Download presentation
Presentation is loading. Please wait.

1
Tom A. Elasy, M.D., M.P.H. Vanderbilt University February, 2012

3
Scalability ◦ People ◦ Intervention ◦ Context Sustainability ◦ Theories ◦ Interventions: induction vs. maintenance Monitoring Goal setting

4
Yarnall KS, et al. Am J Public Health 2003;93:635-641

6
A line of inquiry ◦ “Relapse” in glucose control ◦ Causes of Relapse ◦ A Taxonomy of Interventions ◦ Results of a RCT to prevent Relapse Implications

7
64 y.o. woman presents to establish primary care – referred by NP in endocrine clinic. “I’m not doin’ so good. My life has been chaotic lately.” PMHx: DM dx’d 1992 – started insulin 2yrs prior to presentation HTN Depression –pharmacotherapy for 3yrs OA – primarily of Left Knee

8
Medication: Lisinopril, HCTZ, Metformin, Glipizide, Basal/Bolus(fixed) insulin, ASA, Citalopram, Simvastatin, occasional Tylenol #3 SHx: Married – lives with husband. 3 grown children. AA at Vanderbilt for 1 yr. No substance abuse. ROS: One yeast infection in last 6 months. Weight stable. No hypoglycemia.

11
Assessment: “Her diet has been erratic and she has missed several doses of her insulin. She’s lost her motivation.” Plan: “I emphasized the importance of keeping her glucose under good control and encouraged her to resume her previous successful management. I scheduled her to come back in 4 weeks.”

12
A Line of Inquiry ◦ “Relapse” in glucose control ◦ Causes of Relapse ◦ A Taxonomy of Interventions ◦ Results of a RCT to prevent Relapse Implications

14
Step 1 Objective: Quantify the occurrence of glycemic deterioration AFTER achieving acceptable glucose control had been achieved. Hypothesis: In individuals who have achieved adequate glucose control, deterioration (“Relapse”) will occur at a rate greater than expected based on previous longitudinal studies.
 will occur at a rate greater than expected based on previous longitudinal studies..")
15
Retrospective Cohort: N=396 Inclusion: ◦ Initial A1c > 8% and had improved by at least 1% AND final A1c less than 8% ◦ Received f/u primary care at Vanderbilt Primary Outcome (time to event) ◦ A1c > 1% of nadir and exceeds 8%
 ◦ A1c > 1% of nadir and exceeds 8%")
16
Natural History of Relapse (n=396) Probability without Relapse 0.0 0.2 0.4 0.6 0.8 1.0 0 61218243036 Months after Nadir
 Probability without Relapse Months after Nadir")
17
0.0 0.2 0.4 0.6 0.8 1.0 061218243036 Relapse: Insulin Start Months after Nadir Probability of Relapse Free Insulin Started No Yes Median time to relapse: 34.1 months 23.8 months p=0.045 (Log Rank test)
")
18
Cumulative incidence of relapse at 1yr: 25% Initiation of insulin therapy is the only independent predictor identified: HR 1.96 50% relapse by 30 months Median time to relapse in those who relapsed is 9 months.

19
A Line of Inquiry ◦ “Relapse” in glucose control ◦ Causes of Relapse ◦ A Taxonomy of Interventions ◦ Results of a RCT to prevent Relapse Implications for Primary Care

20
Movere: To move

21
Intent Ability/Skill Norms Environmental constraints Anticipated outcomes Self-standards Emotion Self-efficacy Fishbein 1991

22
Step 2 Objective: Determine the dispositional and situational variables that contribute to deterioration of glycemic control Hypothesis : Individuals who successfully complete a diabetes improvement program will be more likely to experience glycemic deterioration if exposed to a life stressor compared to those who are not exposed to a life stressor.

23
Cross-Sectional Structured Interviews ◦ ~ 90 minutes each Population: N= 89 (convenience sample) ◦ 42 who had relapsed and 47 who had not Timing: within 3 months of relapse Exposure (new life stressor) definition: any change in financial, relational, health or new responsibility
 ◦ 42 who had relapsed and 47 who had not Timing: within 3 months of relapse Exposure (new life stressor) definition: any change in financial, relational, health or new responsibility")
24
Relapse (n=42)Stable (n=47) Age4952 BMI31.332.4 Insulin Use*63%49% Duration of DM 7.26.6 Female58%57% African American* 26%17% High School88%85%
Stable (n=47) Age4952 BMI Insulin Use*63%49% Duration of DM Female58%57% African American* 26%17% High School88%85%")
25
Relapse (n=42)Stable (n=47) Financial10%11% Relational19%15% Health17%11% New Responsibilities* 45%23% Total*95%60%
Stable (n=47) Financial10%11% Relational19%15% Health17%11% New Responsibilities* 45%23% Total*95%60%")
26
Life stressors, high in both groups, appear to be higher (OR =1.5) in individuals who experience glycemic deterioration New responsibilities (or competing priorities) appear to be driving the difference
 in individuals who experience glycemic deterioration New responsibilities (or competing priorities) appear to be driving the difference")
27
A Line of Inquiry ◦ “Relapse” in glucose control ◦ Causes of Relapse ◦ A Taxonomy of Interventions ◦ Results of a RCT to prevent Relapse Implications

