Download presentation
Presentation is loading. Please wait.

1
1 Gardasil TM : Quadrivalent Human Papillomavirus 6, 11, 16, 18 L1 VLP Vaccine Applicant: Merck & Co., Inc. Gardasil TM : Quadrivalent Human Papillomavirus 6, 11, 16, 18 L1 VLP Vaccine Applicant: Merck & Co., Inc. Vaccines and Related Biological Products Advisory Committee Meeting May 18, 2006 Nancy B. Miller, M.D. CBER, FDA

2
2 Review Team Chairperson:Gopa Raychaudhuri, Ph.D. Regulatory Coordinator:Julienne Vaillancourt, R.Ph., M.P.H. Clinical:Nancy Miller, M.D. Joseph Toerner, M.D., M.P.H. Joseph Toerner, M.D., M.P.H. Karen Goldenthal, M.D. Karen Goldenthal, M.D. Antonia Geber, M.D. Antonia Geber, M.D. Douglas Pratt, M.D., M.P.H Douglas Pratt, M.D., M.P.H Statistical:Henry Hsu, Ph.D., M.P.H. Lev Sirota, Ph.D. Lev Sirota, Ph.D. A. Dale Horne, Dr.Ph. A. Dale Horne, Dr.Ph. Product:Robin Levis, Ph.D. Rolf Taffs, Ph.D. Rolf Taffs, Ph.D. Gennady Rezapkin, Ph.D. Gennady Rezapkin, Ph.D. Loris McVittie, Ph.D. Loris McVittie, Ph.D. Jerry Weir, Ph.D. Jerry Weir, Ph.D. Non-Clinical:Sally Hargus, Ph.D. Marion Gruber, Ph.D. Marion Gruber, Ph.D. Pharmacovigilance: Hector Izurieta, M.D. Robert Ball, M.D., M.P.H. Bioresearch Monitoring:Robert Wesley Facility: Susan Yu, Ph.D. Laurie Norwood, Ph.D. Laurie Norwood, Ph.D. Advertising/Promotional Labeling: Maryann Gallagher

3
3 Gardasil: Description Each 0.5 mL dose contains –20 mcg HPV 6 L1 VLP –40 mcg HPV 11 L1 VLP –40 mcg HPV 16 L1 VLP –20 mcg HPV 18 L1 VLP –Adjuvant: 225 mcg aluminum Administered 0, 2, and 6 months IM

4
4 Gardasil: Applicant’s Proposed Indications (1) Prevention of HPV 16/18 related: –Cervical cancer –Cervical AIS –CIN 2 and CIN 3 –Vulvar and vaginal cancer –VIN 2 and VIN 3 –VaIN 2 and VaIN 3 Prevention of HPV 6/11/16/18 related: –CIN grade 1 –Genital warts (condyloma acuminata) –VIN grade 1 and VaIN grade 1 –HPV infection AIS = Adenocarcinoma in situ; CIN = Cervical Intraepithelial Neoplasia; VIN = Vulvar Intraepthelial Neoplasia; VaIN = Vaginal Intraepithelial Neoplasia
 Prevention of HPV 16/18 related: –Cervical cancer –Cervical AIS –CIN 2 and CIN 3 –Vulvar and vaginal cancer –VIN 2 and VIN 3 –VaIN 2 and VaIN 3 Prevention of HPV 6/11/16/18 related: –CIN grade 1 –Genital warts (condyloma acuminata) –VIN grade 1 and VaIN grade 1 –HPV infection AIS = Adenocarcinoma in situ; CIN = Cervical Intraepithelial Neoplasia; VIN = Vulvar Intraepthelial Neoplasia; VaIN = Vaginal Intraepithelial Neoplasia")
5
5 Gardasil: Applicant’s Proposed Indications (2) Children and adolescents 9 through 17 years of age and women 18 through 26 years of age.
 Children and adolescents 9 through 17 years of age and women 18 through 26 years of age.")
6
6 Gardasil: FDA Proposed Indications FDA considers the data submitted in the BLA to be supportive of use of Gardasil in preadolescent and adolescent and females 18-26 years of age. FDA considers the data submitted in the BLA to be supportive of use of Gardasil in preadolescent and adolescent females 9-17 years of age and females 18-26 years of age.

7
7 Regulatory History 1997: Submission of IND for monovalent HPV 11 L1 VLP vaccine (Other INDs for monovalent HPV 16 and 18) 2000: Submission of IND for quadrivalent HPV 6, 11, 16, 18 L1 VLP vaccine 2001 (November): VRBPAC discussion of endpoints for Phase 3 development 2002: Product development program granted fast track status; Initiation of Phase 3 trials 2005 (May): Pre-BLA meeting, agreement to allow rolling BLA and Priority Review 2005 (August): Start of rolling BLA submisssion 2005 (December): Last section of rolling BLA received including Phase 3 study data; 6 month priority review
 2000: Submission of IND for quadrivalent HPV 6, 11, 16, 18 L1 VLP vaccine 2001 (November): VRBPAC discussion of endpoints for Phase 3 development 2002: Product development program granted fast track status; Initiation of Phase 3 trials 2005 (May): Pre-BLA meeting, agreement to allow rolling BLA and Priority Review 2005 (August): Start of rolling BLA submisssion 2005 (December): Last section of rolling BLA received including Phase 3 study data; 6 month priority review")
8
8 Efficacy Endpoint for Preventive HPV Vaccines (Cervical Cancer) November 2001 VRBPAC: CIN 2/3 histology, AIS, or worse with virology. CIN 2/3 histology, AIS, or worse with virology.

9
9 Phase I/II Safety and Immunogenicity Studies 001: HPV 11 L1 VLP Vaccine 002: HPV 16 L1 VLP Vaccine 004: HPV 16 L1 VLP Vaccine 006: HPV 18 L1 VLP Vaccine

10
10 Gardasil BLA: Protocols Contributing to Combined Efficacy Analysis “Proof of Concept” Phase II Efficacy Trial (HPV 16) 005: “Proof of Concept” Phase II Efficacy Trial (HPV 16) Quadrivalent Dose-Ranging and Efficacy Study 007: Quadrivalent Dose-Ranging and Efficacy Study CIN/Warts Efficacy Study 013: CIN/Warts Efficacy Study CIN 2/3 Efficacy Study 015: CIN 2/3 Efficacy Study
 005: Proof of Concept Phase II Efficacy Trial (HPV 16) Quadrivalent Dose-Ranging and Efficacy Study 007: Quadrivalent Dose-Ranging and Efficacy Study CIN/Warts Efficacy Study 013: CIN/Warts Efficacy Study CIN 2/3 Efficacy Study 015: CIN 2/3 Efficacy Study")
11
11 Gardasil Protocol 013 Substudies Gardasil: Protocol 013 Substudies Hepatitis B Concomitant Use Substudy 011: Hepatitis B Concomitant Use Substudy HPV 16 Bridging Substudy 012: HPV 16 Bridging Substudy

