Download presentation
Presentation is loading. Please wait.

1
Avances en el tratamiento del Cáncer de Pulmón Lugar de la Angiogénesis en el tratamiento de segunda linea del CPCNP Carlos Camps Inducing angiogenesis Hanahan D and Weinberg RA. Cell 2011;144:646-47.

2
Precision lung cancer care BSC 2–4 months Plat based 6–8 months Targeted therapies Plat doublets 8–10 months

4
4 Ligands are structurally related molecules. VEGFA, VEGFB, PlGF: variety of isoforms Expression of the VEGF family is tightly regulated by host factors and epigenetics signal in the tumor microenvironmet VEGFR-2 mediate almost all of the known cellular responses to VEGF VEGFR-1 modulate VEGFR-2 signaling, sequestering VEGFA Role in mobilization of progenitors from BM VEGFR-3 mediates lymphangiogenesis NRP-1 facilitate the presentation and binding of VEGF to its receptor. Adapted from Kerbel RS. N Engl J Med. 2008. Epigenetic Induction Hypoxia, cytokines, sex hormones, growth factors, chemokines Genetic Component

5
5 ANGIOGENESIS: ANGIOGENESIS: redundant and complex

6
6 66 Proximal splice siteDistal splice site Renner, et al Future Oncol 2009 VEGFA: isoforms NRP-1 binding region Post-transcriptional control Pro-angiogenicAnti-angiogenic Regulation of the splicing ??

8
Numerous anti-angiogenic agents have failed to show a survival benefit in advanced NSCLC StudyInterventionTargetPFS, monthsOS, months Primary endpoint ESCAPE 1 (n=926) CB/PTX/placebo CB/PTX/sorafenib VEGFR-2, -3, PDGFR-ß, Flt-3, b-RAF, c-kit 5.4 4.6 HR: 0.99 (0.84–1.16) 10.6 10.7 HR: 1.15 (0.94–1.41) OS NExUS 2 (n=772) CIS/GEM/placebo CIS/GEM/sorafenib 5.5 6.0 HR: 0.83 (0.71–0.97) 12.5 12.4 HR: 0.98 (0.83–1.16) OS ZEAL 3 (n=534) Pemetrexed/placebo Pemetrexed/vandetanib VEGFR-1,-2, -3, EGFR, RET 2.8 4.1 HR: 0.86 (0.69–1.06) 9.2 10.5 HR: 0.86 (0.65–1.13) PFS ZODIAC 4 (n=1391) Docetaxel/placebo Docetaxel/vandetanib 3.2 4.0 HR: 0.79 (0.70–0.90) 10.0 10.6 HR: 0.91 (0.78–1.07) PFS SUN1087 5 (n=960)* Erlotinib/placebo Erlotinib/sunitinib VEGFR-1, -2, -3, PDGFR-ɑ, -ß, Flt- 3, c-kit 2.0 3.6 HR: 0.81 (0.70–0.94) 8.5 9.0 HR: 0.92 (0.80–1.07) OS VITAL 6 (n=913) Docetaxel/placebo Docetaxel/afliberceptVEGF-A, -B, PIGF 4.1 5.2 HR: 0.82 (0.72–0.94) 10.4 10.1 HR: 1.01 (0.87–1.17) OS BETA 7 (n=636) Erlotinib/placebo Erlotinib/bevacizumabVEGF-A 1.7 3.4 HR: 0.62 (0.52–0.75) 9.2 9.3 HR: 0.97 (0.80–1.18) OS First line Second line *280 patients received >1 prior treatment lines. CB = carboplatin; PTX = paclitaxel; CIS = cisplatin; GEM = gemcitabine; OS = overall survival; PFS = progression-free survival; HR = hazard ratio; VEGF = vascular endothelial growth factor receptor; PDGFR = platelet-derived growth factor receptor; RAF = rapidly accelerated fibrosarcoma; PIGF = placental growth factor receptor. 1. Scagliotti G, et al. J Clin Oncol 2010;28:1835–42; 2. Paz-Ares LG, et al. J Clin Oncol 2012;30:3084–92; 3. de Boer R, et al. J Clin Oncol 2011;29:1067–74; 4. Herbst R, et al. Lancet Oncol 2010;11:619–26; 5. Scagliotti GV, et al. J Clin Oncol 2012;30:2070–8; 6. Ramlau R, et al. J Clin Oncol 2012;30:3640–7; 7. Herbst R, et al. Lancet Oncol 2011;377:1846–54.

