Download presentation
Presentation is loading. Please wait.

1
Adjuvant therapy for resected colon cancer
Dr.vahedian ardakani Medical oncologist 1390/10/1

3
Adjuvant therapy Following potentially curative resection of colon cancer, the goal of adjuvant chemotherapy is to eradicate micrometastases, thereby reducing the likelihood of disease recurrence and increasing the cure rate.

4
Adjuvant therapy The benefits of adjuvant chemotherapy have been most clearly demonstrated in stage III (node-positive) disease (an approximately 30 percent reduction in the risk of disease recurrence and a 22 to 32 percent reduction in mortality), whereas benefit is less certain for stage II disease.
 disease (an approximately 30 percent reduction in the risk of disease recurrence and a 22 to 32 percent reduction in mortality), whereas benefit is less certain for stage II disease.")
6
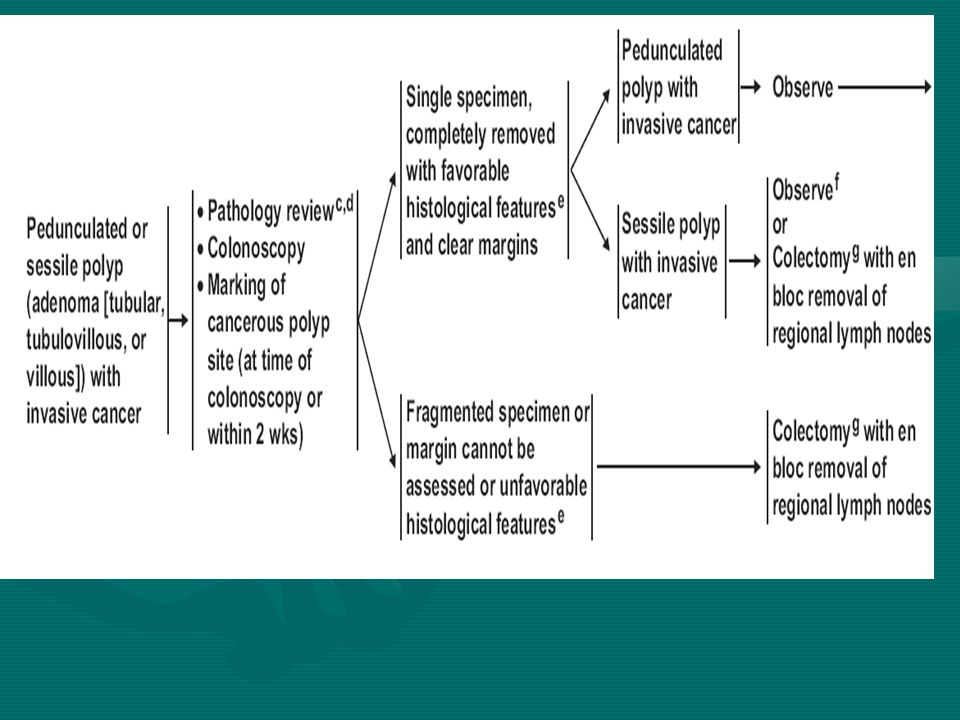
management of invasive cancer in a polyp
Endoscopic resection alone is a reasonable approach for favorable-risk early stage colon cancers arising in a polyp. Large polypoid lesions may require a segmental resection

