Download presentation
Presentation is loading. Please wait.

1
Grading Criteria Changes New Pathway 2012 Robert Brown & Yvonne D’Souza SMDESP – June 2012

2
New Pathway diagram

3
How will it effect SMDESP? Removal of 6/12 Re-screen Discontinuation of R1.5 & M0.5 OPDR – Virtual Surveillance Clinic Clarity in grading criteria

4
Retinopathy Grading Criteria R0NoneNo DR R1Backgroundmicroaneurysm(s) or HMa* retinal haemorrhage(s) venous loop any exudate in the presence of other non-referable features of DR any number of cotton wool spots (CWS) in the presence of other non- referable features of DR
 or HMa* retinal haemorrhage(s) venous loop any exudate in the presence of other non-referable features of DR any number of cotton wool spots (CWS) in the presence of other non- referable features of DR")
5
Grading changes in the new pathway Defining the R2 pre-proliferative level Defining groups of exudates Introducing a stable treated R3 grade Simplifying image quality into adequate and inadequate (no longer a ‘good’category)
")
6
The R2 Pre-proliferative level Venous beading Venous reduplication Multiple blot haemorrhages IRMA New definition

7
OPDR Pathway Pregnant women Patients who require increased level of surveillance Patients discharged from HES More frequent photography + OCT

10
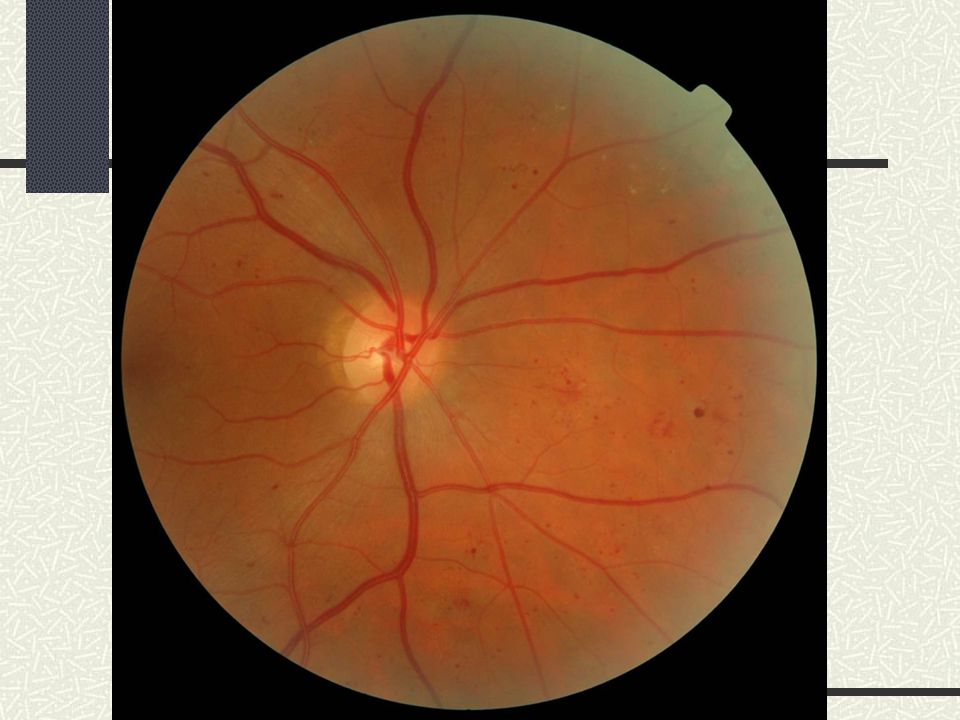
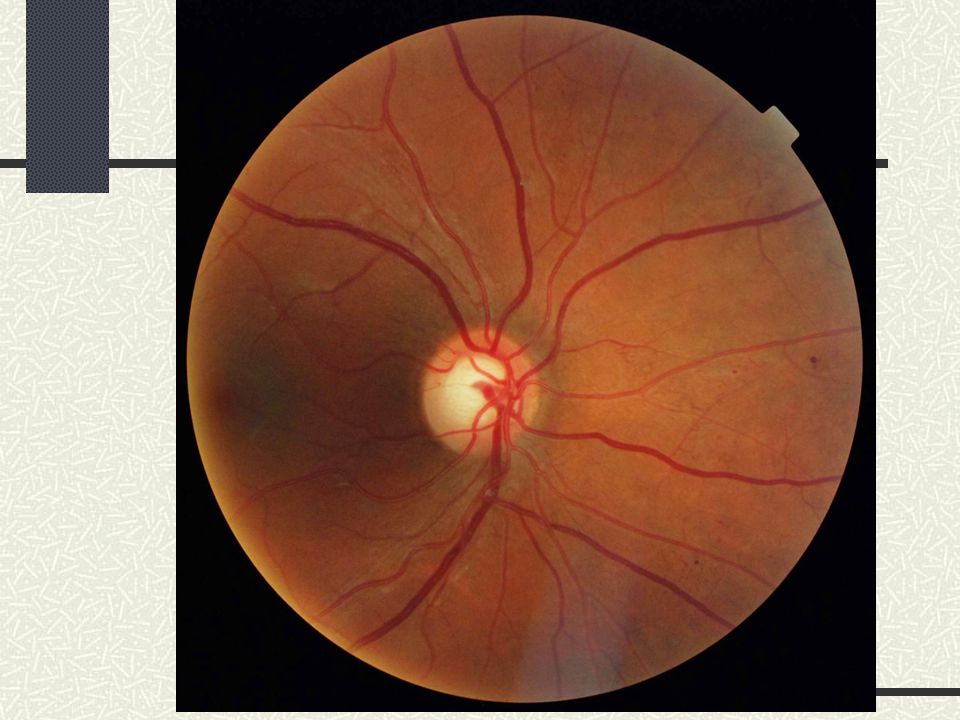
Referable