9
Targeted Approaches to Anti-VEGF Therapy Anti-receptor- blocking antibodies Anti-ligand-blocking antibodies Tyrosine kinase inhibitors Bevacizumab Nintedanib Ramucirumab VEGF VEGFR Howewer …..We do not know what is the best way to run Avastin

10
Rationale for Anti-VEGF Therapy Vascular leakiness result in decreased flow to some areas of tumor and increased pressure in tumors – Decrease access of drugs, immune cells – Result in hypoxia, which induces tumor progression and decreases efficacy of drugs that require oxygen, and low pH Antiangiogenic therapy targeting VEGF or VEGFR may restore a more normal vasculature, generating an environment less favorable to cancer cell growth Vascular leakiness result in decreased flow to some areas of tumor and increased pressure in tumors – Decrease access of drugs, immune cells – Result in hypoxia, which induces tumor progression and decreases efficacy of drugs that require oxygen, and low pH Antiangiogenic therapy targeting VEGF or VEGFR may restore a more normal vasculature, generating an environment less favorable to cancer cell growth Weinmann M, et al. Onkologie. 2004;27:83-90 [2] ; Goel S, et al. Physiol Rev. 2011;91:1071-1121. [26] Decreased drug delivery (and hence resistance) and increased tumor hypoxia. Another mechanism of antiangiogenic therapy is attenuation of vascular hyperpermeability, increasing vessel pericyte coverage, and normalization of the basement membrane to reduced interstitial fluid pressure and improved blood perfusion. This normalization have consequences on drug and oxygen delivery and on the immune microenvironment
 and increased tumor hypoxia. Another mechanism of antiangiogenic therapy is attenuation of vascular hyperpermeability, increasing vessel pericyte coverage, and normalization of the basement membrane to reduced interstitial fluid pressure and improved blood perfusion. This normalization have consequences on drug and oxygen delivery and on the immune microenvironment.")
11
The mechanisms by which anti-VEGF therapy increases survival remain unclear – Anti-VEGF therapy led to a increase in plasma PlGF – High levels of soluble VEGFR1 before starting Bv - worse survival(biomarker of treatment resistance) – Reducing blood flow and permeability improved OS in patients with improved tumor vasculature and blood perfusion after treatment. – Excessive decreasing vascular permeability after Bv therapy negatively impact of combination therapy in NSCLC. – We have to examine the dose effect on tumor vasculature and treatment efficacy. Heist R et al, PNAS, 2015, 112 :1547–1552

12
Initial Cohort q<0.05 (VEGFR1) FLT1: rs9582036 Glubb, Jantus-Lewintre, et al, Clin Cancer Res, 2015, Submitted ANGIOMET I
 FLT1: rs Glubb, Jantus-Lewintre, et al, Clin Cancer Res, 2015, Submitted ANGIOMET I")
13
Huang Y, ProcNatl Acad Sci USA,2012,109:17561 Años Inmunoterapia Tratamientos dirigidos Supervivencia Antiangiogénicos Tratamiento Convencional/sintomático

14
Activation EGFR increases VEGF Inhibition EGFR decreases VEGF Resistence to inhibition EGFR is associated with enhanced VEGF leves(HGF/Met) Activation EGFR increases VEGF Inhibition EGFR decreases VEGF Resistence to inhibition EGFR is associated with enhanced VEGF leves(HGF/Met)
 Activation EGFR increases VEGF Inhibition EGFR decreases VEGF Resistence to inhibition EGFR is associated with enhanced VEGF leves(HGF/Met)")
16
Sato, JCO 2014, 15:1236-

17
BELIEF (MO29711): phase II study Sponsor: ETOP Primary objective – PFS Secondary objectives – OS – RR / Safety / QoL – Additional translational research (TBD) Previously untreated stage IIIb–IV non-squamous NSCLC EGFR mut+ (Ex19/21) ± T790M (n=102) Previously untreated stage IIIb–IV non-squamous NSCLC EGFR mut+ (Ex19/21) ± T790M (n=102) Erlotinib 150 mg po + bevacizumab 15 mg/Kg iv PD NCT01562028
: phase II study Sponsor: ETOP Primary objective – PFS Secondary objectives – OS – RR / Safety / QoL – Additional translational research (TBD) Previously untreated stage IIIb–IV non-squamous NSCLC EGFR mut+ (Ex19/21) ± T790M (n=102) Previously untreated stage IIIb–IV non-squamous NSCLC EGFR mut+ (Ex19/21) ± T790M (n=102) Erlotinib 150 mg po + bevacizumab 15 mg/Kg iv PD NCT")
18
Clinical scenarios for 2nd - line treatment: not all are created equal 1 st Line 2 nd Line PD 1 st Line 2 nd Line Follow-up PDOR/SD 1 st Line Maintenance 2 nd Line PDOR/SD OR=Objective response. SD=Stable Disease. PD=Progressive disease.

