Download presentation
Presentation is loading. Please wait.

1
Angioedema of the GI Tract Howard Weiner, MD June 21, 2006

2
C.K. 41 YO WHITE FEMALE 11.01.05 – Admitted via Internist’s Office HPI: 1 day history of abdominal pain, fever, nausea, vomiting; several days of minimal diarrhea PMH: Heartburn, hypercholesterolemia, asthma, hypertension, breast biopsy SH: ENT Office Worker; FMH: None MEDS: Lipitor, Protonix, Advair, Singulair, Dyazyde, Tri-norinyl; NKA PE: 152/100P116T100.2 ASD: obese, soft, bowel sounds normal, mild epigastric tenderness LAB: WBC 21,200; HGB 14; LFTS, Amylase, Lipase WNL CT SCAN: Markedly thickened duodenum and proximal jejunum, some free fluid in the pelvis, fatty liver.

3
C.K. 11.03.05 Endoscopy:acute duodenitis, with edema and erosions, extending into jejunum, erosive gastritis Biopsy:Bulb: mild increase in chronic inflammatory cells 11.04.05 Discharged

4
C.K. 01.29.06 – Admitted via ER HPI: 1 week of increased bowel frequency, followed by cramps, nausea, vomiting 1 day PTA MEDS: Lisinopril, Singulair, Lipitor, Prevacid, Trinorinyl PE: 137/96P100T98.6R18 ABD: obese, mild mid and lower abdominal tenderness. LAB: WBC 20,100; HgB 14.4; AST 43, GLU 131, stool Heme stool WBC Ө CT: Markedly thickened 3 rd, 4 th duodenum and proximal jejunum, free fluid, fatty liver

5
C.K. 01.30.06 Enteroscopy to 190 cm: copious secretions, slightly edematous with focal submucosal erythema in small bowel Biopsy:increased intramucosal chronic inflammatory cells Post procedure:sore throat; 1½ hour post procedure uvula, face, tongue, lips are swollen Subsequent history of regarding lisindpril C1 Esterase inhibitor 28 (21 – 29 mg/dL)
.")
6
Angioedema (AE) Non-inflammatory disease Increased capillary permeability in various organs/areas 1 st described in 1882 1 st report of hereditary AE in 1888 (Osler) Classification Hereditary Non-Hereditary
 Non-inflammatory disease Increased capillary permeability in various organs/areas 1 st described in st report of hereditary AE in 1888 (Osler) Classification Hereditary Non-Hereditary")
7
Classification of Recurrent Angioedema 1. Hereditary angioedema due to defiC1ency of C1 inhibitor protein and activity (hereditary angioedema type I) 2. Hereditary angioedema due to defiC1ency of C1 inhibitor activity (hereditary angioedema type II) 3. Hereditary angioedema with normal C1 inhibitor activity in women (hereditary angioedema type III) 4. Acquired angioedema due to increased consumption of C1 inhibitor or autoantibody formation (acquired angioedema types I and II) 5. Recurrent angioedema due to angiotensin-converting enzyme inhibitors or angiotensin II-receptor antagonists 6. Urticaria-related angioedema 7. Idiopathic angioedema
 2. Hereditary angioedema due to defiC1ency of C1 inhibitor activity (hereditary angioedema type II) 3. Hereditary angioedema with normal C1 inhibitor activity in women (hereditary angioedema type III) 4. Acquired angioedema due to increased consumption of C1 inhibitor or autoantibody formation (acquired angioedema types I and II) 5. Recurrent angioedema due to angiotensin-converting enzyme inhibitors or angiotensin II-receptor antagonists 6. Urticaria-related angioedema 7. Idiopathic angioedema.")
8
Angioedema Clinical characteristics Episodes last 1-3 days Face, airway, GI tract, skin, brain, muscle, urogenital tract Provocative Factors Infection, diagnostic tests, drugs, hormones

9
Hereditary AE Defect of C1 esterase inhibitor Dominant trait, variable penetrance 20-25% do not have FMH Incidence 1:50,000 to 1:150,000 Onset early adolescence Variable Presentation Skin91% Abdominal73% Laryngeal48%