7
management of invasive cancer in a polyp
radical resection if any of the following are present: Poorly differentiated histology Lymphovascular invasion Cancer at the resection or stalk margin Invasion into the muscularis propria of the bowel wall (T2 lesion) Invasive carcinoma arising in a sessile (flat) polyp with unfavorable features (eg, lower third submucosal penetration, lymphovascular invasion, poorly differentiated) Invasive carcinoma with incomplete polypectomy
 Invasive carcinoma arising in a sessile (flat) polyp with unfavorable features (eg, lower third submucosal penetration, lymphovascular invasion, poorly differentiated) Invasive carcinoma with incomplete polypectomy.")
9
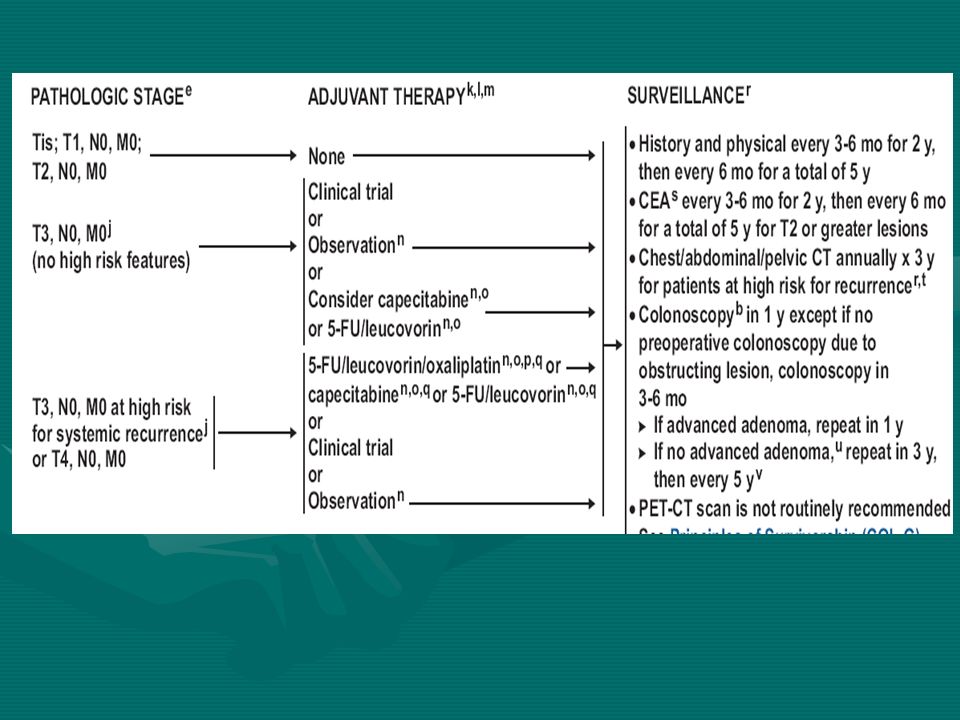
Stage I Colon Cancer Following a complete resection of a stage I lesion, no further adjuvant therapy is required. Patients managed in this way can expect a more than 95% 5-year survival.

10
Stage II , III Colon Cancer
The primary management of stage II and III colon cancer is surgical resection The role of adjuvant therapy is to eradicate that microscopic metastatic disease. Because current diagnostic techniques are unable to identify those patients with or without micrometastases, patients at sufficient risk of clinical recurrence are treated postoperatively