19
Continued treatment with anti-VEGF increases survival in murine xenograft Bagri, et al. Clin Cancer Res 2010 Preclinical data: the continued inhibition of VEGF provides maximum benefit 010203040506070 80 Animals remaining in study (%) 100 80 60 40 20 0 Time (days) Anti-VEGF Control Anti-VEGF x3 weeks Anti-VEGF EOS Median PFS Bev+Pem:10.2m Bev:6.6m HR: 0.50; p<0.001 0369121518 AVAPER AVAPERL L 1* Δ 3.6m PFS estimate 1. Barlesi, et al. EMCC 2011 1.0 0.8 0.6 0.4 0.2 0 *Investigator assessed
 Time (days) Anti-VEGF Control Anti-VEGF x3 weeks Anti-VEGF EOS Median PFS Bev+Pem:10.2m Bev:6.6m HR: 0.50; p< AVAPER AVAPERL L 1* Δ 3.6m PFS estimate 1. Barlesi, et al. EMCC *Investigator assessed.")
20
ATLAS 1:1 Unblind to PE Avastin + Tarceva until PE NSCLC quimionaïve N=1,160 4 cicles 1ªlíne + Avastin Non-PD n=768 (66%) Treatment post-progresión Avastin + Placebo until PE Main Objective: PFS
 Treatment post-progresión Avastin + Placebo until PE Main Objective: PFS")
21
PD: progression of disease *SOC2 (Standard of Care) Labelled agents for second-line treatment of NSCLC (erlotinib, pemetrexed and docetaxel) † SOC3 (Standard of Care) and beyond: Choice of labelled agents is the Investigator’s choice Bevacizumab dose must remain the same throughout the trial Primary endpoint: OS PD 1 SOC2* + bevacizumab SOC3† + bevacizumab SOC4 ± bevacizumab SOC2*SOC3 † SOC4 PD 3 PD 2 Estudio fase III randomizado para evaluar del uso continuado de bevacizumab en todas las líneas de tratamiento en CNMP Randomize 1:1 Stage IIIB/IV non-squamous NSCLC treated with platinum- doublet (4-6 cycles) + bevacizumab PLUS > 2 cycles of bevacizumab maintenance Gridelli et al. Clin Lung Cancer, 2011