19
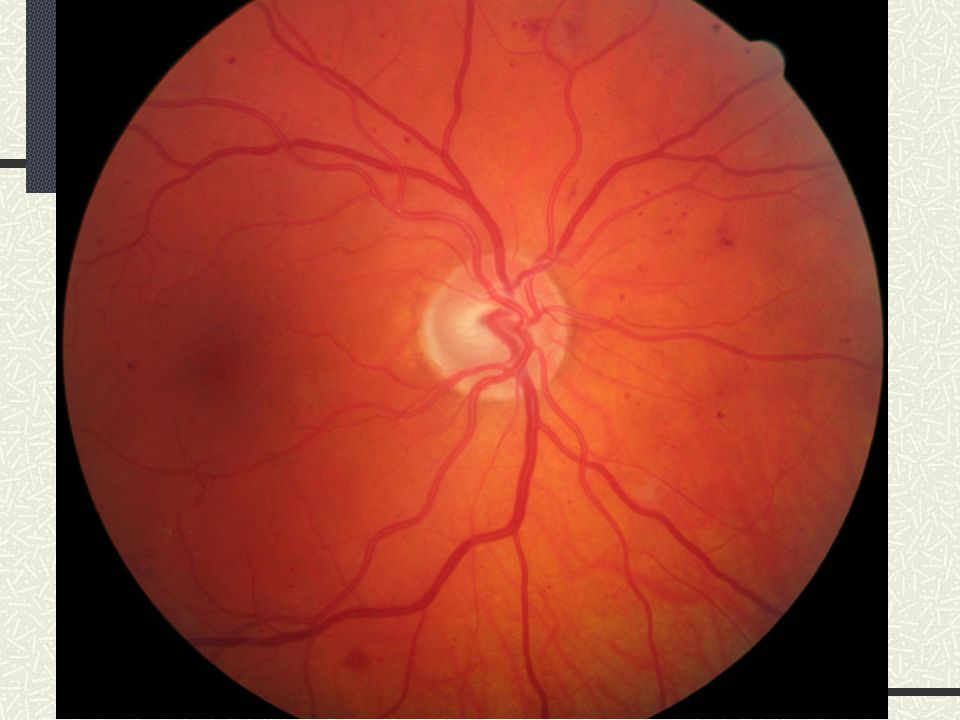
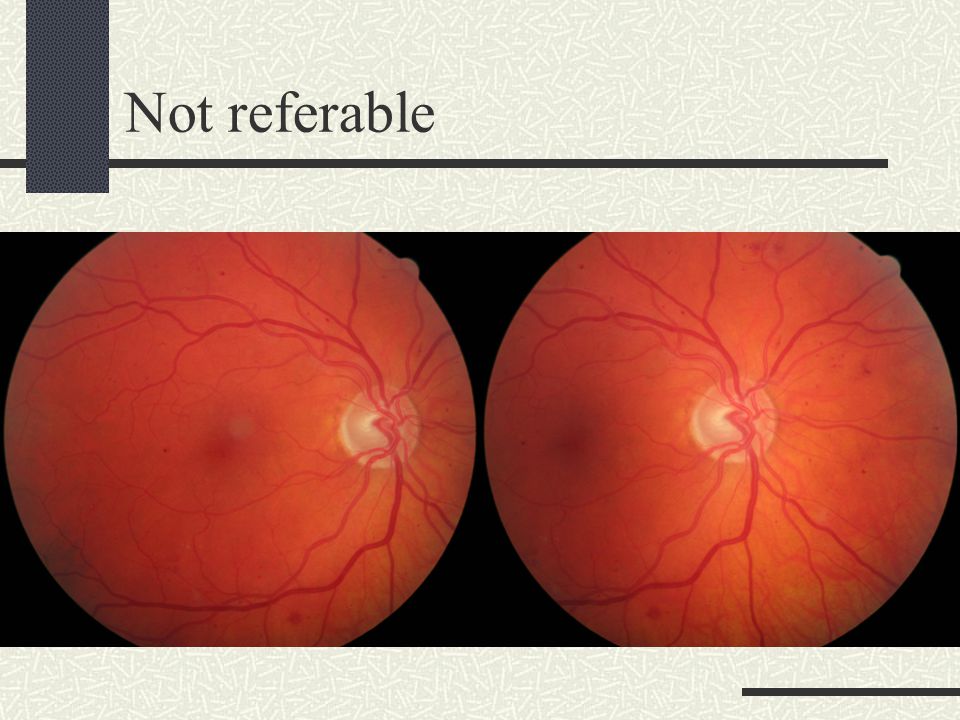
Not referable

