Download presentation
Presentation is loading. Please wait.

1
Abnormal Psychology Oltmanns and Emery Chapter Thirteen Schizophrenic Disorders presented by: Mani Rafiee

2
Copyright © Prentice Hall 2007
Chapter Outline Symptoms Diagnosis Frequency Causes Treatment Copyright © Prentice Hall 2007

3
Overview The most common symptoms of schizophrenia include changes in the way a person thinks & feels No single symptom or specific set of symptoms. combinations of psychotic symptoms both the patients and their families.

4
Overview The onset of schizophrenia typically occurs during adolescence or early adulthood. ages of 15 and 35. three phases of variable and unpredictable duration: prodromal, active, and residual. Prodromal signs and symptoms are similar to those associated with schizotypal personality disorder. The residual phase follows the active phase similar in many respects to those seen during the prodromal phase.

5
Copyright © Prentice Hall 2007
Symptoms The symptoms of schizophrenia can be divided into three dimensions: positive symptoms, negative symptoms, and disorganization. Positive symptoms, also called psychotic symptoms, include hallucinations and delusions. In contrast, negative symptoms include characteristics such as lack of initiative, social withdrawal, and deficits in emotional responding. Copyright © Prentice Hall 2007

6
Copyright © Prentice Hall 2007
Symptoms Some additional symptoms of schizophrenia, such as incoherent or disorganized speech, do not fit easily into either the positive or negative types. Verbal communication problems and bizarre behavior represent this third dimension, which is sometimes called disorganization. Copyright © Prentice Hall 2007

7
Symptoms Hallucinations are sensory experiences that are not caused by actual external stimuli. those experienced by schizophrenic patients are most often auditory. delusions, or idiosyncratic beliefs that are rigidly held in spite of their preposterous nature. Common delusions include the belief that thoughts are being inserted into the patient’s head, that other people are reading the patient’s thoughts, or that the patient is being controlled by mysterious, external forces.

8
Symptoms Many delusions focus on grandiose or paranoid content.
In actual clinical practice, delusions are complex and difficult to define. Their content is sometimes bizarre and confusing.

9
Copyright © Prentice Hall 2007
Symptoms Negative Symptoms Blunted affect, or affective flattening, involves a flattening or restriction of the person’s nonverbal display of emotional responses. Another type of emotional deficit is called anhedonia, which refers to the inability to experience pleasure. Many people with schizophrenia become socially withdrawn. Copyright © Prentice Hall 2007

10
Symptoms Negative Symptoms (continued) poverty of speech, patients show remarkable reductions in the amount of speech. In another form, referred to as thought blocking, the patient’s train of speech is interrupted before a thought or idea has been completed.

11
Copyright © Prentice Hall 2007
Symptoms Disorganization Some symptoms of schizophrenia do not fit easily into either the positive or negative type. Thinking disturbances and bizarre behavior represent a third symptom dimension, which is sometimes called disorganization. One important set of schizophrenic symptoms, known as disorganized speech, involves the tendency of some patients to say things that don’t make sense. Copyright © Prentice Hall 2007

12
Copyright © Prentice Hall 2007
Symptoms Disorganization (continued) Schizophrenic patients may exhibit various forms of unusual motor behavior. Catatonia most often refers to immobility and marked muscular rigidity, but it can also refer to excitement and overactivity. Catatonic posturing is often associated with a stuporous state, or generally reduced responsiveness. Copyright © Prentice Hall 2007
 Schizophrenic patients may exhibit various forms of unusual motor behavior. Catatonia most often refers to immobility and marked muscular rigidity, but it can also refer to excitement and overactivity. Catatonic posturing is often associated with a stuporous state, or generally reduced responsiveness. Copyright © Prentice Hall")
13
Symptoms Disorganization (continued)
Another kind of bizarre behavior involves affective responses that are obviously inconsistent with the person’s situation. The most remarkable features of inappropriate affect are incongruity and lack of adaptability in emotional expression.