22
BEYOND Secondary endpoints –ORR –OS –DoR and safety –PFS with Bev to 3rd PD Secondary endpoints –ORR –OS –DoR and safety –PFS with Bev to 3rd PD Phase III (double-blinded, multi-centre) study Zhou, et al. WCLC 2013 Carboplatin + paclitaxel + bevacizumab 15mg/kg q3w (up to 6 cycles) Carboplatin + paclitaxel + placebo q3w (up to 6 cycles) Locally advanced, metastatic or recurrent NSCLC first- line n=270 Locally advanced, metastatic or recurrent NSCLC first- line n=270 Primary endpoint –PFS Primary endpoint –PFS R 1:1 PD Bevacizumab* 15mg/kg q3w PD Placebo HR=0.40 (95% CI: 0.29–0.54) p<0.0001 PFS estimate 05101520 Time (months) 1.0 0.8 0.6 0.4 0.2 0 6.5 9.2 Carbo/Pac + Pl → Pl Carbo/Pac + Bev → Bev
 Carboplatin + paclitaxel + placebo q3w (up to 6 cycles) Locally advanced, metastatic or recurrent NSCLC first- line n=270 Locally advanced, metastatic or recurrent NSCLC first- line n=270 Primary endpoint –PFS Primary endpoint –PFS R 1:1 PD Bevacizumab* 15mg/kg q3w PD Placebo HR=0.40 (95% CI: 0.29–0.54) p< PFS estimate Time (months) Carbo/Pac + Pl → Pl Carbo/Pac + Bev → Bev.")
23
BEYOND: exploratory analysis in EGFR WT A total of 152 patients contributed tissue for biomarker analysis (n=85 Carbo/Pac + Bev; n=67 Carbo/Pac + Pl) – EGFR mut-pos rate was 27% in Carbo/Pac + Bev and 25% in Carbo/Pac + Pl patients No correlation was observed between EGFR mutation status and Bev efficacy – a similar degree of treatment benefit was seen for mut-pos and WT groups (mut-pos HR=0.27; 95% CI: 0.12–0.63; WT HR=0.33; 95% CI: 0.21–0.53) PFS (primary endpoint) 1.0 0.8 0.6 0.4 0.2 0.0 051015 Study month Carbo/Pac + Pl: EGFR WT Carbo/Pac + Bev: EGFR WT 5.6 8.3 Zhou, et al. WCLC 2013 HR=0.33; 95% CI: 0.21–0.53 PFS (primary endpoint) 1.0 0.8 0.6 0.4 0.2 0.0 051015 Study month 7.912.4 PFS (primary endpoint) Zhou, et al. WCLC 2013 Carbo/Pac + Pl: EGFR Mut+ Carbo/Pac + Bev: EGFR Mut+ HR=0.33; 95% CI: 0.21–0.53 A total of 152 patients contributed tissue for biomarker analysis (n=85 Carbo/Pac + Bev; n=67 Carbo/Pac + Pl) – EGFR mut-pos rate was 27% in Carbo/Pac + Bev and 25% in Carbo/Pac + Pl patients BEYOND: exploratory analysis in EGFR Mut+p
 Study month PFS (primary endpoint) Zhou, et al. WCLC 2013 Carbo/Pac + Pl: EGFR Mut+ Carbo/Pac + Bev: EGFR Mut+ HR=0.33; 95% CI: 0.21–0.53 A total of 152 patients contributed tissue for biomarker analysis (n=85 Carbo/Pac + Bev; n=67 Carbo/Pac + Pl) – EGFR mut-pos rate was 27% in Carbo/Pac + Bev and 25% in Carbo/Pac + Pl patients BEYOND: exploratory analysis in EGFR Mut+p.")
24
BEYOND: OS Zhou, et al. IASLC 2014 SG (ITT): 24.3 meses vs. 17.1 meses (HR=0.68, p=0.0154) SG (EGFR WT): 20.3 meses vs. 13.8 meses (HR= 0.57)
 SG (EGFR WT): 20.3 meses vs meses (HR= 0.57).")
25
Summary Bevacizumab plus erlotinib regimens are effective as maintenance treatment for advanced NSCLC in EGFR mutated patients Continuation maintenance therapy with bevacizumab can further extend survival Which is the best sequence of use of this drug? Remains unclear whether bevacizumab’s efficacy is dependent on the chemotherapeutic regimen used. POINTBREAK

26
Phase III CALGB 30607: Sunitinib as Switch Maintenance in Advanced NSCLC Stratification factors: ECOG PS (0 vs 1) Stage (IIIB vs IV) Prior use of bevacizumab (yes or no) Sex (male vs female) Primary endpoint: PFS 1:1 Chemo-naive advanced NSCLC ECOG PS 0-1 Non-PD 4 cycles of 1st-line platinum- based doublet* Placebo (n = 104) PD Sunitinib 37.5 mg/day (n = 106) PD Socinski MA, et al. Chicago Multidisciplinary Symposium in Thoracic Oncology 2014. Abstract 1. *Bevacizumab allowed but was discontinued with the fourth cycle. 1.0 0.8 0.6 0.4 0.2 0 Survival Probability Mos From Randomization 0306121824 2-sided log-rank P =.0005 Median PFS (95% CI) 4.3 (3.2-4.9) 2.6 (1.8-3.0) HR (95% CI) 0.61 (0.46-0.81) Ref Sunitinib Placebo Median OS, mos (95% CI): Sunitinib 11.7 (9.4-15.0); Placebo 11.7 (9.9-14.0) Effect independent of histology
 4.3 ( ) 2.6 ( ) HR (95% CI) 0.61 ( ) Ref Sunitinib Placebo Median OS, mos (95% CI): Sunitinib 11.7 ( ); Placebo 11.7 ( ) Effect independent of histology.")
27
Targeted Approaches to Anti-VEGF Therapy Anti-receptor- blocking antibodies Anti-ligand-blocking antibodies Tyrosine kinase inhibitors Bevacizumab Nintedanib Ramucirumab VEGF VEGFR VEGFs FGFs PDGFs Endothelial cells VEGFRs, FGFRs Pericytes PDGFRs Smooth muscle cells FGFRs, PDGFRs LigandsCell type/receptors Stimulation Nintedanib Triple angiokinase inhibitor oral agent Can be combined with chemotherapy Docetaxel / Pemetrexed Triple angiokinase inhibitor oral agent Can be combined with chemotherapy Docetaxel / Pemetrexed

28
Drug Target EGFRFGFRPDGFRVEGFVEGFR Axitinib β R-1, 2, 3 Bevacizumab* BMS-690514 Brivanib R-1 R-2 Cediranib α/βα/β R-1, 2, 3 Linifanib R-1, 2, 3 MGCD265 Motesanib R-1, 2, 3 Nintedanib R-1, 2, 3α/βα/β Pazopanib R-1, 3α/βα/β R-1, 2, 3 Sorafenib β R-2, 3 Sunitinib α/βα/β R-1, 2, 3 Vandetanib R-2, 3 Angiogenesis Inhibitors in NSCLC * Currently approved for first-line therapy of NSCLC, in combination with a platinum and taxane Ellis PM & Al-Saleh K. Critical Rev Onc/Hem. 2012;84:47-58.