26
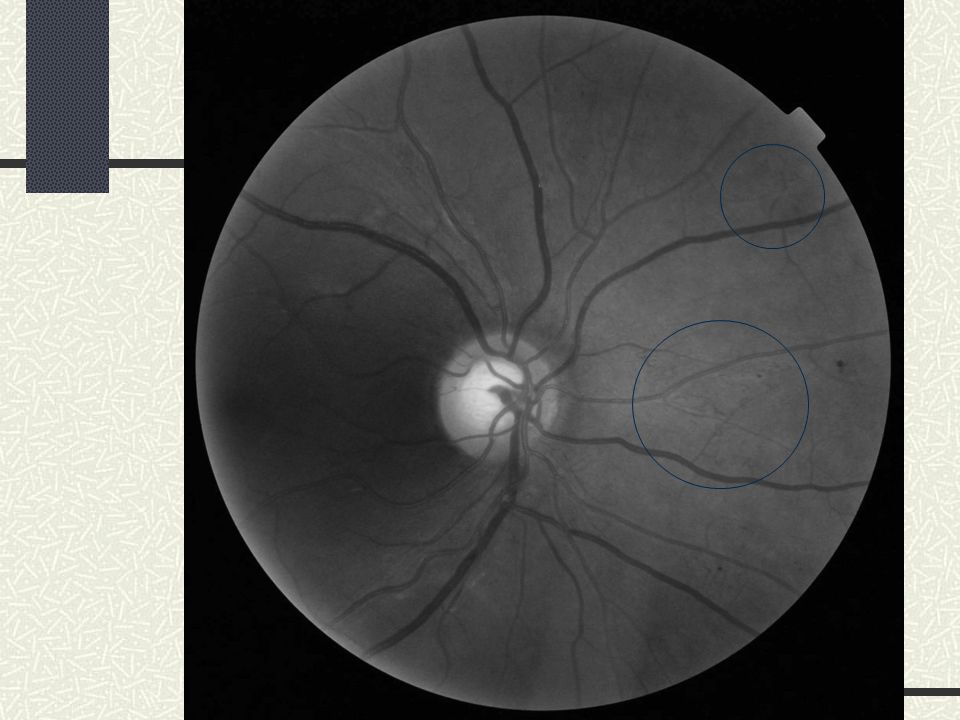
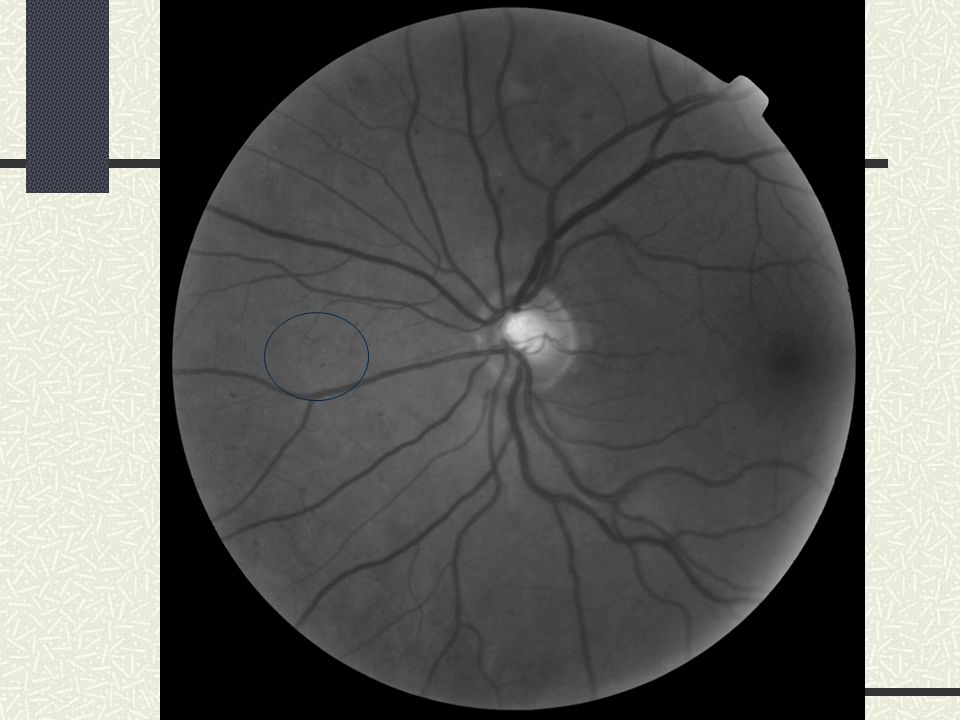
IRMA – Intraretinal microvascular abnormalities The amount of haemorrhage present in the following image sets does not warrant a referral. However, a careful search for IRMA should be made when the amount of haemorrhages is equal to that shown in the images. Patients with IRMA that are definitely seen should be referred into the Hospital Eye Service.