11
Stage II The optimal management of stage II colon cancer patients remains undefined. Although the role of adjuvant therapy in stage II colon cancer patients has not been firmly established, Using the Surveillance, Epidemiology, and End Results (SEER)-Medicare linked database, Schrag et al identified 3,151 patients aged 65 to 75 with resected stage II colon cancer and no adverse prognostic features Their review identified that 27% of patients received chemotherapy during the 3-month postoperative period. Younger age, white race, unfavorable tumor grade, and low comorbidity were associated with a greater likelihood of receiving treatment. The 5-year survival was 75% for untreated patients and 78% for those patients who received therapy in this nonrandomized comparison.
-Medicare linked database, Schrag et al identified 3,151 patients aged 65 to 75 with resected stage II colon cancer and no adverse prognostic features. Their review identified that 27% of patients received chemotherapy during the 3-month postoperative period. Younger age, white race, unfavorable tumor grade, and low comorbidity were associated with a greater likelihood of receiving treatment. The 5-year survival was 75% for untreated patients and 78% for those patients who received therapy in this nonrandomized comparison.")
12
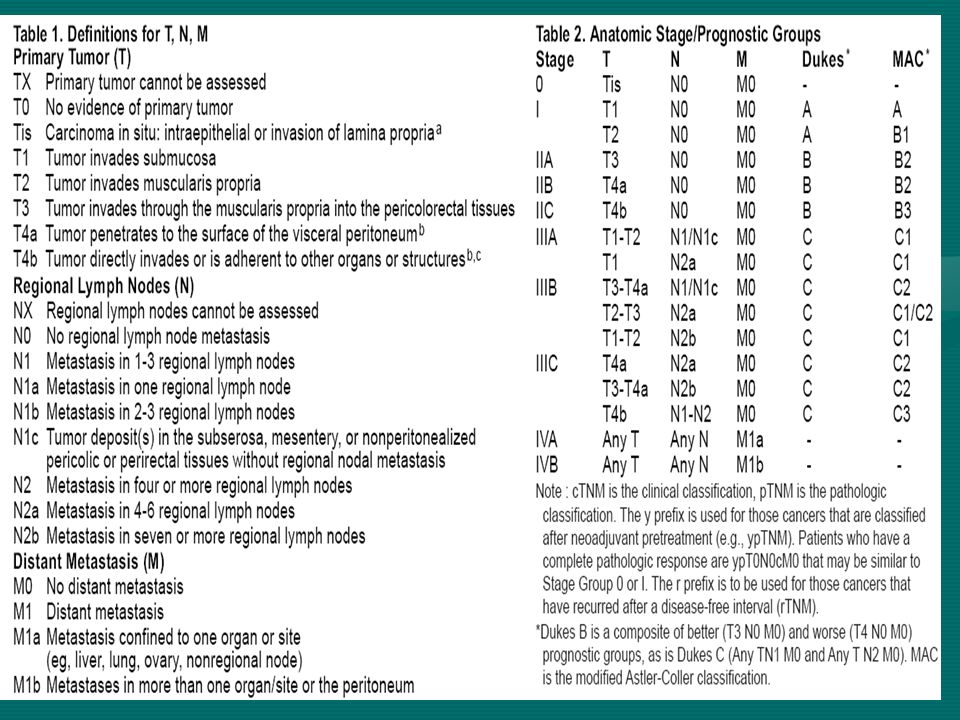
Stage II Several prognostic indicators have been identified that correlate with a higher risk for subsequent failure in stage II patients. These include : obstruction or perforation of the bowel wall as well as other less-established risk factors such as elevated preoperative CEA, poorly differentiated histology, or a high S-phase fraction, and tumors not demonstrating high levels of microsatellite instability, or tumors with an 18q deletion in colorectal tumors may correlate with a poor prognosis. 12

13
Total Number of Lymph Nodes
The CAP consensus statement suggests that a minimum of 12 to 15 lymph nodes should be examined in order to determine node negativity. Availability of fewer nodes should therefore be regarded as a relative high-risk factor in terms of prognosis and should be factored into decisions regarding adjuvant therapy.

14
the number of lymph nodes analyzed, presence of high-risk clinicopathologic features (fewer than 12 nodes in the surgical specimen; T4 or perforated/obstructed lesion poorly differentiated histology (including signet ring and mucinous); lymphovascular or perineural invasion), mismatch repair enzyme (MMR) status,
; lymphovascular or perineural invasion), mismatch repair enzyme (MMR) status,")
15
Stage II It appears that stage II patients with one or more of these risk factors have a poorer prognosis and a prognosis closer to patients with stage III disease. Whether adjuvant chemotherapy can provide similar benefits in these patients as it does in stage III patients currently remains a matter of conjecture. In the absence of definitive data, definitive recommendations cannot be made at this time. In fully informed high-risk stage II patients, it is reasonable to consider adjuvant treatment using stage III treatment regimens. COLON AND RECTUM 15