29
LUME-Lung 1: Trial Design Reck M, et al. ASCO 2013. Patients with NSCLC who have failed first-line chemotherapy Oral nintedanib + Chemotherapy (docetaxel) Placebo + Chemotherapy (docetaxel) Primary endpoint: PFS Key secondary endpoint: OS Second-line treatment Randomization Number of docetaxel cycles not restricted Monotherapy with nintedanib/placebo allowed after ≥ 4 cycles
 Placebo + Chemotherapy (docetaxel) Primary endpoint: PFS Key secondary endpoint: OS Second-line treatment Randomization Number of docetaxel cycles not restricted Monotherapy with nintedanib/placebo allowed after ≥ 4 cycles.")
30
LUME-Lung 1: primary endpoint met – significantly longer PFS with the addition of nintedanib to docetaxel Independent central review in all patients (N=1134) Reck M, et al. Lancet Oncol 2014;15:143–155. 100 80 60 40 20 Probability of PFS (%) 024681012141618 Time (months) 0 No. at risk Nintedanib56529515557194310 Placebo56925011643212100 Nintedanib + docetaxel Placebo + docetaxel Median PFS (months)3.42.7 HR = 0.79 (95% CI: 0.68–0.92); p=0.0019
 Time (months) 0 No. at risk Nintedanib Placebo Nintedanib + docetaxel Placebo + docetaxel Median PFS (months) HR = 0.79 (95% CI: 0.68–0.92); p=")
31
LUME-Lung 1: PFS benefit consistent in major histologies Nintedanib + docetaxel Placebo + docetaxel Median PFS (months) 4.02.8 HR = 0.77 (95% CI: 0.62–0.96); p=0.0193 AdenocarcinomaSquamous cell carcinoma Nintedanib + docetaxel Placebo + docetaxel Median PFS (months) 2.92.6 HR = 0.77 (95% CI: 0.62–0.96); p=0.02 100 80 60 40 20 0 012345678910111213141516 Time (months) Probability of PFS (%) No. at risk: 277 285 150 129 86 70 32 28 13 12 1 1 1 1 0 0 Nintedanib Placebo 100 80 60 40 20 0 012345678910111213141516 Time (months) Probability of PFS (%) No. at risk: 240 247 122 101 59 36 22 13 5 8 3 1 2 0 1 0 Nintedanib Placebo 0 0 Reck M, et al. Lancet Oncol. 2014;15:143-55. Independent central review: by histology
 Probability of PFS (%) No. at risk: Nintedanib Placebo 0 0 Reck M, et al. Lancet Oncol. 2014;15: Independent central review: by histology.")
32
LUME-Lung 1: OS by Histology Adenocarcinoma subset Nintedanib + docetaxel (n = 655) Placebo + docetaxel (n = 659) Median, mo10.19.1 HR (95% CI)0.94 (0.83 to 1.05) P.2720 Reck M, et al. ASCO 2013. Nintedanib + docetaxel (n = 322) Placebo + docetaxel (n = 336) Median, mo12.610.3 HR (95% CI)0.83 (0.70 to 0.99) P.0359 All patients Probability of survival (%) 100 80 60 40 20 0 0 4 8 12 16 20 24 28 32 36
 Placebo + docetaxel (n = 336) Median, mo HR (95% CI)0.83 (0.70 to 0.99) P.0359 All patients Probability of survival (%)")
33
LUME-Lung 1: Characteristics Associated With Improved OS in Nintedanib-Treated Adenocarcinoma Patients CharacteristicHR (95% CI)P value Prior bevacizumab.241 Yes0.61 (0.31, 1.20) No0.85 (0.71, 1.01) Best response to first-line therapy.189 CR/PR/SD0.90 (0.73, 1.10) PD0.62 (0.41, 0.94) Time since start of first-line therapy.419 < 9 months0.75 (0.60, 0.92) ≥ 9 months0.89 (0.66, 1.19) Reck M, et al. ASCO 2013. CR = complete response; PD = progressive disease; PR = partial response; SD = stable disease

