral Superior temporal gyrus (41,42) Middle temporal gyrus (motion) F2 Insula Caudate Putamen Pallidum F3 Cuneus (18) Sup Occipital (19/7) Mid Occipital (39 & 19/37) Inf Occipital (V5/MT) F4 Cerebellum (8-9) Cerebellar vermis F7 SFG (8/9/6) (R) MFG (R) IFG (44/45) (R) Angular (R) (39) F6 SFG (8/9/6) (L) Medial SFG (8) Ant Cingulate (24,32) Mid Cingulate (24,31) F5 MFG (L) Sup Parietal (7) Inf Parietal (40) Supramarginal (40) fMRI (Nback) i
 Operculum (13) Cingulate (32) SMA (R)F Postcentral Superior temporal gyrus (41,42) Middle temporal gyrus (motion) F2 Insula Caudate Putamen Pallidum F3 Cuneus (18) Sup Occipital (19/7) Mid Occipital (39 & 19/37) Inf Occipital (V5/MT) F4 Cerebellum (8-9) Cerebellar vermis F7 SFG (8/9/6) (R) MFG (R) IFG (44/45) (R) Angular (R) (39) F6 SFG (8/9/6) (L) Medial SFG (8) Ant Cingulate (24,32) Mid Cingulate (24,31) F5 MFG (L) Sup Parietal (7) Inf Parietal (40) Supramarginal (40) fMRI (Nback) i")
51
i F1 Sup Occipital (7) Mid Occipital (39 & 19/37) Inf Occipital (V5/MT) Fusiform (37, FFA) F2 Calcarine (17/18) Cuneus (18, V2) Lingual (19, V3) F3 Premotor MFG (R) IFG (44/45) (R) Sup Parietal (7) Inf Parietal (L) (40) F4 Hippocampus Parahippocampus Amygdala Inf Temporal (L) (IT) F6 Cerebellum (1) Cerebellum (6) F5 SFG (8/9/6) MFG (L) Medial SFG (8) fMRI (Faces) i (161 HVs, max likelihood extraction w/ varimax rotation, 58.1 % total variance explained, goodness-of-fit p < 1e-5).44.40.45.40.39.41.10
 Mid Occipital (39 & 19/37) Inf Occipital (V5/MT) Fusiform (37, FFA) F2 Calcarine (17/18) Cuneus (18, V2) Lingual (19, V3) F3 Premotor MFG (R) IFG (44/45) (R) Sup Parietal (7) Inf Parietal (L) (40) F4 Hippocampus Parahippocampus Amygdala Inf Temporal (L) (IT) F6 Cerebellum (1) Cerebellum (6) F5 SFG (8/9/6) MFG (L) Medial SFG (8) fMRI (Faces) i (161 HVs, max likelihood extraction w/ varimax rotation, 58.1 % total variance explained, goodness-of-fit p < 1e-5)")
52
fMRI (Faces) i i F1 Sup Occipital (7) Mid Occipital (39 & 19/37) Inf Occipital (V5/MT) Fusiform (37, FFA) F2 Calcarine (17/18) Cuneus (18, V2) Lingual (19, V3) F3 Premotor MFG (R) IFG (44/45) (R) Sup Parietal (7) Inf Parietal (L) (40) F4 Hippocampus Parahippocampus Amygdala Inf Temporal (L) (IT) F6 Cerebellum (1) Cerebellum (6) F5 SFG (8/9/6) MFG (L) Medial SFG (8)
 i i F1 Sup Occipital (7) Mid Occipital (39 & 19/37) Inf Occipital (V5/MT) Fusiform (37, FFA) F2 Calcarine (17/18) Cuneus (18, V2) Lingual (19, V3) F3 Premotor MFG (R) IFG (44/45) (R) Sup Parietal (7) Inf Parietal (L) (40) F4 Hippocampus Parahippocampus Amygdala Inf Temporal (L) (IT) F6 Cerebellum (1) Cerebellum (6) F5 SFG (8/9/6) MFG (L) Medial SFG (8)")
53
i F1 Orbitofrontal (47) Operculum (13) Insula Suparmarginal (L) (40) Sup temporal (41,42) Mid temporal (TG) F2 SFG (8/9/6) MFG IFG (44/45) Med SFG (8) Ant Cing (24/32) Mid Cing (24/31) F3 Hippocampus Parahippocampus Amygdala Caudate Putamen Pallidum Thalamus F4 Inf Occipital Fusiform Sup Cerebellum F6 Calcarine (17/18) Cuneus (18, V2) Lingual (19, V3) Sup Occipital (7) F5 Inf Cerbellum fMRI (DSVT) i (161 HVs, max likelihood extraction w/ varimax rotation, 51.6 % total variance explained, goodness-of-fit p < 1e-5).40.41.42.41.40.41.10
 Operculum (13) Insula Suparmarginal (L) (40) Sup temporal (41,42) Mid temporal (TG) F2 SFG (8/9/6) MFG IFG (44/45) Med SFG (8) Ant Cing (24/32) Mid Cing (24/31) F3 Hippocampus Parahippocampus Amygdala Caudate Putamen Pallidum Thalamus F4 Inf Occipital Fusiform Sup Cerebellum F6 Calcarine (17/18) Cuneus (18, V2) Lingual (19, V3) Sup Occipital (7) F5 Inf Cerbellum fMRI (DSVT) i (161 HVs, max likelihood extraction w/ varimax rotation, 51.6 % total variance explained, goodness-of-fit p < 1e-5)")