12
12 Immunogenicity and Safety Studies in Adolescents Adolescent/Adult Bridging and End-Expiry Study 016: Adolescent/Adult Bridging and End-Expiry Study Adolescent Immunogenicity and Safety Study 018: Adolescent Immunogenicity and Safety Study

13
13 Comparison of Study Design: Protocols That Contribute to Combined Analysis Features Protocol 005 Protocol 007 Protocol 013 Protocol 015 SitesUS US, International Design DB, R, PC Vaccine HPV 16 GardasilGardasil*Gardasil *384 subjects received HPV 16 to bridge to Protocol 005 DB = Double blind; R=Randomized; PC = Placebo controlled From Table 1, HPV L1 VLP Vaccine Combined Efficacy (Interim Analysis)
")
14
14 Comparison of Study Design: Baseline Characteristics of Subjects Subjects Protocol 005 Protocol 007 Protocol 013 Protocol 015 Inclusion Criteria AgeGender 16-23 years female female female 16-26 years* female Lifetime Partners 0-50-40-40-4 Exclusion Criteria Previous abnormal Pap Not allowed *23 years except for 26 years in Singapore Source: Table 1, HPV L1 VLP Vaccine Combined Efficacy (Interim Analysis Report)
")
15
15 Comparison of Study Design: Pap Tests and Referral for Colposcopy Features Protocol 005 Protocol 007 Protocol 013 Protocol 015 Pap interval 6 months 12 months Pap test ThinPrep TM Pap reading 5 regional labs DCL Lab, Indianapolis DCL Lab, Indianapolis DCL Lab, Indianapolis Minimal Pap Referral ASC-USASC-US HPV (+) HC-II ASC-US ASC-US Screening Triage VoluntaryVoluntaryMandatoryMandatory Exit Colposcopy YesYesNoNo Source: Interim Analysis, Table 1
 HC-II ASC-US ASC-US Screening Triage VoluntaryVoluntaryMandatoryMandatory Exit Colposcopy YesYesNoNo Source: Interim Analysis, Table 1")
16
16 Comparison of Study Design: Triage Abnormal Pap Tests for Colposcopy ThinPrep TM Pap Result Protocol 005 Protocols 007 and 013 Protocol 015 ASC-US Reflex HPV test on residual ThinPrep TM material; if probe positive, referred for colposcopy; if probe negative, Pap at routine interval Reflex HPV test on residual ThinPrep TM material; if at least one probe positive, referred for colposcopy; if both probes negative, Pap at routine interval Repeat ThinPrep TM Pap in 6 months LSIL Referred for colposcopy Repeat ThinPrep TM Pap in 6 months Source: Table 2.7.3-cervix cancer: 5

17
17 Comparison of Study Design: Laboratory Tests, Pathology Panel Features Protocol 005 Protocol 007 Protocol 013 Protocol 015 Laboratory Processing DCL Lab, Indianapolis Pathology Panel Reading (Endpoints)* KurmanRonetteStolerFerenczy^KurmanRonetteStolerFerenczyKurmanRonetteStolerFerenczyKurmanRonetteStolerFerenczy HPV Causality Assessment Merck HPV PCR assay frozen biopsy Merck HPV PCR assay paraffin *All biopsies in 4 studies read by one of several pathologists in central Lab for patient management. Biopsies also independently read by panel of expert pathologists for final diagnosis for study purposes (endpoints). Panel blinded to group, HPV testing, dx at DCL. ^Until 10/2000, pathologists were Kurman/Sherman/Stoler/Ferenczy Source: Interim Analysis, Table 1
. Panel blinded to group, HPV testing, dx at DCL. ^Until 10/2000, pathologists were Kurman/Sherman/Stoler/Ferenczy Source: Interim Analysis, Table 1.")
18
18 Comparison of Study Design: Number of Subjects, Median Age, and Duration of Follow-up In Efficacy Population Subjects Protocol 005 Protocol 007 Protocol 013 Protocol015 N # Vaccine # Placebo 2391119311985512762755442271727251215760826075 Median Age (Range) 20 yr. (16-25) (13-24) (16-24) (15-26) Mean duration of follow-up 3.1 years 2.4 years 1.7 years 1.4 years Total number of subjects with data for cervical disease efficacy = 20541 Sources: CSR 007, Table 7-2 and 2.7.3–cervix cancer Table 2.7.3:8
 (13-24) (16-24) (15-26) Mean duration of follow-up 3.1 years 2.4 years 1.7 years 1.4 years Total number of subjects with data for cervical disease efficacy = Sources: CSR 007, Table 7-2 and 2.7.3–cervix cancer Table 2.7.3:8.")
19
19 Number of Subjects Enrolled: Distribution by Protocol and Region (Efficacy Population) Subjects Protocol 005 Protocol 007 Protocol 013 Protocol 015 Total North America 2391(100%)251(45.6%)1713(29.8%)913(7.5%)5268 Latin America 0187(33.9%)2278(39.8%)3191(26.2%)5606 Europe0113(20.5%)1189(20.7%)7872(64.8%)9174 Asia-Pacific00566(9.9%)181(1.5%)747 Source: Table 2.7.3-cervix cancer: 9
 Subjects Protocol 005 Protocol 007 Protocol 013 Protocol 015 Total North America 2391(100%)251(45.6%)1713(29.8%)913(7.5%)5268 Latin America 0187(33.9%)2278(39.8%)3191(26.2%)5606 Europe0113(20.5%)1189(20.7%)7872(64.8%)9174 Asia-Pacific00566(9.9%)181(1.5%)747 Source: Table cervix cancer: 9")
20
20 Subjects Excluded from Efficacy Analysis Because of Baseline HPV Status GardasilPlaceboTotal Number of Subjects Enrolled 102911029220583 Received > 1 injection 102681027320541 Excluded from PPE analysis HPV 16 HPV 18 281816263008169258263318 Sero and/or PCR+ HPV 16 * At Day 1 At/before Month 7 165417701679202933333799 Sero and/or PCR+ HPV 18 * At Day 1 At/before Month 7 57465657277311461428 *Day 1 includes Sero+ and/or PCR+. Post Day 1 includes PCR+ only. Source: Interim Analysis Report, Table 2

21
21 Role of Baseline HPV Status and Endpoint Counting for Prophylactic Vaccine Efficacy Analyses Baseline HPV Status HPV 6- related HPV 11- related HPV 16- related HPV 18- related Naïve to all 4 vaccine HPV types YesYesYesYes Positive HPV 6 or 11, Naïve 16/18 NoNoYesYes Positive HPV 16, Naïve for 6/11/18 YesYesNoYes Positive HPV 18, Naïve 6/11/16 YesYesYesNo Naïve: Subjects seronegative Day 1 and PCR negative Day 1 through Month 7. Source: Merck Briefing Document

22
22 Role of Baseline HPV Status and Endpoint Counting for Prophylactic Vaccine Efficacy Analyses Baseline HPV Status HPV 6- related HPV 11- related HPV 16- related HPV 18- related Naïve to all 4 vaccine HPV types YesYesYesYes Positive HPV 6 or 11, Naïve 16/18 NoNoYesYes Positive HPV 16, Naïve for 6/11/18 YesYesNoYes Positive HPV 18, Naïve 6/11/16 YesYesYesNo Source: Merck Briefing Document Note: Non-HPV 6, 11, 16, 18 related disease not included in analyses.