30
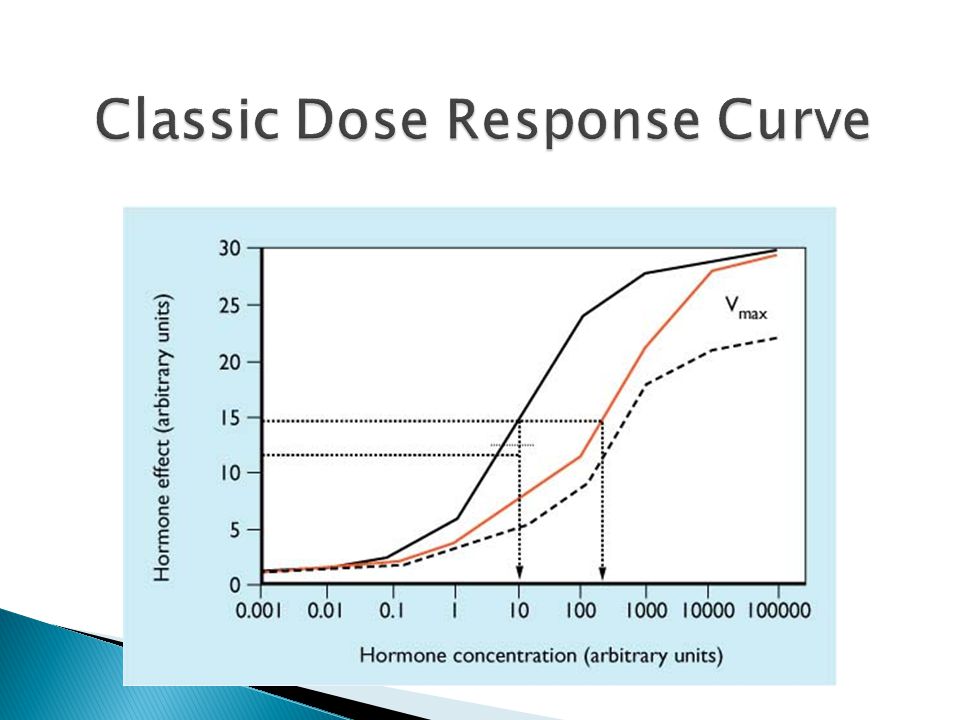
Step 3 Objective: Identify the domains of variation within DM educational interventions. Exploratory Hypothesis: High intensity (“dose”) of DM educational interventions will be predictive of better glucose control.
 of DM educational interventions will be predictive of better glucose control..")
31
Design: ◦ Literature review and expert input “In what meaningful ways can DM educational interventions vary?” ◦ Standard meta-analytical and meta-regression techinique Population: RCTs with glycemic control as an outcome (1990-2000)
")
32
Setting: One-on-one, group, family Delivery: Face-to-face, telecommunication, written material Teaching method: didactic, goal-setting, cognitive reframing, situational problem solving Content: diet, exercise, medication adherence, knowledge Provider: Nurse, RD, psychologist, exercise specialist Intensity of the intervention: # of episodes, duration of episodes, duration of intervention

35
Six domains characterize meaningful variation in DM educational interventions Educational interventions have a modest net effect (0.32%) on HbA1c No clear effect of educational “dose” on glycemic variation
 on HbA1c No clear effect of educational dose on glycemic variation")
36
A Line of Inquiry ◦ “Relapse” in glucose control ◦ Causes of Relapse ◦ A Taxonomy of Interventions ◦ Results of a RCT to prevent Relapse Implications

37
Step 4 Objective: To assess the relative effectiveness of 3 maintenance treatments, varying in intensity, for preventing glycemic relapse after acceptable glycemic control is achieved Hypothesis: A higher frequency of intervention will yield, in a dose-dependant fashion, a lower relapse rate