14
Diagnosis Brief Historical Perspective
Kraepelin’s term dementia praecox was, Bleuler suggested a new name for the disorder—schizophrenia. This term referred to the splitting of mental associations, which Bleuler believed to be the fundamental disturbance in schizophrenia. Bleuler's four A's: (disturbance of) affect, association, ambivalence and autism
 affect, association, ambivalence and autism.")
15
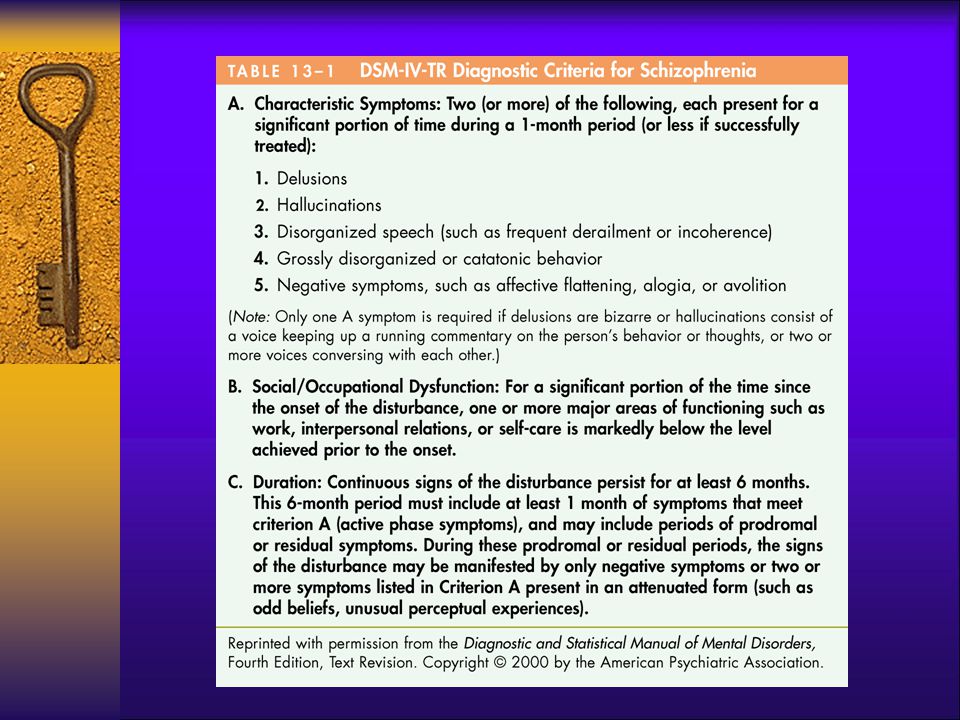
Diagnosis DSM-IV-TR DSM-IV-TR lists several specific criteria for schizophrenia. The first requirement (Criterion A) is that the patient must exhibit two (or more) active symptoms for at least 1 month. The DSM-IV-TR definition also takes into account social and occupational functioning as well as the duration of the disorder (Criteria B and C).
 is that the patient must exhibit two (or more) active symptoms for at least 1 month. The DSM-IV-TR definition also takes into account social and occupational functioning as well as the duration of the disorder (Criteria B and C).")
17
Diagnosis Subtypes DSM-IV-TR recognizes five subtypes of schizophrenia. The catatonic type is characterized by symptoms of motor immobility (including rigidity and posturing) or excessive and purposeless motor activity. The disorganized type of schizophrenia is characterized by disorganized speech, disorganized behavior, and flat or inappropriate affect.
 or excessive and purposeless motor activity. The disorganized type of schizophrenia is characterized by disorganized speech, disorganized behavior, and flat or inappropriate affect.")
18
Diagnosis Subtypes The most prominent symptoms in the paranoid type are systematic delusions with persecutory or grandiose content. The undifferentiated type of schizophrenia includes schizophrenic patients who display prominent psychotic symptoms and either meet the criteria for several subtypes or otherwise do not meet the criteria for the catatonic, disorganized, or paranoid types.

19
Diagnosis Subtypes The residual type includes patients who no longer meet the criteria for active phase symptoms but nevertheless demonstrate continued signs of negative symptoms or attenuated forms of delusions, hallucinations, or disorganized speech. They are in “partial remission.”

20
Diagnosis Related Psychotic Disorders
Schizoaffective disorder is defined by an episode in which the symptoms of schizophrenia partially overlap with a major depressive episode or a manic episode. People with delusional disorder do not meet the full symptomatic criteria for schizophrenia, but they are preoccupied for at least 1 month with delusions that are not bizarre.