23
23 Efficacy Analysis Populations (1) Per Protocol Population for Efficacy (PPE): Received all 3 vaccinations, naïve to relevant vaccine HPV type through Month 7, did not deviate from protocol; cases counted after Month 7. Modified Intent to Treat -1 Population (MITT-1): Same as PPE, but included protocol violators Modified Intent to Treat-2 Population (MITT-2): Received at least 1 vaccination, naïve to relevant vaccine HPV type at Day 1, and had any follow-up visit after the first vaccination; cases counted from 30 days after dose 1.
: Same as PPE, but included protocol violators Modified Intent to Treat-2 Population (MITT-2): Received at least 1 vaccination, naïve to relevant vaccine HPV type at Day 1, and had any follow-up visit after the first vaccination; cases counted from 30 days after dose 1..")
24
24 Efficacy Analysis Populations (2) Restricted MITT-2 Population (RMITT-2): Seronegative and PCR negative to all four vaccine HPV types at Day 1 and a normal Pap test at Day 1; cases counted 30 days after dose 1. All MITT-1 Population: Naïve to all four vaccine HPV types through Month 7, and cases counted starting after Month 7.

25
25 Efficacy Analysis Populations (3) Modified Intent to Treat-3 Population (MITT-3): Received at least one vaccination and had any follow-up visit one month after dose 1. Cases were counted from 30 days after dose 1. Subjects were included regardless of baseline HPV status.

26
26 Baseline Characteristics of Subjects in Efficacy Population (Protocols 005, 007, 013, and 015) Squamous intraepithelial lesion (SIL) present at baseline: 12% PCR positive and/or seropositive to a vaccine HPV type: 27%
 Squamous intraepithelial lesion (SIL) present at baseline: 12% PCR positive and/or seropositive to a vaccine HPV type: 27%")
27
27 Endpoints from Efficacy Protocols (Protocols 005, 007, 013, and 015) Primary Endpoints: HPV 16/18 related CIN 2/3 or worse [015, combined analysis] HPV 6/11/16/18 related CIN [013] HPV 6/11/16/18 related External Genital Lesions (EGLs) [013]
![27 Endpoints from Efficacy Protocols (Protocols 005, 007, 013, and 015) Primary Endpoints: HPV 16/18 related CIN 2/3 or worse [015, combined analysis] HPV 6/11/16/18 related CIN [013] HPV 6/11/16/18 related External Genital Lesions (EGLs) [013]](http://images.slideplayer.com/12/3347513/slides/slide_27.jpg "27 Endpoints from Efficacy Protocols (Protocols 005, 007, 013, and 015) Primary Endpoints: HPV 16/18 related CIN 2/3 or worse [015, combined analysis] HPV 6/11/16/18 related CIN [013] HPV 6/11/16/18 related External Genital Lesions (EGLs) [013]")
28
28 Other Endpoints Other Endpoints of Interest: HPV 16/18 related EGLs CIN 2/3 due to any HPV type and non-vaccine HPV types EGL due to any HPV type and non- vaccine HPV types

29
29 Efficacy Against HPV 16/18 CIN 2/3 or Worse

30
30 Analysis of Efficacy Against HPV 16/18 Related CIN 2/3 or Worse (Protocol 015) GardasilN=6082PlaceboN=6075 PopulationN No. of cases IncidenceN IncidenceEfficacy (95% CI) PPE530100.05258210.3100% (75.8, 100%) MITT-35947670.659731111.039.2% (16.9, 55.8%) Incidence Rate: Calculated per 100 person years at risk. PPE: Naïve to relevant HPV type, received three doses of vaccine, cases counted after Month 7. MITT-3: Included regardless of baseline HPV status; received at least one dose of vaccine, cases counted 30 days post-dose 1. Sources: Table 7-2, p. 229; Table 7-5, p. 236, CSR 015v2
 PPE % (75.8, 100%) MITT % (16.9, 55.8%) Incidence Rate: Calculated per 100 person years at risk. PPE: Naïve to relevant HPV type, received three doses of vaccine, cases counted after Month 7. MITT-3: Included regardless of baseline HPV status; received at least one dose of vaccine, cases counted 30 days post-dose 1. Sources: Table 7-2, p. 229; Table 7-5, p. 236, CSR 015v2.")
31
31 Analysis of Efficacy Against HPV 16/18 Related CIN 2/3 or Worse (Protocols 005, 007, 013, 015) HPV L1 VLP Vaccine N=10268PlaceboN=10273 PopulationN No. of Cases IncidenceN IncidenceEfficacy (95% CI) PPE8487008460530.4100% (92.9, 100%) MITT-398311220.698962010.939.0% (23.3, 51.7%) Source: Table 2.7.3-cervixcancer: 29, p. 127-8
 PPE % (92.9, 100%) MITT % (23.3, 51.7%) Source: Table cervixcancer: 29, p")
32
32 Analysis of Efficacy of Against HPV 16/18 Related CIN 2/3 or Worse by HPV Type – MITT 3 Analysis (Protocols 005, 007, 013, 015) GardasilN=10268PlaceboN=10273 HPV Type N No. of cases IncidenceN IncidenceEfficacy (95% CI) HPV-1698311150.598961840.937.2% (20.3, 50.7%) HPV-18881470.048846330.278.7% (51.0, 92.0%) Source: Table 2.7.3-cervixcancer:31, p. 131
 HPV % (20.3, 50.7%) HPV % (51.0, 92.0%) Source: Table cervixcancer:31, p")
33
33 Efficacy Against HPV 6/11/16/18 CIN