34
Mellemgaard A, et al. Eur J Cancer. 2013;49(suppl. 2):Abstract 3409 and oral presentation. Reck M, et al. Lancet Oncol. 2014;15:143-55. LUME-Lung 1: positive OS
:Abstract 3409 and oral presentation. Reck M, et al. Lancet Oncol. 2014;15: LUME-Lung 1: positive OS.")
35
LUME-Lung 1: Adverse Events of Special Interest Reck M, et al. ASCO 2013. Adverse Events, Grade ≥ 3 (incidence ≥ 1%) Adverse Events, All Grades (incidence ≥ 15%) Patients Reporting (%) Nintedanib + docetaxel Placebo + docetaxel
 Adverse Events, All Grades (incidence ≥ 15%) Patients Reporting (%) Nintedanib + docetaxel Placebo + docetaxel.")
36
Combination Therapy With Angiogenesis Inhibitors: First-Line vs Second-Line Outcomes a. Sandler A, et al. New Engl J Med. 2006;355:2542-2550. b. Reck M, et al. J Clin Oncol. 2013;31(suppl): LBAS011. OS (mo) LUME-Lung 1 (Adenocarcinoma subset) HR, 0.79; 95% CI, 0.67 to 0.92 P =.003 HR, 0.83; P =.0359 [a] [b]
: LBAS011. OS (mo) LUME-Lung 1 (Adenocarcinoma subset) HR, 0.79; 95% CI, 0.67 to 0.92 P =.003 HR, 0.83; P =.0359 [a] [b].")
37
37 ANGIOGENESIS: ANGIOGENESIS: Redundant and Complex

38
38 Angiogenic biomarkers related to the tumor and its microenvironment Sanmartin et al, ASCO 2012 Surg Oncol 2014 VEGF-A VEGF-B PlGF p = 0.019p = 0.003 OS (months) p = 0.048 OS (months) Low High Low High Risk Score (RS) = 3*PIGF + 3*VEFGA + 4*VEGFB
 p = OS (months) Low High Low High Risk Score (RS) = 3*PIGF + 3*VEFGA + 4*VEGFB")
39
39 RISK SCORE: Prognostic value Adjuvant CT B OS (months) OS No Adjuvant treatment Sanmartin et al, ASCO 2012
 OS No Adjuvant treatment Sanmartin et al, ASCO 2012")
40
Targeted Approaches to Anti-VEGF Therapy Anti-receptor- blocking antibodies Anti-ligand-blocking antibodies Tyrosine kinase inhibitors Bevacizumab Nintedanib Ramucirumab VEGF VEGFR