54
fMRI (DSVT) i i F1 Orbitofrontal (47) Operculum (13) Insula Suparmarginal (L) (40) Sup temporal (41,42) Mid temporal (TG) F2 SFG (8/9/6) MFG IFG (44/45) Med SFG (8) Ant Cing (24/32) Mid Cing (24/31) F3 Hippocampus Parahippocampus Amygdala Caudate Putamen Pallidum Thalamus F4 Inf Occipital Fusiform Sup Cerebellum F6 Calcarine (17/18) Cuneus (18, V2) Lingual (19, V3) Sup Occipital (7) F5 Inf Cerbellum
 i i F1 Orbitofrontal (47) Operculum (13) Insula Suparmarginal (L) (40) Sup temporal (41,42) Mid temporal (TG) F2 SFG (8/9/6) MFG IFG (44/45) Med SFG (8) Ant Cing (24/32) Mid Cing (24/31) F3 Hippocampus Parahippocampus Amygdala Caudate Putamen Pallidum Thalamus F4 Inf Occipital Fusiform Sup Cerebellum F6 Calcarine (17/18) Cuneus (18, V2) Lingual (19, V3) Sup Occipital (7) F5 Inf Cerbellum")
55
i F1 Calcarine (17/18) Cuneus (18, V2) Lingual (19, V3) Sup Occipital (7) Mid Occipital (39 & 19/37) Inf Occipital (V5/MT) Fusiform (37, FFA) Inf Temporal (R) (IT) F2 Caudate Putamen Pallidum Thalamus F3 SFG (8/9/6) MFG Angular (R) (39) F4 Insula Sup Temporal (TG) Mid Temporal (R) (TG) F6 Precentral (L) IFG (44/45) IFG (45/46) Postcentral (L) Sup Parietal (L) (7) Inf Parietal (L) (40) Supramarginal (L) (40) F5 Hippocampus Parahippocampus Inf Temporal (L) (IT) fMRI (MTL) i (161 HVs, max likelihood extraction w/ varimax rotation, 51.6 % total variance explained, goodness-of-fit p < 1e-5).40.41.42.41.40.41.10
 Cuneus (18, V2) Lingual (19, V3) Sup Occipital (7) Mid Occipital (39 & 19/37) Inf Occipital (V5/MT) Fusiform (37, FFA) Inf Temporal (R) (IT) F2 Caudate Putamen Pallidum Thalamus F3 SFG (8/9/6) MFG Angular (R) (39) F4 Insula Sup Temporal (TG) Mid Temporal (R) (TG) F6 Precentral (L) IFG (44/45) IFG (45/46) Postcentral (L) Sup Parietal (L) (7) Inf Parietal (L) (40) Supramarginal (L) (40) F5 Hippocampus Parahippocampus Inf Temporal (L) (IT) fMRI (MTL) i (161 HVs, max likelihood extraction w/ varimax rotation, 51.6 % total variance explained, goodness-of-fit p < 1e-5)")
56
fMRI (MTL) i i F1 Calcarine (17/18) Cuneus (18, V2) Lingual (19, V3) Sup Occipital (7) Mid Occipital (39 & 19/37) Inf Occipital (V5/MT) Fusiform (37, FFA) Inf Temporal (R) (IT) F2 Caudate Putamen Pallidum Thalamus F3 SFG (8/9/6) MFG Angular (R) (39) F4 Insula Sup Temporal (TG) Mid Temporal (R) (TG) F6 Precentral (L) IFG (44/45) IFG (45/46) Postcentral (L) Sup Parietal (L) (7) Inf Parietal (L) (40) Supramarginal (L) (40) F5 Hippocampus Parahippocampus Inf Temporal (L) (IT)
 i i F1 Calcarine (17/18) Cuneus (18, V2) Lingual (19, V3) Sup Occipital (7) Mid Occipital (39 & 19/37) Inf Occipital (V5/MT) Fusiform (37, FFA) Inf Temporal (R) (IT) F2 Caudate Putamen Pallidum Thalamus F3 SFG (8/9/6) MFG Angular (R) (39) F4 Insula Sup Temporal (TG) Mid Temporal (R) (TG) F6 Precentral (L) IFG (44/45) IFG (45/46) Postcentral (L) Sup Parietal (L) (7) Inf Parietal (L) (40) Supramarginal (L) (40) F5 Hippocampus Parahippocampus Inf Temporal (L) (IT)")
57
An i by any other name… gFaces iNback iDSVT iMTL i g Pearson Correlation 1-.060.042-.025-.210 ** Sig. (1-tailed).226.300.378.004 Faces i Pearson Correlation -.0601-.182 * -.027.014 Sig. (1-tailed).226.010.365.428 Nback i Pearson Correlation.042-.182 * 1.056-.049 Sig. (1-tailed).300.010.241.267 DSVT i Pearson Correlation -.025-.027.0561.124 Sig. (1-tailed).378.365.241.059 MTL i Pearson Correlation -.210 **.014-.049.1241 Sig. (1-tailed).004.428.267.059 **. Correlation is significant at the 0.01 level (1-tailed). *. Correlation is significant at the 0.05 level (1-tailed).