34
34 Analysis of Efficacy Against HPV 6/11/16/18 Related CIN (Protocol 013) GardasilN=2717PlaceboN=2725 PopulationN No. of cases IncidenceN IncidenceEfficacy (95% CI) PPE2240002258371.0100% (87.4, 100%) MITT-32607651.226111132.042.9% (21.9, 58.6%) Source: Table 7-3, CSR 013v1, p. 240, Table 7-8. p 250.
 PPE % (87.4, 100%) MITT % (21.9, 58.6%) Source: Table 7-3, CSR 013v1, p. 240, Table 7-8. p")
35
35 Analysis of Efficacy Against HPV 6/11/16/18 Related CIN (Protocols 007, 013, 015) GardasilN=9075PlaceboN=9075 PopulationN No. of cases IncidenceN IncidenceEfficacy (95% CI) PPECombined785840.037861830.795.2% (87.2, 98.7%) MITT-3 Combined 88141701.088463171.846.4% (35.2, 55.7%) Source: Table2.7.3-cervixcancer: 26, p. 121-2
 PPECombined % (87.2, 98.7%) MITT-3 Combined % (35.2, 55.7%) Source: Table2.7.3-cervixcancer: 26, p")
36
36 Cases of HPV 6/11/16/18 Related CIN in PPE Population Four cases occurred in the Gardasil group for the PP analysis (Protocol 015). All four cases had HPV 16 related CIN 1 at Month 12-13. − −One subject had anti-HPV 16 level just below level of detection and LSIL at Day 1 and HSIL at Mo 7, and possibly had prior exposure to HPV 16; also non-naïve to HPV 18 at Day 1 and colposcopy triggered by the HSIL at Mo 7, led to a diagnosis of HPV 18 related CIN 3 at Mo 9. − −Three other subjects developed LSIL at Mo 7 and Mo 12, which led to colposcopies with the resulting diagnoses. One had anti-HPV 16 level at Mo 7 higher than GMT seen in Per Protocol Immunogenicity (PPI) population.
 population..")
37
37 Analysis of Efficacy Against HPV 6/11/16/18 Related CIN by HPV Type – MITT-3 (Protocols 005, 007, 013, 015) GardasilN=10572Placebo N= 10273 HPV Type N No. of cases IncidenceN No. of casesIncidenceEfficacy (95% CI) HPV 6/11 8814160.18846610.373.7% (53.8, 85.8%) HPV 16 101211550.798962781.345.6% (33.6, 55.6%) HPV 18 8814190.18846630.4 69.7% (48.8, 82.9%) Source: Table 2.7.3-cervixcancer:28, p. 126
 HPV 6/ % (53.8, 85.8%) HPV % (33.6, 55.6%) HPV % (48.8, 82.9%) Source: Table cervixcancer:28, p")
38
38 Efficacy Against HPV 6/11/16/18 Related CIN 2/3 or Worse and AIS (Protocols 005, 007, 013, and 015) GardasilPlacebo Day 1 Status N No. cases IncidenceN No. of cases Incidence Efficacy 95% CI MITT-39831 122 0.79896 201 0.9 39.0% (23.3, 51.7%) PCR (-) Sero (-) 9342 1 0.69400 81 0.4 98.8% (92.9, 100.0%) PCR (-) Sero (+) 853 0 0.0910 4 0.2 100% (-63.6, 100.0%) PCR (+) Sero (-) 661 42 3.2626 57 4.6 31.2% (-4.5, 54.9%) PCR (+) Sero (+) 473 79 [121] * 9.1499 69 [130] * 7.3 -25.8% (-76.4, 10.1%) * Total number of cases in subjects who were sero+ and/or PCR+ at baseline for the relevant HPV type which was associated with disease. Source: Table 1-1, Additional efficacy analysis requested by CBER
 PCR (-) Sero (-) % (92.9, 100.0%) PCR (-) Sero (+) % (-63.6, 100.0%) PCR (+) Sero (-) % (-4.5, 54.9%) PCR (+) Sero (+) [121] * [130] * % (-76.4, 10.1%) * Total number of cases in subjects who were sero+ and/or PCR+ at baseline for the relevant HPV type which was associated with disease. Source: Table 1-1, Additional efficacy analysis requested by CBER.")
39
39 Selected Characteristics for Subgroup of Vaccine Related HPV PCR Positive and Seropositive Subjects at Day 1 (Protocol 013) GardasilPlacebo Subgroup Population 156137 History of cervicovaginal infection or STD 35.9%32.1% Pap test with HSIL 6.5%3.7% Source: Table 2a-2, Response to CBER questions from 3/1/06.
 GardasilPlacebo Subgroup Population History of cervicovaginal infection or STD 35.9%32.1% Pap test with HSIL 6.5%3.7% Source: Table 2a-2, Response to CBER questions from 3/1/06.")
40
40 Efficacy Against Any HPV Type and Non-Vaccine HPV Type Related CIN