41
..if you don´t have any markers? Ramucirumab Ramucirumab is a human immunoglobulin G, subclass 1 monoclonal antibody that specifically binds to the extracellular domain of VEGF Receptor-2 with high affinity 1 This antibody blocks the binding of the VEGF ligand to VEGF Receptor-2 and inhibits VEGF-stimulated activation 1 Two completed Phase 1 studies of ramucirumab demonstrated safety and tolerability at clinically relevant doses, with preliminary evidence of clinical efficacy across various solid tumors 1,2 Over 3500 patients have been treated with ramucirumab in clinical studies 3 1.Spratlin et al. J Clin Oncol 2010;28(5):780-7. 2.Chiorean et al. Presented at EORTC-NCI-AACR Symposium on Molecular Targets and Cancer Therapeutics 2007. Abstract B15. 3.Data on file, Eli Lilly and Company.
: Chiorean et al. Presented at EORTC-NCI-AACR Symposium on Molecular Targets and Cancer Therapeutics Abstract B15. 3.Data on file, Eli Lilly and Company..")
42
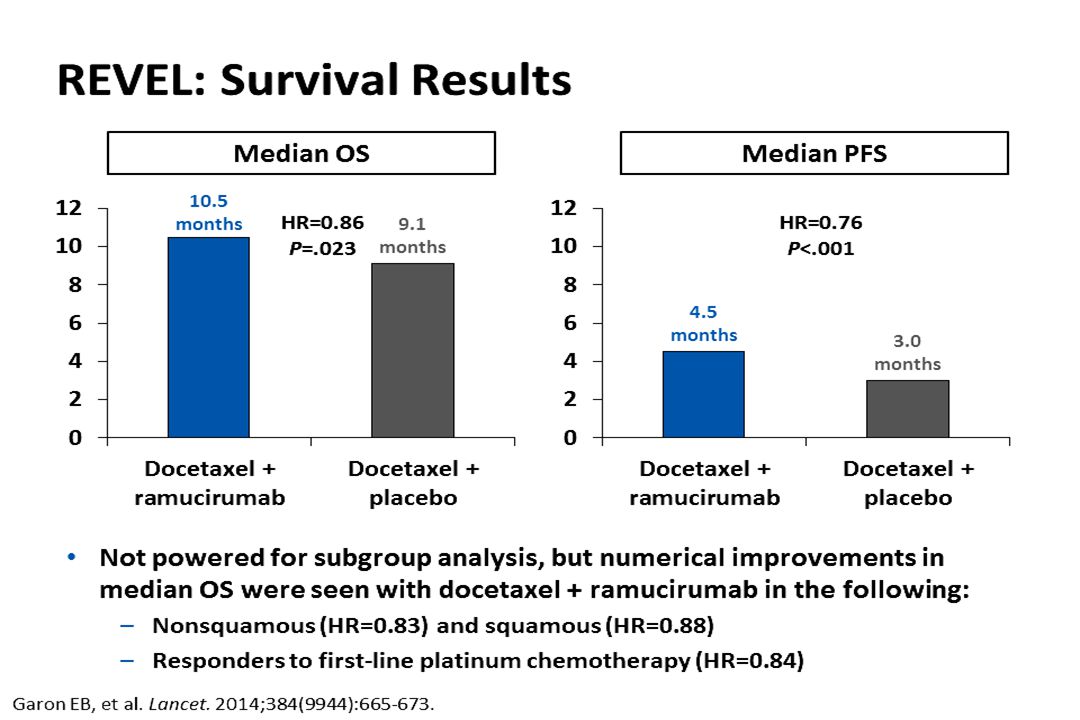
REVEL: Phase III trial Ramucirumab (10 mg/kg) + docetaxel (75 mg/m 2 ) n=628 Ramucirumab (10 mg/kg) + docetaxel (75 mg/m 2 ) n=628 Placebo + docetaxel (75 mg/m 2 ) n=625 Placebo + docetaxel (75 mg/m 2 ) n=625 R A N D O M IS E Stage IV NSCLC Failed 1st-line platinum-based chemotherapy +/ maintenance Any histology ECOG PS 0 or 1 No prior EGFR TKI monotherapy or docetaxel 1:1 PD Primary endpoint: overall survival Secondary endpoints: PFS (investigator review), objective response rate, safety, patient-reported outcomes Primary endpoint: overall survival Secondary endpoints: PFS (investigator review), objective response rate, safety, patient-reported outcomes Garon et al. Lancet 2014;384:335–673.