35
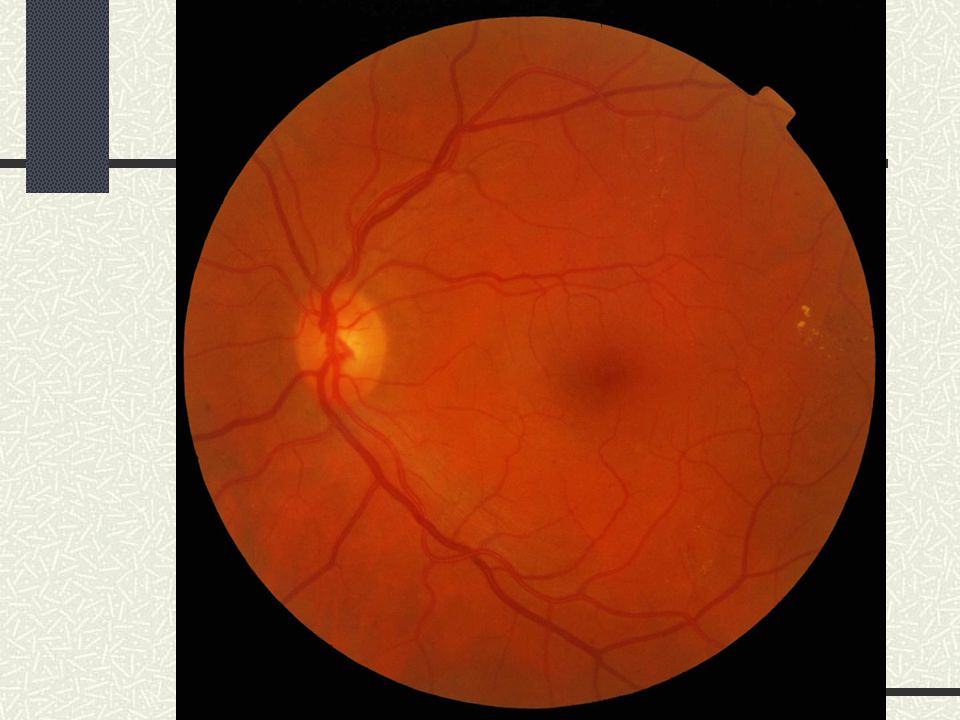
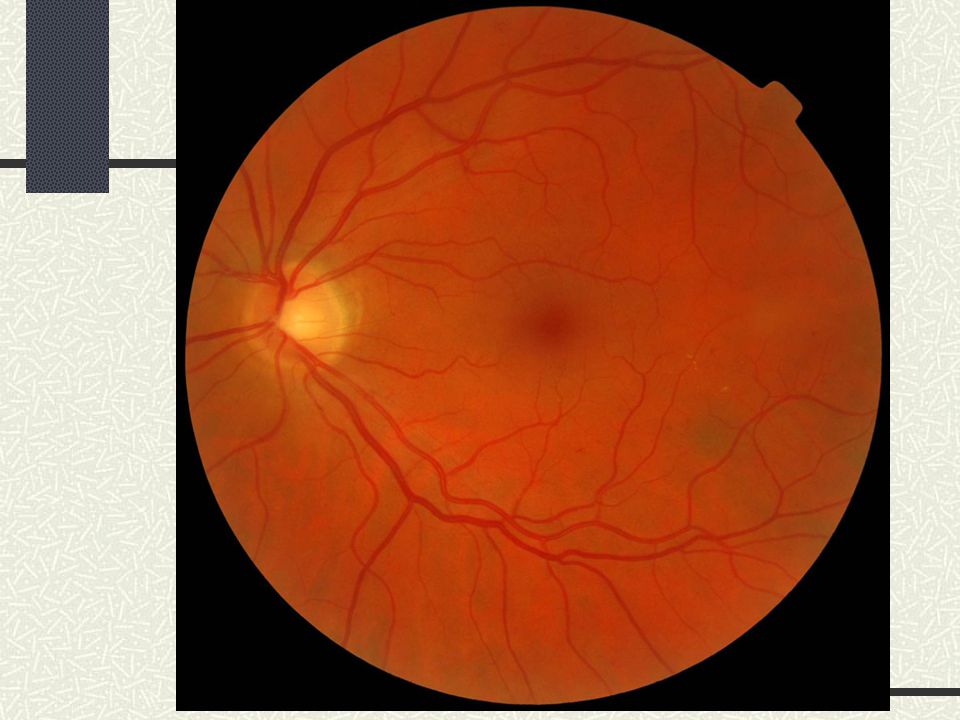
Grading IRMA Only IRMA that are definitely seen should be referred Once an IRMA is found, one should always return to the colour image. IRMA is considered present if the IRMA can still be seen on the colour image as well as on the red free. If an IRMA can only be seen on a red free image and not on the colour image a referral should not be made (return to annual screening).
..")
36
Localised patch of IRMA If there is a localised patch of possible IRMA in one area of the retina with very little other signs of diabetic retinopathy, one needs to consider whether a small branch vein occlusion may have occurred in this area in the past and that these might be small collaterals. If it is judged that small collaterals are present from an old small vein occlusion instead of IRMA, this would not warrant a referral.

