Download presentation
Presentation is loading. Please wait.

1
Introduction to Nephrology Sandeep K. Shori, D.O. Dialysis Associates Fort Worth, TX

2
The ultimate goal of a nephrologist is to maintain renal function and manage associated metabolic changes and prolong time till dialysis. Only a nephrologist can perform hemodialysis Nephrologists manage Acute Renal Failure and provide lifesaving Continuous Renal Replacement Threapy (CRRT) in the ICU. Nephrologists are specialists in electrolyte, fluid balance, acid/base, anemia assoc renal disease, metabolic bone disease, and Hypertension management.
 in the ICU. Nephrologists are specialists in electrolyte, fluid balance, acid/base, anemia assoc renal disease, metabolic bone disease, and Hypertension management..")
3
When should you call for a nephrologist? When does a patient need a Nephrologist? What therapy can be given? What is the most common cause of kidney disease? Why is kidney disease increasing so rapidly? How many Americans are on dialysis now? What is a interventional nephrologist?

4
What you need to know about kidney disease including Diagnosis, intervention, and prognosis? What is GFR and what is its importance in renal management and dialysis? KDOQI expands the Dialysis Outcomes Quality Initiative or DOQI, a project begun by the National Kidney Foundation in 1997 and recognized throughout the world for improving the care of dialysis patients

5
A sustained decrease in blood flow or prolonged obstruction is often associated with kidney damage. Chronically decreased GFR is more often associated with kidney damage. > 3 months for the definition of chronic kidney disease. Decreased GFR may be acute or chronic. An acute decrease in GFR does not necessarily indicate the presence of kidney damage.

6
Decreased GFR is one of the markers of kidney damage. This marker is used to evaluate for kidney disease and its associated etiology. Individuals without evidence of kidney damage, yet chronically decreased GFR, are at increased risk for adverse outcomes (for example, toxicity from drugs excreted by the kidney, and acute kidney failure in a wide variety of circumstances).
..")
9
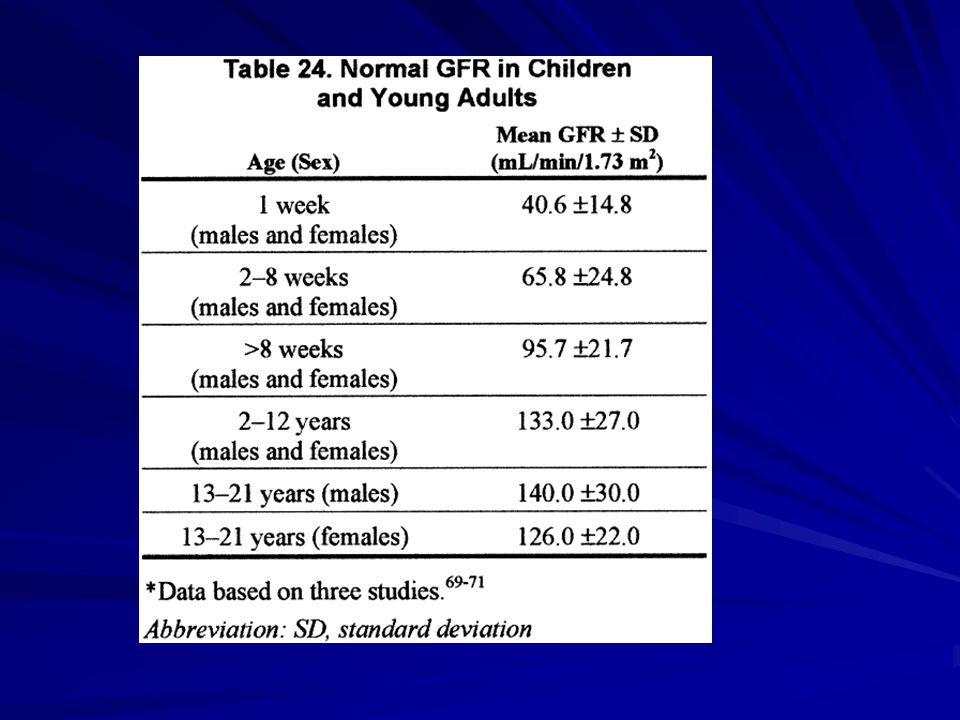
Chronically low GFR is age dependent. GFR <90 mL/min/1.73 m2 would be abnormal in a young adult. On the other hand, a GFR of 60–89 mL/min/1.73 m2 could be normal from approximately 8 weeks to 1 year of age and in older individuals. GFR 30 to 59 mL/min/1.73 m2 could also be normal in individuals at the extremes of age, in vegetarians, after unilateral nephrectomy or in an older individual. It is likely that a GFR <30 mL/min/1.73 m2 is abnormal at all ages other than neonates