41
41 Overall Impact on CIN 2/3 or Worse Due to Any HPV Type (Protocols 007, 013, and 015) GardasilN=9075Placebo N= 9075 PopulationN No. of cases IncidenceN No. of casesIncidenceEfficacy (95% CI) MITT-388142871.688463281.912.2% (-3.2, 25.3%) Source: Table 5.3.5.3.2:17, p. 78-9, Integrated Summary of Efficacy
 MITT % (-3.2, 25.3%) Source: Table :17, p. 78-9, Integrated Summary of Efficacy.")
42
42 Analysis of Efficacy Against Non-HPV 6/11/16/18 Related CIN 2 or CIN 3 Among Subjects in All MITT-1 Population (Protocols 007, 013, 015) GardasilN=9075Placebo N= 9075 N No. of cases IncidenceN No. of casesIncidenceEfficacy (95% CI) CIN 2 5993590.75766490.6-16.1% (-73.2, 21.8%) CIN 3 5993360.45766270.3-28.5% (-120.1, 24.1%) All MITT-1 Population: Naïve to all four vaccine HPV types through Month 7, received three doses of vaccine. Source: Table 3-4, Additional Efficacy Analyses Requested by CBER
 CIN % (-73.2, 21.8%) CIN % (-120.1, 24.1%) All MITT-1 Population: Naïve to all four vaccine HPV types through Month 7, received three doses of vaccine. Source: Table 3-4, Additional Efficacy Analyses Requested by CBER.")
43
43 Efficacy Against HPV 6/11/16/18 Related External Genital Lesions (EGLs)
")
44
44 Analysis of Efficacy Against HPV 6/11/16/18 EGL (Protocol 013) GardasilN=2717PlaceboN=2725 PopulationN No. of cases IncidenceN IncidenceEfficacy (95% CI) PPE226100.02279401.0100% (88.4, 100%) MITT-32671260.52668801.467.8% (49.3, 80.1%) Source: Table 7-3, CSR 013v1, p. 240 and Table 7-18, p. 271
 PPE % (88.4, 100%) MITT % (49.3, 80.1%) Source: Table 7-3, CSR 013v1, p. 240 and Table 7-18, p")
45
45 Analysis of Efficacy Against HPV 6/11/16/18 Related EGLs (Protocols 007, 013, 015) GardasilN=9075Placebo N= 9075 PopulationN No. of cases IncidenceN No. of casesIncidenceEfficacy (95% CI) PPE798710.0178991130.999.1% (95.0, 100.0%) RMITT-2574260.157751271.195.3% (89.4, 98.3%) MITT-38954680.489622291.370.4% (61.0, 77.7%) Source: Table2.7.3-exgenlesions: 6, p. 39-40 Table 4-1, Additional Efficacy Analyses Requested by CBER
 PPE % (95.0, 100.0%) RMITT % (89.4, 98.3%) MITT % (61.0, 77.7%) Source: Table2.7.3-exgenlesions: 6, p Table 4-1, Additional Efficacy Analyses Requested by CBER.")
46
46 Analysis of Efficacy Against HPV 6/11/16/18 Related EGLs by HPV Type (Protocols 007, 013, 015) Gardasil N=9075 Placebo N= 9075 N No. of cases IncidenceN No. of cases Incidence Efficacy (95% CI) MITT-3 HPV 6/11 8954590.389621941.1 69.6% (59.2, 77.7%) MITT-3 HPV 16 8954110.18962551.1 80.0% (61.3, 90.5%) MITT-3 HPV 18 895420.018962200.1 90.0% (58.7, 98.9%) Source: Appendix 2.7.3-exgenlesions:9, p. 64
 MITT-3 HPV 6/ % (59.2, 77.7%) MITT-3 HPV % (61.3, 90.5%) MITT-3 HPV % (58.7, 98.9%) Source: Appendix exgenlesions:9, p. 64.")
47
47 Analysis of Efficacy Against HPV 16/18 Related EGLs (Protocols 007, 013, 015) GardasilN=9075Placebo N= 9075 Population - EGL type N No. of cases IncidenceN No. of casesIncidenceEfficacy (95% CI) PPE - Condyloma, VIN 1 or VaIN 1) 776900.07741240.2100.0% (83.4, 100.0%) PPE - VIN 2/3 or VaIN 2/3 or worse) 776900.07741100.1100.0% (55.5, 100.0%) MITT-3 - Condyloma, VIN 1 or VaIN 1) 895470.048962510.386.2% (69.6, 94.7%) MITT-3 – VIN 2/3 or VaIN 2/3 or worse) 895480.058962260.169.1% (29.8, 87.9%) Source: Table 2.7.3-exgenlesions:7, p. 41
 PPE - Condyloma, VIN 1 or VaIN 1) % (83.4, 100.0%) PPE - VIN 2/3 or VaIN 2/3 or worse) % (55.5, 100.0%) MITT-3 - Condyloma, VIN 1 or VaIN 1) % (69.6, 94.7%) MITT-3 – VIN 2/3 or VaIN 2/3 or worse) % (29.8, 87.9%) Source: Table exgenlesions:7, p. 41.")
48
48 Analysis of Efficacy Against HPV 6/11/16/18 Related EGL by Severity of Disease – PPE Population (Protocols 007, 013, 015) GardasilN=9075Placebo N= 9075 Population - EGL type N No. of cases IncidenceN No. of casesIncidenceEfficacy (95% CI) PPE - Condyloma 789710.07899910.898.9% (93.7, 100.0%) PPE – VIN 1 789700.07899100.1100.0% (55.4, 100.0%) PPE-VIN 2/3 789700.0789980.1100.0% (41.4, 100.0%) PPE-VaIN 2/3 789700.0789950.04100.0% (<0.0, 100.0%) Source: Table 1-1, Response to CBER request 5/1/06.
 PPE - Condyloma % (93.7, 100.0%) PPE – VIN % (55.4, 100.0%) PPE-VIN 2/ % (41.4, 100.0%) PPE-VaIN 2/ % (<0.0, 100.0%) Source: Table 1-1, Response to CBER request 5/1/06..")
49
49 Analysis of Efficacy Against HPV 6/11/16/18 Related EGL by Severity of Disease – MITT-3 population (Protocols 007, 013, 015) GardasilN=9075Placebo N= 9075 Population - EGL type N No. of cases IncidenceN No. of casesIncidenceEfficacy (95% CI) MITT-3 Condyloma 8954580.389621841.068.5% (57.5, 77.0%) MITT-3 VIN 1 895480.058962190.157.8% (<0.0, 84.0%) MITT-3 VIN 2/3 895470.048962220.168.1% (22.7, 88.5%) MITT-3 VaIN 2/3 895420.01896290.177.7% (<0.0, 97.7%) Source: Table 1-3, CBER Additional Request for analyses, 5/1/06
 MITT-3 Condyloma % (57.5, 77.0%) MITT-3 VIN % (<0.0, 84.0%) MITT-3 VIN 2/ % (22.7, 88.5%) MITT-3 VaIN 2/ % (<0.0, 97.7%) Source: Table 1-3, CBER Additional Request for analyses, 5/1/06.")
50
50 Efficacy Against HPV 6/11/16/18 Related EGLs (Protocols 007, 013, and 015) GardasilN=9075Placebo N= 9075 Day 1 Status N No. of cases IncidenceN No. of casesIncidenceEfficacy (95% CI) Sero (-) PCR (+) 810442.9782412.8-4.0% (-63.2, 33.6%) Sero (+) PCR (-) 127000.0130140.2100.0% (-56.2, 100.0%) Sero (+) PCR (+) 3365[49]*1.03315[50]*1.02.4% (-324.3, 77.5%) * Total number of cases in subjects who were sero+ and/or PCR + at baseline for the relevant HPV type which was associated with disease. Source: Table 2.7.3-exgenlesions:8, p. 43 and Table 7-1, Additional Efficacy Analyses Requested by CBER
 Sero (-) PCR (+) % (-63.2, 33.6%) Sero (+) PCR (-) % (-56.2, 100.0%) Sero (+) PCR (+) 3365[49]* [50]*1.02.4% (-324.3, 77.5%) * Total number of cases in subjects who were sero+ and/or PCR + at baseline for the relevant HPV type which was associated with disease. Source: Table exgenlesions:8, p. 43 and Table 7-1, Additional Efficacy Analyses Requested by CBER.")
51
51 Impact of Gardasil on Incidence of EGLs Due to Any HPV Type by Severity of Disease (Protocols 007, 013, 015) GardasilN=9075Placebo N= 9075 N No. of cases IncidenceN No. of casesIncidenceEfficacy (95% CI) RMITT 2 condylomata, VIN 1 or VaIN 1 5734520.557691511.365.4% (52.3, 75.3%) RMITT 2- VIN 2/3 or VaIN 2/3 or worse 573450.045769270.281.3% (50.8, 94.4%) MITT-3 – condylomata, VIN 1 or VaIN 1 89541691.089622841.640.5% (27.8, 51.1%) MITT-3 – VIN 2/3 or VaIN 2/3 or worse 8954220.18962430.248.7% (12.3, 70.8%) Source: Table 2.7.3-exgenlesions: 9, p. 46
 RMITT 2 condylomata, VIN 1 or VaIN % (52.3, 75.3%) RMITT 2- VIN 2/3 or VaIN 2/3 or worse % (50.8, 94.4%) MITT-3 – condylomata, VIN 1 or VaIN % (27.8, 51.1%) MITT-3 – VIN 2/3 or VaIN 2/3 or worse % (12.3, 70.8%) Source: Table exgenlesions: 9, p. 46.")
52
52 Efficacy Against Non-HPV 6/11/16/18 Related EGL in All MITT-1 Population (Protocols 007, 013, 015) GardasilN=9075PlaceboN=9075 N No. of cases IncidenceN IncidenceEfficacy (95% CI) EGL not related to HPV 6/11/16/18 5999520.65773490.6-2.1% (-54.1, 32.2%) Condyloma, VIN 1, VaIN 1 5999460.55773490.69.7% (-37.9, 40.9%) VIN 2/3 or VaIN 2/3 599950.1577360.119.8% (-215.3, 80.6%) Vulvar or vaginal cancer 599910.01577300.0NA Source: Table 6-2, Additional Efficacy Analyses Requested by CBER
 EGL not related to HPV 6/11/16/ % (-54.1, 32.2%) Condyloma, VIN 1, VaIN % (-37.9, 40.9%) VIN 2/3 or VaIN 2/ % (-215.3, 80.6%) Vulvar or vaginal cancer NA Source: Table 6-2, Additional Efficacy Analyses Requested by CBER.")
53
53 Safety Safety Population Safety Surveillance DeathsSAEsPregnancies/Lactation