38
60% of primary care patients are not at A1C goal Intensive diabetes improvement programs improve glycemic control Many patients fail to sustain glycemic control after 1-2 years (i.e. relapse) ◦ Biological ◦ Behavioral
 ◦ Biological ◦ Behavioral.")
40
Adapted from UK Prospective Diabetes Study (UKPDS) Group. Lancet. 1998;352:837- 853. Cross-sectional Median Values (7.0% vs 7.9%) 9 8 7 6 6.2% upper limit of normal range ADA target ADA action suggested 0 0369 Years From Randomization 1218 Conventional Intensive 7.4% 6.6% 8.4% 7.5% 8.7% 8.1% Median HbA 1c (%) 6-3
 % upper limit of normal range ADA target ADA action suggested Years From Randomization 1218 Conventional Intensive 7.4% 6.6% 8.4% 7.5% 8.7% 8.1% Median HbA 1c (%) 6-3.")
42
Relapse defined as an A1C≥1% Approximately 45% of patients relapse within 1 year 76% relapse by 3 years Median time to relapse was 15.2 months

43
Routine contact with providers Obesity, Perri et al, 1984 Behavioral maintenance package ◦ Identification of situations that are high risk for slips ◦ Training in problem solving to deal with high-risk situations ◦ Actual practice in coping with potential slips or high-risk situations ◦ Development of cognitive coping techniques for negotiating lapses Alcoholism, Marlatt et al, 1996 Systematic but brief assessment & encouragement Smoking, Baer et al, 1991

44
Un-blinded randomized controlled trial ◦ Randomization: permuted block scheme 3 arms ◦ Least intensive – usual care, control ◦ Moderate intensity – Quarterly telephonic contact ◦ High intensity – Monthly telephonic contact

45
Patients with type 2 diabetes who recently completed a diabetes improvement program and achieved glycemic control (A1C decrease of ≥ 1%) ◦ DIP is a 12 week intensive outpatient treatment consisting of education from a CDE NP and RD and medication titration
 ◦ DIP is a 12 week intensive outpatient treatment consisting of education from a CDE NP and RD and medication titration")
46
Phone contact by a nurse practitioner with a referral to a dietitian if nutrition self-care is perturbed Identify and problem-solve issues arising in self-care behaviors, including diet, physical activity, self-monitoring of blood glucose and medication adherence

47
If no problem in self-care behaviors identified ◦ Anticipatory planning ◦ Positive reinforcement ◦ Goal-setting

48
If problem in self-care behavior identified ◦ Standard problem solving paradigm ◦ If cannot identify source of problem Goal setting was employed Compensation with another self-care behavior

49
Nurse practitioners were to adhere to a set of intervention protocols and guidelines Intervention fidelity analysis performed to determine adherence to the protocol

50
Glycemic relapse ◦ Defined as an increase in A1C of ≥ 1% from baseline ◦ Proportion of relapse at each time point ◦ Time to event

51
28 of the participants also had maximally stimulated c-peptide measured throughout the study Determine the extent of relapse due to decrease in -cell function

52
Characteristic Control Group (n=54) Quarterly contact (n=55) Monthly contact (n=55) Age, y ** 56.2 ± 1055.7 ± 1153.5 ± 11 Female (%)433851 African American (%)132922 ≥ High School (%)878991 Duration of diabetes, y * 5.5 (0.7,10)4.0 (0.5,10) Insulin use (%)594558 Units of insulin/kg*39 (24, 79)59 (32,100)61 (25, 93) BMI, kg/m 2** 34 ± 733 ± 635 ± 7 A1C, % ** 6.7 ± 0.76.6 ± 0.76.8 ± 0.6 CES-D * 9 (4,18)10 (4,17)7 (4,14) No differences between study arms for any characteristic * Reported as Median (IQR); ** Reported as Mean ± SD
 Quarterly contact (n=55) Monthly contact (n=55) Age, y ** 56.2 ± ± ± 11 Female (%) African American (%) ≥ High School (%) Duration of diabetes, y * 5.5 (0.7,10)4.0 (0.5,10) Insulin use (%) Units of insulin/kg*39 (24, 79)59 (32,100)61 (25, 93) BMI, kg/m 2** 34 ± 733 ± 635 ± 7 A1C, % ** 6.7 ± ± ± 0.6 CES-D * 9 (4,18)10 (4,17)7 (4,14) No differences between study arms for any characteristic * Reported as Median (IQR); ** Reported as Mean ± SD")
53
Adherence to Relapse interview protocol quite high ◦ 29 calls from 2 NPs analyzed by 2 coders ◦ All elements of protocol present at least 80% of the time 96% of phone calls were completed Attrition rate 9.2%

54
3 months8% 6 months14% 12 months16% 24 months25% Overall (at any point in study)45%
45%")
55
ControlsMonthlyQuarterly