43
REVEL: Overall Survival – ITT Population Garon et al. Lancet 2014;384(9944):665-73.
:")
44
REVEL: Overall Survival by Histology Garon et al. Lancet 2014;384(9944):665-73.
:")
47
REVEL: Conclusions Ramucirumab improvement in OS, PFS and overall response rate 1 Overall survival benefit in squamous and nonsquamous NSCLC The safety profile minimal. Which is the minimum clinically valuable difference? 1.Garon et al. Lancet 2014;384(9944):665-73. 2.Garon et al. Presented at EMSO 2014. Abstract 5775. REVEL trialLUME-Lung 1 trial Trial designPhase III, N=1,253Phase III, N=1,314 TreatmentRamucirumab + docetaxel / Placebo + docetaxelNintedanib + docetaxel / Placebo + docetaxel Stratification ECOG PS (0 vs 1) Sex Previous maintenance therapy Geographic region (Taiwan/South Korea vs other) ECOG PS (0 vs 1) Prior bevacizumab Brain metastases Histology (squamous vs nonsquamous) Primary endpointOSPFS (central independent review) Previous treatment1 platinum-based chemotherapy (14% prior bevacizumab) 1 chemo chemotherapy (> 95% had platinum- based chemotherapy; 4% prior bevacizumab) CountriesGlobal (not Japan)
: Garon et al. Presented at EMSO Abstract REVEL trialLUME-Lung 1 trial Trial designPhase III, N=1,253Phase III, N=1,314 TreatmentRamucirumab + docetaxel / Placebo + docetaxelNintedanib + docetaxel / Placebo + docetaxel Stratification ECOG PS (0 vs 1) Sex Previous maintenance therapy Geographic region (Taiwan/South Korea vs other) ECOG PS (0 vs 1) Prior bevacizumab Brain metastases Histology (squamous vs nonsquamous) Primary endpointOSPFS (central independent review) Previous treatment1 platinum-based chemotherapy (14% prior bevacizumab) 1 chemo chemotherapy (> 95% had platinum- based chemotherapy; 4% prior bevacizumab) CountriesGlobal (not Japan).")
48
REVEL vs LUME-Lung 1 in 2L treatment of NSCLC REVEL trialLUME-Lung 1 trial Ramucirumab + docetaxel (n=628) Placebo + docetaxel (n=625) Nintedanib + docetaxel (n=655) Placebo + docetaxel (n=659) OS, months 10.59.110.19.1 HR (95% CI) 0.86 (0.75−0.98); p=0.0230.94 (0.83–1.05); p=0.272 Investigator assessment ORR, % 22.9*13.610.47.6 PFS, months 4.53.0 4.23.1 HR (95% CI) 0.76 (0.68–0.86); p<0.0010.80 (0.69–0.93); p=0.003 *p<0.001 vs placebo REVEL trial (non-squamous)LUME-Lung 1 trial (adenocarcinoma) Ramucirumab + docetaxel (n=628) Placebo + docetaxel (n=625) Nintedanib + docetaxel (n=655) Placebo + docetaxel (n=659) OS, months 11.19.712.610.3 HR (95% CI) 0.90 (0.71–0.97); p=0.0200.83 (0.70–0.99); p=0.036 Investigator assessment ORR, % 21.9*14.511.58.9 PFS, months 4.63.7 HR (95% CI) 0.77 (0.67-0.88); p<0.0010.78 (0.62–0.97); p=0.025
 Placebo + docetaxel (n=625) Nintedanib + docetaxel (n=655) Placebo + docetaxel (n=659) OS, months HR (95% CI) 0.86 (0.75−0.98); p= (0.83–1.05); p=0.272 Investigator assessment ORR, % 22.9* PFS, months HR (95% CI) 0.76 (0.68–0.86); p< (0.69–0.93); p=0.003 *p<0.001 vs placebo REVEL trial (non-squamous)LUME-Lung 1 trial (adenocarcinoma) Ramucirumab + docetaxel (n=628) Placebo + docetaxel (n=625) Nintedanib + docetaxel (n=655) Placebo + docetaxel (n=659) OS, months HR (95% CI) 0.90 (0.71–0.97); p= (0.70–0.99); p=0.036 Investigator assessment ORR, % 21.9* PFS, months HR (95% CI) 0.77 ( ); p< (0.62–0.97); p=0.025")
49
A majority of NSCLC patients do not have targetable mutations Second-line treatment options for these patients have historically been limited Important new options for patients without driver mutations who have few effective treatment choices Nintedanib is the only TKI to show a potential OS benefit in the second-line setting Ramucirumab is the first monoclonal antibody to show a survival benefit in the second-line setting (in combination with docetaxel) and the first to benefit patients with disease characterized by squamous histology Careful manegement of side effects will be critical to ensuring that patients maximice treatment benefit Key take-aways
 and the first to benefit patients with disease characterized by squamous histology Careful manegement of side effects will be critical to ensuring that patients maximice treatment benefit Key take-aways")
50
REVEL: Baseline Patient Demographics and Characteristics (2 of 2) Garon et al. Lancet 2014;384(9944):665-73. Characteristic RAM+DOC (N = 628) PL+DOC (N = 625) n(%)n Disease Measurable606(96)603(96) Nonmeasurable22(4)22(4) Smoking history Ever518(82)483(77) Never109(17)141(23) Unknown1(<1)1 EGFR status Wild type207(33)197(32) Mutant15(2)18(3) Unknown or missing406(65)410(66) Best response to platinum CR/PR/SD420(67)417(67) PD178(28)182(29) Previous maintenance No 493(79)482(77) Yes 135(21)143(23) Prior taxaneYes 153(24)149(24) Prior bevacizumabYes 88(14)92(15) Time since previous therapy <9 months400(64)374(60) ≥9 months226(36)251(40) Missing2(<1)0-
: Characteristic RAM+DOC (N = 628) PL+DOC (N = 625) n(%)n Disease Measurable606(96)603(96) Nonmeasurable22(4)22(4) Smoking history Ever518(82)483(77) Never109(17)141(23) Unknown1(<1)1 EGFR status Wild type207(33)197(32) Mutant15(2)18(3) Unknown or missing406(65)410(66) Best response to platinum CR/PR/SD420(67)417(67) PD178(28)182(29) Previous maintenance No 493(79)482(77) Yes 135(21)143(23) Prior taxaneYes 153(24)149(24) Prior bevacizumabYes 88(14)92(15) Time since previous therapy <9 months400(64)374(60) ≥9 months226(36)251(40) Missing2(<1)0-.")
Similar presentations