54
54 Safety Population: Detailed and General Safety Population GardasilPlacebo Detailed Safety Population 61604064 General Safety Population 117789686 Source: Tables 2.7.4: 4 and 5, p. 29-30, Summary of Clinical Safety 3/8/06

55
55 Vaccine Exposure in 9-15 Year Old Female Subjects (Protocols 016 and 018) Age Females Gardasil 985 10158 11196 12165 13190 14192 15137 Total1123 Source: Applicant’s response to additional CBER questions
 Age Females Gardasil Total1123 Source: Applicant’s response to additional CBER questions")
56
56 Safety Surveillance (Detailed Safety Cohort) Vaccine Report Cards for 14 days after each vaccination (Protocols 005, 007, 013 + NSAE 015) – –Solicited local AEs: Pain, tenderness, redness for 5 days after vaccination – –Temperatures for 5 days after vaccination > 100° F oral – –Solicited and unsolicited systemic AEs: Sore muscle, sore joints, headache, rash, diarrhea for 14 days after vaccination
 Vaccine Report Cards for 14 days after each vaccination (Protocols 005, 007, NSAE 015) – –Solicited local AEs: Pain, tenderness, redness for 5 days after vaccination – –Temperatures for 5 days after vaccination > 100° F oral – –Solicited and unsolicited systemic AEs: Sore muscle, sore joints, headache, rash, diarrhea for 14 days after vaccination")
57
57 Serious Adverse Event Reporting Any SAE for day of consent to 14 days postdose 1, and 14 days postdose 2 and 3 regardless of attribution Any death or SAE which resulted in study discontinuation Any SAE throughout study which was possibly vaccine or procedure related or whose relationship was unclear Pregnancy related SAEs throughout study Source: Applicant’s Response to CBER question

58
58 Reporting New Medical Conditions Pre-vaccination Study period through Month 7 Study period after Month 7

59
59 Pregnancy and Lactation Reporting All pregnancies were to be followed to outcome SAEs were reported for mothers and infants Lactation outcomes were followed

60
60 Safety Results

61
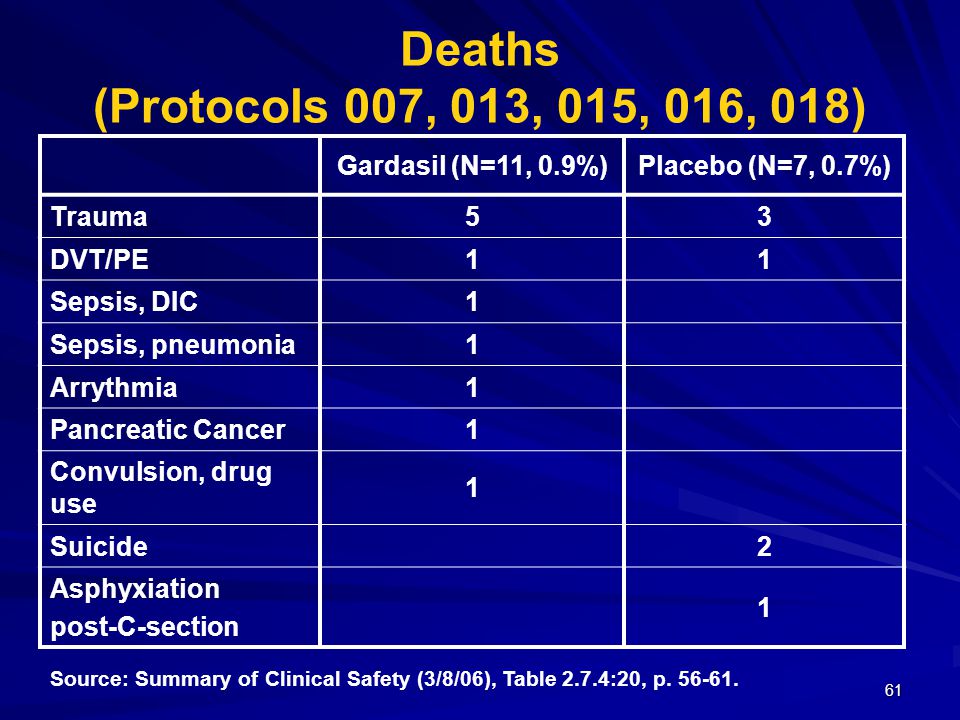
61 Deaths (Protocols 007, 013, 015, 016, 018) Gardasil (N=11, 0.9%)Placebo (N=7, 0.7%) Trauma53 DVT/PE11 Sepsis, DIC1 Sepsis, pneumonia1 Arrythmia1 Pancreatic Cancer1 Convulsion, drug use 1 Suicide2 Asphyxiation post-C-section 1 Source: Summary of Clinical Safety (3/8/06), Table 2.7.4:20, p. 56-61.
62
62 Serious Adverse Events (Protocols 007, 013, 015, 016, 018) SAE (Organ system)Gardasil N=11778Placebo N=9680 Gyn or Obstetrical4241 GI116 Appendicitis41 Injury66 Neurological47 Immune mediated24 Coagulation/DVT21 Pulmonary25 GU65 Endocrine10 Injection site reaction10 Psychiatric52 Cardiovascular11 Musculoskeletal11 ENT10 Administration of excess study vaccine 1620 Total101 (0.9%)97 (1.0%) Source: Summary of Clinical Efficacy (3/8/06) Table 2.7.4:21, p. 63-102.