56
ControlsMonthlyQuarterly 0.00 0.10 0.20 0.30 0.40 0.50 Probability of relapse 0.25 0.35 0.45 0.55 0.65 0.75 0.85 0.95 Relapse Free 06121824 Time to first relapse (months)
")
57
Maximally stimulated C-peptide (ng/mL) * Baseline7.2 (IQR 5.2, 8.4) 24 months7.0 (IQR 5.4, 7.9) * p = 0.72 by signed-rank test (non-parametric paired data)
 * Baseline7.2 (IQR 5.2, 8.4) 24 months7.0 (IQR 5.4, 7.9) * p = 0.72 by signed-rank test (non-parametric paired data)")
58
Relapse at 24 months (n=12) No relapse at 24 months (n=9) Delta C-peptide (ng/mL)* 0.18 (-0.7, 2.2)0.24 (-0.7, 1.2) * median (IQR), p = 0.94 by Wilcoxon rank sum
 No relapse at 24 months (n=9) Delta C-peptide (ng/mL)* 0.18 (-0.7, 2.2)0.24 (-0.7, 1.2) * median (IQR), p = 0.94 by Wilcoxon rank sum")
59
Quarterly:ControlMonthly:Control Overall0.96 (0.49 – 1.9)1.01 (0.52 – 1.9) Female Male 0.4 (0.13 – 1.2) 1.69 (0.58 – 4.9) 1.1 (0.4 – 2.7) 0.73 (0.26 – 2.1) BMI < 35 kg/m 2 BMI ≥ 35 kg/m 2 1.8 (0.71 – 4.7) 0.52 (0.18 – 1.5) 2.4 (1.01 – 5.7) 0.42 (0.17 – 1.0) Black Non-Black 1.1 (0.0024 – 523) 1.01 (0.47 – 2.2) 1.6 (0.0037 – 716) 0.94 (0.46 – 1.9)
1.01 (0.52 – 1.9) Female Male 0.4 (0.13 – 1.2) 1.69 (0.58 – 4.9) 1.1 (0.4 – 2.7) 0.73 (0.26 – 2.1) BMI < 35 kg/m 2 BMI ≥ 35 kg/m (0.71 – 4.7) 0.52 (0.18 – 1.5) 2.4 (1.01 – 5.7) 0.42 (0.17 – 1.0) Black Non-Black 1.1 ( – 523) 1.01 (0.47 – 2.2) 1.6 ( – 716) 0.94 (0.46 – 1.9)")
60
Quarterly:ControlMonthly:Control Overall0.96 (0.49 – 1.9)1.01 (0.52 – 1.9) Female Male 0.4 (0.13 – 1.2) 1.69 (0.58 – 4.9) 1.1 (0.4 – 2.7) 0.73 (0.26 – 2.1) BMI < 35 kg/m 2 BMI ≥ 35 kg/m 2 1.8 (0.71 – 4.7) 0.52 (0.18 – 1.5) 2.4 (1.01 – 5.7) 0.42 (0.17 – 1.0) Black Non-Black 1.1 (0.0024 – 523) 1.01 (0.47 – 2.2) 1.6 (0.0037 – 716) 0.94 (0.46 – 1.9)
1.01 (0.52 – 1.9) Female Male 0.4 (0.13 – 1.2) 1.69 (0.58 – 4.9) 1.1 (0.4 – 2.7) 0.73 (0.26 – 2.1) BMI < 35 kg/m 2 BMI ≥ 35 kg/m (0.71 – 4.7) 0.52 (0.18 – 1.5) 2.4 (1.01 – 5.7) 0.42 (0.17 – 1.0) Black Non-Black 1.1 ( – 523) 1.01 (0.47 – 2.2) 1.6 ( – 716) 0.94 (0.46 – 1.9)")
61
Two maintenance strategies employing a telephonic behavioral maintenance strategy did not prevent glycemic relapse more than usual care Certain sub-groups may have benefited from the intervention ◦ BMI ≥ 35 kg/m 2 – both intervention arms ◦ Females – quarterly contact only

62
Lower relapse rate than anticipated from observational studies Intervention ◦ Based on successful maintenance strategies for other diseases; other programs may prove more effective ◦ No protocol for what to do when someone relapsed Self-care behavior assessment not sufficient to detect early deterioration

63
Disease management companies use telephonic contact or newsletters in the maintenance phase of disease care This kind of intervention is understudied – further work is needed to understand maintenance care and who benefits from these interventions

64
Kong Chen, PhD Renee Stiles, PhD Ayumi Shintani, PhD Ken Wallston, PhD Anne Brown, ANP Kathleen Wolff, ANP Al Powers, MD Robert Dittus, MD Alan Graber, MD Jim Pichert, PhD Ted Speroff, PhD Shelley Ellis, MD Francine Johnson, MD Jeffrey Bontrager, MD Carolyn Nyuang, MD Michael Blaha, MD Stephanie Michon, RD LauraShackleford, FNP David Schlundt, PhD Daryl Granner, MD NIDDK

Similar presentations

























 Grants Chapter 6.>")