37
R3 Proliferative Grading Criteria R3ProliferativeR3a (Active Proliferative Retinopathy) All newly occurring R3 patients with: new vessels on disc (NVD) new vessels elsewhere (NVE) pre-retinal or vitreous haemorrhage pre-retinal fibrosis tractional retinal detachment R3s (Stable post treatment) Evidence of Peripheral Retinal Laser Treatment AND Stable retina from photograph taken at or shortly after discharge from the Hospital Eye service (HES)
 All newly occurring R3 patients with: new vessels on disc (NVD) new vessels elsewhere (NVE) pre-retinal or vitreous haemorrhage pre-retinal fibrosis tractional retinal detachment R3s (Stable post treatment) Evidence of Peripheral Retinal Laser Treatment AND Stable retina from photograph taken at or shortly after discharge from the Hospital Eye service (HES)")
38
R3 will be split into R3a (Active Proliferative Retinopathy) and R3s (Stable Treated Proliferative Retinopathy) R3 (Proliferative Diabetic Retinopathy)
 and R3s (Stable Treated Proliferative Retinopathy) R3 (Proliferative Diabetic Retinopathy)")
39
R3s (Proliferative Diabetic Retinopathy The Definition of R3s (Stable) will be Evidence of Peripheral Retinal Laser Treatment AND Stable retina from photograph taken at or shortly after discharge from the HES
 will be Evidence of Peripheral Retinal Laser Treatment AND Stable retina from photograph taken at or shortly after discharge from the HES")
40
Guidance to the discharging ophthalmologist must make it clear that the English NHS Diabetic Eye Screening Programme only operates an annual screening programme and that they should only discharge patients who they assess are at sufficiently low risk to receive 12 monthly photographic screening. Assuming that the screening programme has an OPDR pathway it is recommended that stable treated retinopathy is kept in the OPDR pathway. R3s