63
63 New Medical Conditions (Number and Percent) During Vaccination Period (through Month 7) and after Month 7 for Selected Organ Systems (Protocols 007, 013, 015, 016, 018) Organ SystemDuring Vaccination PeriodPost Month 7 Gardasil N=11778 Placebo N=9868 Gardasil N=10452 Placebo N=9385 Cardiac11 (0.1%)12 (0.1%)21 (0.2%)13 (0.1%) Endocrine20 (0.2%)17 (0.2%)40 (0.4%)33 (0.4%) GI711 (6.0%)638 (6.6%)7272 (7.0%)595 (6.3%) Immune150 (1.3%)112 (1.2%)105 (1.0%)88 (0.9%) Musculoskeletal387 (3.3%)256 (2.6%)320 (3.1%)242 (2.6%) Neoplasms68 (0.6%)50 (0.5%)105 (1.0%)67 (0.7%) Nervous system684 (5.8%)495 (5.1%)333 (3.2%)217 (2.3%) Psychiatric168 (1.4%)162 (1.7%)212 (2.2%)203 (2.2%) Surgical384 (3.3%)296 (3.1%)477 (4.6%)495 (5.3%) Appendectomy19 (0.2%)4 (<0.1%)17 (0.2%)26 (0.3%) Source: Summary of Clinical Efficacy (3/8/06): Appendices 2.7.4: 31, 33, 34, 36
 During Vaccination Period (through Month 7) and after Month 7 for Selected Organ Systems (Protocols 007, 013, 015, 016, 018) Organ SystemDuring Vaccination PeriodPost Month 7 Gardasil N=11778 Placebo N=9868 Gardasil N=10452 Placebo N=9385 Cardiac11 (0.1%)12 (0.1%)21 (0.2%)13 (0.1%) Endocrine20 (0.2%)17 (0.2%)40 (0.4%)33 (0.4%) GI711 (6.0%)638 (6.6%)7272 (7.0%)595 (6.3%) Immune150 (1.3%)112 (1.2%)105 (1.0%)88 (0.9%) Musculoskeletal387 (3.3%)256 (2.6%)320 (3.1%)242 (2.6%) Neoplasms68 (0.6%)50 (0.5%)105 (1.0%)67 (0.7%) Nervous system684 (5.8%)495 (5.1%)333 (3.2%)217 (2.3%) Psychiatric168 (1.4%)162 (1.7%)212 (2.2%)203 (2.2%) Surgical384 (3.3%)296 (3.1%)477 (4.6%)495 (5.3%) Appendectomy19 (0.2%)4 (<0.1%)17 (0.2%)26 (0.3%) Source: Summary of Clinical Efficacy (3/8/06): Appendices 2.7.4: 31, 33, 34, 36")
64
64 Pregnancy Outcome Summary (Protocols 013, 015, 016, 018) Gardasil (N=10418) Placebo (N=9120) Subjects with pregnancies 1115 (10.7%) 1151 (12.6%) Number of pregnancies 12441272 Number of fetuses/infants with known outcomes 9961018 Number of pregnancies with unknown outcomes 258263 Live Births 621 (62.3%) 611 (60.0%) Spontaneous miscarriage 249 (25%)* 257 (25.2%)* Late fetal deaths 11 (1.2%) 8 (0.9%) *Percentage calculated with number of known outcomes Source: Summary of Clinical Safety (3/8/06), Table 2.7.4:24, p. 126-8.

65
65 Distribution of Congenital Anomalies by Estimated Dates of Conception (EDCn) Timing in Relation to Vaccination (Protocols 013, 015, 016, 018)GardasilPlacebo Congenital Anomalies 1516 EDCn within 30 days of study vaccine 5**0 Live birth reported in neonatal period 50 EDCn beyond 30 days of study vaccine 1016 Live birth reported in neonatal period 812 Live birth reported beyond neonatal period 11 Fetal Loss Fetal Loss02 Intra-uterine diagnosis Intra-uterine diagnosis11 **Diagnoses included hip dysplasia, ankyloglossia and pyloric stenosis, congenital hydronephrosis, club foot, and congenital megacolon Source: Table 2.7.4:26, p. 135, safety update 3/8/06

66
66 Adverse Events in Pregnancy/Lactation (1) (Protocols 013, 015, 016, 018) A similar pattern and occurrence of SAEs and AEs in pregnancy were reported in women who were vaccinated with Gardasil (N=40, 4.2%) or placebo (N=41, 4.3%). – –These events included conditions leading to C-section, premature labor, and conditions associated with pregnancy.

67
67 Adverse Events in Pregnancy/Lactation (2) (Protocols 013, 015, 016) Higher proportion of children with SAEs in women who received Gardasil while breastfeeding in the vaccination period (Gardasil N=17, 3.4%; placebo N=9, 1.8%); the events were of similar nature in both groups. –In both the vaccine and placebo groups, these included respiratory infections, gastroenteritis, and asthma.

68
68 Adverse Events in Infants/Lactation(3) (Protocols 013, 015, 016) EventGardasilN=500PlaceboN=495 Respiratory Infections 124 Gastroenteritis/Diarrhea 52 Asthma 11 Bronchial Obstruction 10 Cellulitis10 Dehydration10 Head Injury 10 Anomalous pulmonary venous return 10 Unspecified Viral Infection 01 Febrile Convulsion 01 Source: Summary of Clinical Safety, Page 181-182 and Appendix 2.7.4:195, Pages 1076-1079
 (Protocols 013, 015, 016) EventGardasilN=500PlaceboN=495 Respiratory Infections 124 Gastroenteritis/Diarrhea 52 Asthma 11 Bronchial Obstruction 10 Cellulitis10 Dehydration10 Head Injury 10 Anomalous pulmonary venous return 10 Unspecified Viral Infection 01 Febrile Convulsion 01 Source: Summary of Clinical Safety, Page and Appendix 2.7.4:195, Pages")
69
69 FDA Safety Conclusion (1) Although no obvious safety signal was identified, post-marketing pharmacovigilance activities will continue to collect AEs that occur post-vaccination in a larger population.
 Although no obvious safety signal was identified, post-marketing pharmacovigilance activities will continue to collect AEs that occur post-vaccination in a larger population.")
70
70 FDA Safety Conclusion (2) An imbalance was noted regarding the EDCn of infants who had congenital anomalies (five cases for mothers who received Gardasil vs. none for mothers who received placebo). However, there did not appear to be a pattern among the congenital anomalies.
. However, there did not appear to be a pattern among the congenital anomalies..")
71
71 Immunogenicity Bridging immune response in adolescent girls to adult women Duration of immune response Co-administration with Hepatitis B vaccine

72
72 Bridging Immune Response from Females 16-26 Years to Females 9-15 Years of Age Females naïve to the four vaccine HPV types are expected to benefit most from the vaccine. Efficacy studies cannot be conducted in preadolescent girls.

73
73 Month 7 HPV 6 GMTs and 95% CI by Age at Enrollment - 9 to 26 Year Old Female Recipients of Gardasil (PPI) Source: Figure 5.3.5.3.3:3, Integrated Summary of Immunogenicity
 Source: Figure :3, Integrated Summary of Immunogenicity")
74
74 Immunogenicity Bridging Between 9-15 Year Old Females in the Immunogenicity Studies to 16-26 Year Old Females in the Efficacy Studies (PPI) 9-15 Year Old Females in Protocols 016 and 018 16-23 Year Old subjects in Protocols 013 and 015 Assay (cLIA) nGMTmMU/mL 95% CI nGMTmMU/mL Anti-HPV 6 927931.3 876.9, 989.2 2827542.4 526.6, 558.7 Anti-HPV 11 9271305.7 1226.2, 1390.4 2827766.1 740.5, 792.6 Anti-HPV 16 9294944.9 4538.5, 5334.8 27072313.8 2206.2, 2426.7 Anti-HPV 18 9321046.0 971.2, 1126.5 3040460.7 443.8, 478.3 Source: Table 5.3.5.3.3:29, p. 85, Integrated Summary of Immunogenicity