21
Copyright © Prentice Hall 2007
Diagnosis Related Psychotic Disorders (continued) Brief psychotic disorder is a category that includes those people who exhibit psychotic symptoms—delusions, hallucinations, disorganized speech, or grossly disorganized or catatonic behavior—for at least 1 day but no more than 1 month. Copyright © Prentice Hall 2007
 Brief psychotic disorder is a category that includes those people who exhibit psychotic symptoms—delusions, hallucinations, disorganized speech, or grossly disorganized or catatonic behavior—for at least 1 day but no more than 1 month. Copyright © Prentice Hall")
22
Schizophrenia Spectrum & other psychotic disorders in DSM 5
The DSM-IV subtypes of schizophrenia (i.e., paranoid, disorganized, catatonic, undifferentiated, and residual types) are eliminated Main change of schizoaffective disorder is the requirement that a major mood episode be present for a majority of the disorder’s total duration after Criterion A has been met
 are eliminated. Main change of schizoaffective disorder is the requirement that a major mood episode be present for a majority of the disorder’s total duration after Criterion A has been met.")
23
Schizophrenia Spectrum & other psychotic disorders in DSM 5
Criterion A for delusional disorder no longer has the requirement that the delusions must be nonbizarre. DSM-5 no longer separates delusional disorder from shared delusional disorder Catatonia: The criteria for catatonia is now uniform for all contexts

24
Frequency Most studies in Europe and the United States have reported lifetime morbid risk figures of approximately 1 percent.

25
Frequency Gender Differences
Most epidemiological studies have reported that across the life span men and women are equally likely to be affected by schizophrenia. males younger by about 4 or 5 years than the average age at which schizophrenic women first experience problems. Male patients are more likely than female patients to exhibit negative symptoms.

26
Frequency Cross-Cultural Comparisons
Schizophrenia has been observed in virtually every culture that has been subjected to careful scrutiny.

27
Causes Biological Factors
Research evidence points clearly toward some type of genetic influence in the transmission of schizophrenia. The family history data are consistent with the hypothesis that the transmission of schizophrenia is influenced by genetic factors.

28
Causes Biological Factors (continued)
Linkage analysis has not been able to identify a specific gene for schizophrenia, but it has implicated regions on a small number of chromosomes that may contribute to the etiology of the disorder. For example, reports of positive linkage on regions of chromosomes 6, 8, 13, and 22 have been verified by more than one laboratory.

29
Causes Pregnancy and Birth Complications
Viral Infections (winter month's birth) Neuropathology decrease in total volume of brain tissue structural changes limbic system enlarged lateral ventricles frontal cortex
 Neuropathology. decrease in total volume of brain tissue. structural changes limbic system. enlarged lateral ventricles. frontal cortex.")
30
Causes Neurochemistry
Scientists have proposed various neurochemical theories to account for the etiology of schizophrenia. The most influential theory, known as the dopamine hypothesis, focuses on the function of specific dopamine pathways in the limbic area of the brain.

31
Causes Social Factors The evidence supporting an inverse relationship between social class and schizophrenia is substantial. Adverse social and economic circumstances may increase the probability that persons who are genetically predisposed to the disorder will develop its clinical symptoms.

32
Causes Psychological Factors
The family environment does have a significant impact on the course (as opposed to the etiology) of schizophrenia. Families is high in expressed emotion. Integration and Multiple Pathways
 of schizophrenia. Families is high in expressed emotion. Integration and Multiple Pathways.")
33
Copyright © Prentice Hall 2007
Treatment Antipsychotic Medication Antipsychotic drugs reduce the severity of, and sometimes eliminate, psychotic symptoms. Classical antipsychotics are also known as neuroleptic drugs because they also induce side effects that resemble the motor symptoms of Parkinson’s disease. Copyright © Prentice Hall 2007

34
Treatment Antipsychotic Medication (continued)
Atypical antipsychotics are less likely than the classical antipsychotics to produce unpleasant motor side effects. Atypical antipsychotics also produce side effects, such as weight gain and obesity. All antipsychotic medications—both traditional and atypical forms—act by blocking dopamine receptors in the cortical and limbic areas of the brain.

35
Treatment Psychosocial Treatment
Family treatment programs attempt to improve the coping skills of family members, recognizing the burdens that people often endure while caring for a family member with a chronic mental disorder. There are several different approaches to this type of family intervention. Most include an educational component that is designed to help family members understand and accept the nature of the disorder.

36
Treatment Various forms of cognitive therapy have been used to treat schizophrenia. Some patients are chronically disturbed and require long-term institutional treatment. Social learning programs, sometimes called token economies, can be useful for these patients.

Similar presentations





 Praecox (Early,>")

>")




 2.hallucinations 3.Disorganized.>")





 between affect (feelings) and cognition (thoughts) Early physicians,>")