10
Clinicians initiate replacement therapy based on -Level of kidney function, presence of signs and symptoms of uremia, the availability of therapy. Variabile relationship exists between level of kidney function to signs/symptoms of uremia. Variabile relationship exists between level of kidney function to signs/symptoms of uremia. The level of GFR at the beginning of dialysis has been estimated in more than 90,000 patients in the United States between 1995 and 1997, using data collected on the Medical Evidence Report (HCFA Form 2728) and the MDRD Study prediction equation
 and the MDRD Study prediction equation.")
12
EVALUATION AND TREATMENT The evaluation and treatment of patients with kidney disease requires understanding of separate but related concepts of diagnosis, comorbid conditions, severity of disease, complications of disease, and risks for loss of kidney function and cardiovascular disease. Patients with kidney disease should be evaluated to determine: –Diagnosis (type of kidney disease); –Comorbid conditions; –Severity, assessed by level of kidney function; –Complications, related to level of kidney function; –Risk for loss of kidney function; –Risk for cardiovascular disease.
; –Comorbid conditions; –Severity, assessed by level of kidney function; –Complications, related to level of kidney function; –Risk for loss of kidney function; –Risk for cardiovascular disease..")
13
Treatment of kidney disease should include: –Specific therapy, based on diagnosis; –Evaluation and management of comorbid conditions; –Slowing the loss of kidney function; –Prevention + treatment cardiovascular disease; –Prevention and treatment of complications of decreased kidney function; –Preparation for kidney failure and kidney replacement therapy; –Replacement of kidney function by dialysis and transplantation, if signs and symptoms of uremia are present.

14
Review of medications should be performed at all visits for the following: –Dosage adjustment based on level of kidney function –Detection of potentially adverse effects on kidney function or complications of chronic kidney disease –Detection of drug interactions –Therapeutic drug monitoring, if possible. Self-management behaviors should be incorporated into the treatment plan at all stages of kidney disease. Refer to a nephrologist for consultation and co-management when GFR <30 mL/min/1.73 m2

15
The definitive diagnosis type of kidney disease is based on biopsy or imaging studies. Often avoided unless a definitive diagnosis would change either the treatment or prognosis. Diabetic kidney disease is the largest single cause of kidney failure. Both type 1 and type 2 diabetes cause chronic kidney disease. Because of the higher prevalence of type 2 diabetes, it is the more common cause of diabetic kidney disease. Diabetic kidney disease usually follows a characteristic clinical course after the onset of diabetes, first manifested by microalbuminuria, then clinical proteinuria, hypertension, and declining GFR.

16
Diseases which cause chronic kidney disease. Evaluation and management of these diseases is important for patients’ well being and may improve the course of chronic kidney disease. This is particularly important for patients with diabetes and high blood pressure, the leading causes of chronic kidney disease and cardiovascular disease in the United States. Cardiovascular disease. Cardiovascular disease is singled out from among the possible comorbid conditions to emphasize its complex relationship with chronic kidney disease, and its importance as a preventable cause of morbidity and mortality in patients with chronic kidney disease. Cardiovascular disease. Cardiovascular disease is singled out from among the possible comorbid conditions to emphasize its complex relationship with chronic kidney disease, and its importance as a preventable cause of morbidity and mortality in patients with chronic kidney disease. In all cases, management of comorbid conditions must be integrated into the overall care of patients with chronic kidney disease.

Similar presentations










>")


>")