16
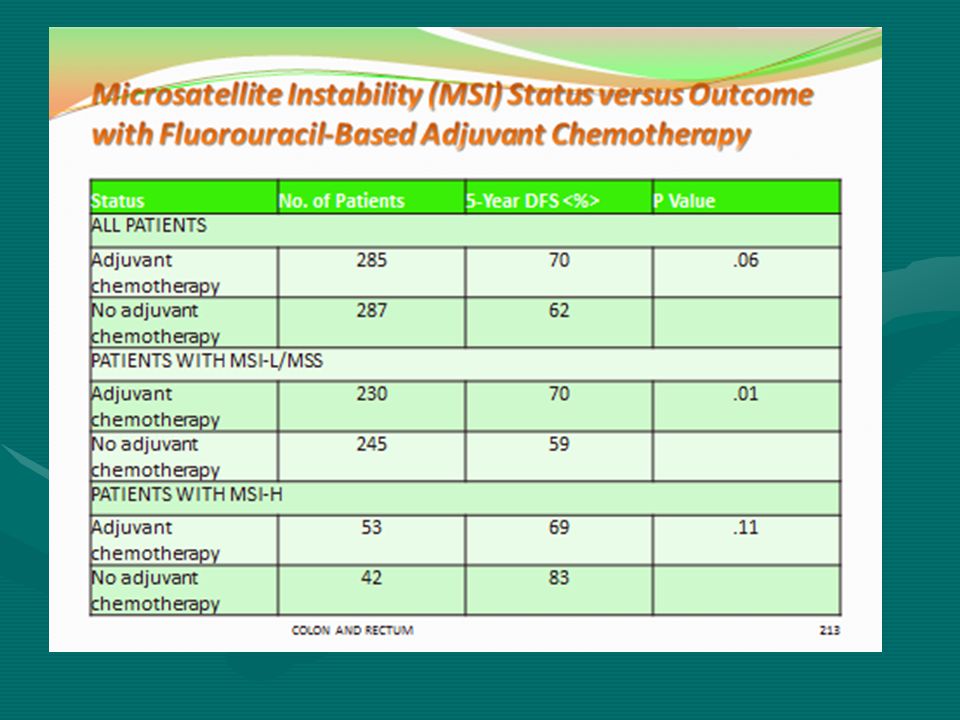
Patients without high-risk features who have MSI-H/dMMR tumors have a favorable prognosis and are not likely to benefit from adjuvant fluoropyrimidine-based therapy. We suggest observation alone for most of these patients

17
Chemotherapy was associated with improved outcome in both stage II and stage III patients with MSS or MSI-L, . In contrast, in patients with MSI-H tumors, treatment did not improve survival, and in fact was associated with a trend toward worse outcome for both stage II and stage III cancers

19
Allelic Loss of 18Q (DCC Gene Loss)
Allelic Status of 18q No. of Patients 5-Year Survival (%) P Value No loss 112 69 .005 Loss 109 50 COLON AND RECTUM
 P Value. No loss Loss COLON AND RECTUM.")
20
We suggest a fluoropyrimidine-based regimen leucovorin-modulated FU or capecitabine alone) rather than an oxaliplatin-based regimen for most patients with stage II disease who are average risk, We discuss the results of the MOSAIC trial and the potential toxicity of oxaliplatin in patients who have high-risk stage II disease, particularly with multiple risk factors For patients who have deficient mismatch repair (dMMR) tumors but other high risk features, the use of oxaliplatin should be considered more strongly given at the apparent lack of benefit from single agent fluoropyrimidines.
 tumors but other high risk features, the use of oxaliplatin should be considered more strongly given at the apparent lack of benefit from single agent fluoropyrimidines.")
21
Results of the MOSAIC Trial
LV5FU2 (n = 1,123) FOLFOX-4 (n = 1,123) Hazard Ratio (95% Confidence Interval) 3-year disease-free survival stage III patients (60% of total) 66% 72% .76 ( ) 3-year disease-free survival, stage II patients (40% of total) 84% 87% .82 ( ) Overall survival Not available - Grade 3-4 neutropenia 5% 41% Neutropenic fever 0% 1% Grade 3-4 diarrhea Grade 3-4 vomiting 7% 11% Neuropathy, any grade 92% Neuropathy, grade 3 12% Persistent neuropathy, grade 2-3, 1 year after treatment 21
 FOLFOX-4 (n = 1,123) Hazard Ratio (95% Confidence Interval) 3-year disease-free survival stage III patients (60% of total) 66% 72% .76 ( ) 3-year disease-free survival, stage II patients (40% of total) 84% 87% .82 ( ) Overall survival. Not available. - Grade 3-4 neutropenia. 5% 41% Neutropenic fever. 0% 1% Grade 3-4 diarrhea. Grade 3-4 vomiting. 7% 11% Neuropathy, any grade. 92% Neuropathy, grade 3. 12% Persistent neuropathy, grade 2-3, 1 year after treatment. 21.")
23
Stage III The benefits of adjuvant chemotherapy have been most clearly demonstrated in stage III (node-positive) disease (an approximately 30 percent reduction in the risk of disease recurrence and a 22 to 32 percent reduction in mortality), whereas benefit in stage II disease remains controversial
 disease (an approximately 30 percent reduction in the risk of disease recurrence and a 22 to 32 percent reduction in mortality), whereas benefit in stage II disease remains controversial.")
24
Stage III We recommend adjuvant systemic therapy after resection of stage III colon cancer If possible, chemotherapy should be initiated within six to eight weeks of surgery