 Faces i Pearson Correlation * Sig. (1-tailed) Nback i Pearson Correlation * Sig. (1-tailed) DSVT i Pearson Correlation Sig. (1-tailed) MTL i Pearson Correlation ** Sig. (1-tailed) **. Correlation is significant at the 0.01 level (1-tailed). *. Correlation is significant at the 0.05 level (1-tailed)..")
58
Structural MRI (351 HVs, max likelihood extraction w/ varimax rotation, 48 % total variance explained, goodness-of-fit p < 1e-5)
")
59
Summary: i F1 Calcarine (17/18) Cuneus (18, V2) Lingual (19, V3) Sup Occipital (7) Mid Occipital (39 & 19/37) Inf Occipital (V5/MT) Fusiform (37, FFA) Inf Temporal (R) (IT) F2 Caudate Putamen Pallidum Thalamus F3 SFG (8/9/6) MFG Angular (R) (39) F4 Insula Sup Temporal (TG) Mid Temporal (R) (TG) F6 Precentral (L) IFG (44/45) IFG (45/46) Postcentral (L) Sup Parietal (L) (7) Inf Parietal (L) (40) Supramarginal (L) (40) F5 Hippocampus Parahippocampus Inf Temporal (L) (IT) A Tale of Two Lectures: I. Imaging genetics & schizophrenia I. Imaging genetics easier in an age of data sharing and public databases II. BOLD fMRI (IMHO) has never been about diagnosis = hello RDoC! III. Multivariate analyses of fMRI: novel findings, novel questions II. General vs specific factors in data I. g inspires a straight-forward, replicable multivariate analysis of fMRI (Factor analytic approach) (Dickinson et al., Biol Psych 2008; JAMA Psych 2014, numerous) II. “i” : factor analytic solution of general factors in fMRI task data III. Multivariate analyses of fMRI redux: I. Data reduction writ large II. Replication across tasks, labs, designs?
 has never been about diagnosis = hello RDoC. III. Multivariate analyses of fMRI: novel findings, novel questions II. General vs specific factors in data I. g inspires a straight-forward, replicable multivariate analysis of fMRI (Factor analytic approach) (Dickinson et al., Biol Psych 2008; JAMA Psych 2014, numerous) II. i : factor analytic solution of general factors in fMRI task data III. Multivariate analyses of fMRI redux: I. Data reduction writ large II. Replication across tasks, labs, designs .")
60
Further musing… Multimodal data, multimodal analysis fMRI phenotypes are not independent Aspects within each task representing individual ‘positive manifold’ Is heritability about this general shared variance or specific task aspects? FMRI i as a data reduction method Not g Complicated, but factor solution may be informed by other data Structural MRI factor solution, no relationship to g or other cognitive factors g holds special relationship to fMRI data Test whether reduced factor structure more related to genes, other MRI, clinical measures i F1 Calcarine (17/18) Cuneus (18, V2) Lingual (19, V3) Sup Occipital (7) Mid Occipital (39 & 19/37) Inf Occipital (V5/MT) Fusiform (37, FFA) Inf Temporal (R) (IT) F2 Caudate Putamen Pallidum Thalamus F3 SFG (8/9/6) MFG Angular (R) (39) F4 Insula Sup Temporal (TG) Mid Temporal (R) (TG) F6 Precentral (L) IFG (44/45) IFG (45/46) Postcentral (L) Sup Parietal (L) (7) Inf Parietal (L) (40) Supramarginal (L) (40) F5 Hippocampus Parahippocampus Inf Temporal (L) (IT)
 Cuneus (18, V2) Lingual (19, V3) Sup Occipital (7) Mid Occipital (39 & 19/37) Inf Occipital (V5/MT) Fusiform (37, FFA) Inf Temporal (R) (IT) F2 Caudate Putamen Pallidum Thalamus F3 SFG (8/9/6) MFG Angular (R) (39) F4 Insula Sup Temporal (TG) Mid Temporal (R) (TG) F6 Precentral (L) IFG (44/45) IFG (45/46) Postcentral (L) Sup Parietal (L) (7) Inf Parietal (L) (40) Supramarginal (L) (40) F5 Hippocampus Parahippocampus Inf Temporal (L) (IT).")
61
Thanks: Dwight Dickinson Sue Tong Jessica Ihne Karen Berman Barbara Spencer Graham Baum Morgan Bartholomew Amanda Zheutlin CTNB clinical staff

Similar presentations












 from China Wang et al. PNAS Feb. 11, 2008.>")