75
75 Duration of Immune Response

76
76 Persistence of Anti-HPV 18 Immune Responses in 18 to 26 Year Old Female Recipients of Gardasil (Seronegative at Day 1 and PCR Negative Through Month 7) Versus Placebo Recipients (Seropositive and PCR Negative at Day 1) Source: Figure 5.3.5.3.3:16, p. 69, Integrated Summary of Immunogenicity

77
77 Seropositivity Rates for Anti-HPV 6, 11, 16, and 18 at Month 24 (Vaccinated Women 18-26 years) with Serology Data at All Time Points (N=2818) HPV type Seropositivity rate at Month 24 (95% CI) Anti-HPV 6 95.7% (94.5, 96.6%) Anti-HPV 11 97.6% (96.8, 98.3%) Anti-HPV 16 99.6% (99.2, 99.9%) Anti-HPV 18 73.9% (71.8, 75.9%) Source: Table 5.3.5.3.3:14, p. 55, Integrated Summary of Immunogenicity

78
78 Co-administration of Gardasil with Hepatitis B Vaccine Anti-HPV 6, 11, 16, and 18 immune responses were non-inferior when Gardasil was given with or without Recombivax (SC rates, GMT ratios) Anti-Hepatitis B immune response was similar when Recombivax was given with or without Gardasil (SC rates) –Anti-Hep B GMTs lower in coadministration group
 Anti-Hepatitis B immune response was similar when Recombivax was given with or without Gardasil (SC rates) –Anti-Hep B GMTs lower in coadministration group")
79
79 Applicant’s Proposed Post-marketing Commitments Routine pharmacovigilance Phase 4 studies Other studies

80
80 Routine Pharmacovigilance Passive reporting of adverse events (AEs) including: Monthly submission of non-serious AE reports Regular FDA-CDC-Sponsor conference calls Pregnancy registry
 including: Monthly submission of non-serious AE reports Regular FDA-CDC-Sponsor conference calls Pregnancy registry")
81
81 Phase 4 Studies Observational safety surveillance study in large U.S. MCO Investigation of serious AEs that occur in close temporal association with vaccination (60 days follow-up) Nordic Long Term Follow-up Study Longitudinal evaluation of subjects in Protocol 015 enrolled in Nordic countries using national registries
 Nordic Long Term Follow-up Study Longitudinal evaluation of subjects in Protocol 015 enrolled in Nordic countries using national registries.")
82
82 Nordic Long Term Follow-up Study: Outcomes HPV-related diseases Long term effectiveness and duration of immune response Potential safety signals Pregnancy outcomes

83
83 Other Studies Evaluation of long term effectivenesss and duration of immune response: Extension of protocol 007 Extension of protocol 018 Detection of unanticipated safety signals through active surveillance in all studies.

84
84 Gardasil: FDA Review Conclusions The efficacy, safety, and “bridging” immune response data submitted to the BLA support licensure of Gardasil in females 9-26 years of age naïve to the relevant vaccine HPV type for prevention of the following diseases/events: –HPV 16/18 related cervical cancer, CIN 2/3 and AIS. –HPV 6/11/16/18 related VIN 2, VIN 3, VaIN 2, VaIN 3 –HPV 6/11/16/18 related CIN 1, genital warts, VIN 1 and VaIN 1

85
85 Gardasil: FDA Review Concerns (1) Applicant’s Per Protocol HPV type-specific analyses that indicated a very high level of efficacy in naïve subjects may not reflect the efficacy of Gardasil for all HPV related disease on a population basis. HPV related disease occurred in Gardasil recipients. − −Some vaccine recipients were non-naïve at baseline for one or more vaccine HPV type(s), and some of these subjects developed HPV disease related to that HPV type(s). − −Subjects who were naïve to all four vaccine HPV types could still develop disease related to an HPV type not included in the vaccine.
, and some of these subjects developed HPV disease related to that HPV type(s). − −Subjects who were naïve to all four vaccine HPV types could still develop disease related to an HPV type not included in the vaccine..")
86
86 Gardasil: FDA Review Concerns (2) Modified Intent to Treat analysis (MITT-3) of all vaccinated females across studies 005, 007, 013, and 015 demonstrate modest efficacy against CIN 2/3: – due to [39.0% (23.5, 51.7%)] –MITT-3: Overall efficacy CIN 2/3 or worse due to HPV6/11/16/18 [39.0% (23.5, 51.7%)] –MITT-3: Overall efficacy CIN 2/3 or worse due to any HPV type [ –MITT-3: Overall efficacy CIN 2/3 or worse due to any HPV type [12.2% (-3.2%, 25.3%)]. (-3.2%, 25.3%)].
![86 Gardasil: FDA Review Concerns (2) Modified Intent to Treat analysis (MITT-3) of all vaccinated females across studies 005, 007, 013, and 015 demonstrate modest efficacy against CIN 2/3: – due to [39.0% (23.5, 51.7%)] –MITT-3: Overall efficacy CIN 2/3 or worse due to HPV6/11/16/18 [39.0% (23.5, 51.7%)] –MITT-3: Overall efficacy CIN 2/3 or worse due to any HPV type [ –MITT-3: Overall efficacy CIN 2/3 or worse due to any HPV type [12.2% (-3.2%, 25.3%)].](http://images.slideplayer.com/12/3347513/slides/slide_86.jpg "(-3.2%, 25.3%)]..")
87
87 Gardasil: FDA Review Concerns (3) Longer-term efficacy –Study 005 results suggest favorable longer term efficacy Duration of immune response –Post-licensure commitments
 Longer-term efficacy –Study 005 results suggest favorable longer term efficacy Duration of immune response –Post-licensure commitments")
88
88 Questions for the Committee 1. Do the data from studies 005, 007, 013, and 015 support the efficacy of Gardasil for the prevention of HPV 16/18 related cervical cancer, cervical AIS, and CIN 2/3 or worse in females 16-26 years of age?

89
89 Questions for the Committee 2. Do the data from studies 007, 013, and 015 support the efficacy of Gardasil for the prevention of HPV 6/11/16/18 related VIN 2/3 and VaIN 2/3 in females 16-26 years of age?

90
90 Questions for the Committee 3. Do the data from studies 007, 013, and 015 support the efficacy of Gardasil for the prevention of HPV 6/11/16/18 related condyloma acuminata, VIN 1 and VaIN 1?

91
91 Questions for the Committee 4. Do the immunogenicity data support bridging of the younger female population (9-15 years of age) to the efficacy population (females 16-26 years of age)?
 to the efficacy population (females years of age) .")
92
92 Questions for the Committee 5. Do the safety data from studies 007, 013, 015, 016 and 018 support the safety of Gardasil for use in females 9-26 years of age?

93
93 Questions for the Committee 6. Please comment on post-marketing commitments.

Similar presentations

: The Background, Current Status and Future of Vaccines to Prevent HPV Infection, Abnormal Genital Lesions and Cervical Cancer.>")


 BLA 125348 FDA Clinical Review Agnes Lim, MD Yao-Yao Zhu, MD, PhD DCEPT/OCTGT/CBER, FDA October 9, 2009 Advisory Committee Meeting.>")