10
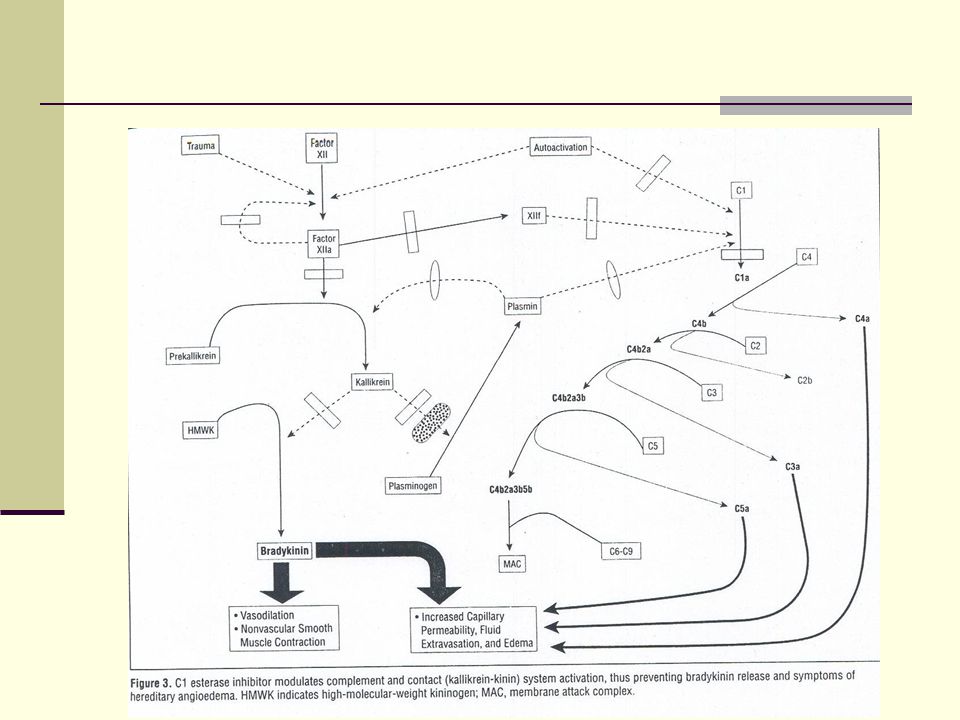
Hereditary AE Mechanism C1 INH prevents conversion of inactive C1 to active form C1 INH blocks plasma proteases, kallikrein, factor XII If C1 INH is not present or functional, vasoactive mediators are released

11
Lab Studies C4, C2, C1 inhibitor levels C1 inhibitor activity C3 SPEP Treatment Antihistamine Epinephrine Steroids Androgen (Danazol) C1 INH concentrate Plasminogen inhibitor
 C1 INH concentrate Plasminogen inhibitor")
12
Acquired AE (C1 INH deficiency) Paraneoplastic syndrome Lymphomas Multiple myeloma Waldenstrom’s CLL Other neoplasms Autoimmune disease Caused by various mechanisms involving paraproteins and immune complexes leading to activation of the C1 complex and depletion of C1 inhibitor
 Paraneoplastic syndrome Lymphomas Multiple myeloma Waldenstrom’s CLL Other neoplasms Autoimmune disease Caused by various mechanisms involving paraproteins and immune complexes leading to activation of the C1 complex and depletion of C1 inhibitor")
13
Angioedema Due to ACE Inhibitors 1 st reported with enalapril - 06.1988 Incidence 0.1-0.2% Octave trial 0.68% Usually apparent within 7 days of initiating Rx; risk levels off by 9 weeks Less severe than hereditary AE Isolated tongue swelling more common Hereditary and idiopathic AE may predispose as may prior drug reactions/seasonal allergies Black Female Small percentage get it with ARB’s also Proposed Mechanisms ACE (Kininase II) degrades bradykinin; when this doesn’t occur vasoactive compounds produce vasodilatation Genetic defects in Kininase I may predispose Induction of tissue or drug specific antibodies Induction of C1 inhibitor deficiency
 degrades bradykinin; when this doesn’t occur vasoactive compounds produce vasodilatation Genetic defects in Kininase I may predispose Induction of tissue or drug specific antibodies Induction of C1 inhibitor deficiency")
14
ACE Inhibitors BenazeprilLotensin CaptoprilCalan EnalaprilVasotec Lexxel FosinoprilMonopril LisinoprilPrinivil Zestril MoexiprilUnirotic RamiprilAltace TrandolaprilMavik Tarka

15
Visceral Angioedema Due to ACE Inhibitors Case Reports ’88, ’93, ’94, ’97, ’00 1 st case report of lisinoril causing isolated visceral AE in 04.97 Female predominance Areas of involvement Jejunum Ileum Duodenum Stomach Colon Pancreas/Biliary tree Ascites Symptoms Abdominal pain Nausea, vomiting Diarrhea Ascites No fever

16
Visceral Angioedema Due to ACE Inhibitors Differential Diagnosis Inflammatory bowel disease Hemorrhage Ischemic bowel Neoplasm Vasculitis Bowel obstruction Pseudo obstruction Findings Leukocytosis Ascites Imaging of bowel wall edema All stool studies negative Lab Evaluations C1 inhibitor level normal No other complement components depleted

17
Treatment of ACE Inhibitor AE Stop ACE Inhibitor Probably don’t use ARB Antihistamines Epinephrine Coricosteroids Miscellaneous Multiple presentations IBD therapy surgery/cholecystectomy

18
Angioedema and Gastroenterology Report associating AE with midazolam Report associating AE with Bezocaine Study showing increased incidence of AE with H. pylori

Similar presentations









 For the prevention and treatment of acute attacks of Hereditary Angioedema Reid Nakagawa November 31, 2013.>")

 Admission criteria for.>")


>")