41
On discharge, the hospital must either place a discharge set of images on the Screening Service software, supply a set of images electronically for the service to import or arrange for a set of discharge images to be taken by the Screening Service within 3 months. R3s

42
Maculopathy Grading Criteria M0No maculopathy absence of any M1 features M1Maculopathyexudate within 1 disc diameter (DD) of the centre of the fovea M1 - list of features as now - but individual features are not mutually exclusive group of exudates within the macula retinal thickening within 1DD of the centre of the fovea (if stereo available) any microaneurysm or haemorrhage within 1DD of the centre of the fovea only if associated with a best VA of 6/12 (if no stereo)
 of the centre of the fovea M1 - list of features as now - but individual features are not mutually exclusive group of exudates within the macula retinal thickening within 1DD of the centre of the fovea (if stereo available) any microaneurysm or haemorrhage within 1DD of the centre of the fovea only if associated with a best VA of 6/12 (if no stereo)")
43
Revised definition of a Group of Exudates A group of exudates is an area of exudates that is greater than or equal to half the disc area and this area (of greater than or equal half the disc area) is all within the macular area
 is all within the macular area")
45
Referable

49
Not Referable

53
Wet AMD Any images with signs of wet AMD should be referred via the local wet AMD service MREH – MARRC clinic SHH – Urgent ref to SHH – referral co-ordinator

54
Photocoagulation P No evidence of previous photocoagulation No grade is assigned Pfocal/grid to macula or peripheral scatter Only assigned if laser scars are identified UUnclassifiable UAn image set that is inadequate for grading

55
The main change will be that there will no longer be a ‘Good’ category, just ‘Adequate’ and ‘Inadequate’. The concept of ‘jig sawing’ is introduced, which is where a series of images can be combined to provide retinal views of the same areas as adequate macular and nasal images. Revision to Classification of Image Quality

56
Adequate Image Quality Macular image centre of fovea >2DD from edge of image & vessels visible within 1DD of centre of fovea and Disc image complete optic disc >2DD from edge of image & fine vessels visible on surface of disc

57
Inadequate Image Quality Inadequate Image Quality – failure to meet definition of adequate above If sight threatening retinopathy (STDR) is present on any image, the eye should be graded as adequate and patient referred to HES. Absence of a macula or disc / nasal image for the eye means the fields are inadequate for grading except if criteria in point 1 is fulfilled. if fine vessels are visible within 1DD of centre of fovea on any image available and fine vessels are visible on the surface of disc on any image available, the eye can be graded for R and M level. This could be by ‘jig sawing’ a series of images so that an adequate view is obtained of critical areas.

58
Implementation Date not yet set – software modifications TAT test sets – likely to change in October 2012

59
Acknowledgement Peter Scanlon Programme Director, NHS Diabetic Eye Screening Programme Ophthalmologist, Gloucestershire and Oxford Eye Unit

60
Thanks for listening! Any Questions?

Similar presentations

























 Waxman MD PhD>")



 Giovanni Caboto Club October 3, 2012>")