25
We recommend a six month course of an oxaliplatin-based regimen rather than bolus 5-FU plus leucovorin (FU/LV) or capecitabine for patients who are likely to tolerate oxaliplatin
 or capecitabine for patients who are likely to tolerate oxaliplatin")
26
Stage III It is clear that in the absence of medical or psychiatric contraindications, patients with node-positive colon cancer should receive postoperative chemotherapy. At the very least, a 5-FU based regimen would appear to be appropriate, and approximately a half year of therapy would be supported by the majority of trials.

27
Stage III this time, the data for incorporation of oxaliplatin into the routine adjuvant treatment of colon cancer appear compelling, and the FOLFOX schedule is now the most widely used adjuvant therapy. Weekly irinotecan plus bolus 5-FU/leucovorin should not be used in the adjuvant setting, as randomized data have shown increased risk of early death and no long-term benefit. The available randomized data overall do not support the routine use of any irinotecan-based regimens in the adjuvant setting.

28
For patients with a contraindication to oxaliplatin eg, preexisting neuropathy), 5-FU/LV is an acceptable option, although outcomes may not be as favorable. An alternative is six months of oral capecitabine We recommend not using bevacizumab , cetuximab or an irinotecan-based regimen in the adjuvant setting.

30
Roswell park regimen -FU + LV 5-FU 500 mg/m2 iv bolus 1 h after the start of leucovorin Leucovorin 500 mg/m2 iv over 2 hrs Qw x 6 wks every 8 wks for 3-4 cycles

31
Mayo clinic regimen 5-FU + LV5-
FU mg/m2/d iv bolus d1-5 Leucovorin mg/m2/d iv bolus d1-5 Q4w x 6 cycles

32
Capecitabine Capecitabine (Xeloda) 1250 mg/m2 po bid x 14 days Q3w x 8 cycles
 1250 mg/m2 po bid x 14 days Q3w x 8 cycles")
33
FOLFOX4 Leucovorin 200 mg/m2 iv over 2 hrs before 5-FU, d1 and 2
5-FU 400 mg/m2 iv bolus and then 600 mg/m2 iv over 22 hrs, d 1 and d2 Oxaliplatin (Eloxatin) 85 mg/m2 iv d1 Q2w x 12 cycles
 85 mg/m2 iv d1 Q2w x 12 cycles.")
34
FOLFOX6 Leucovorin 400 mg/m2 iv over 2 hrs before 5-FU d1
5-FU 400 mg/m2 iv bolus d1 followed by 2400 mg/m2 iv over 46 hrs Oxaliplatin (Eloxatin) 100 mg/m2 in 500 ml dextrose 5% iv over 2 hours d1 Q2w x 12 cycles
 100 mg/m2 in 500 ml dextrose 5% iv over 2 hours d1. Q2w x 12 cycles.")
35
Modified FOLFOX6 Leucovorin 400 mg/m2 iv over 2 hrs before 5-FU d1
5-FU 400 mg/m2 iv bolus d1 followed by 2400 mg/m2 iv over 46 hrs Oxaliplatin (Eloxatin) 85 mg/m2 iv d1 Q2w x 12 cycles
 85 mg/m2 iv d1. Q2w x 12 cycles.")
36
FLOX 5-FU 500 mg/m2 iv bolus 1 hr after start of leucovorin qw x 6 weeks every 8 weeks for 3 cycles Leucovorin 500 mg/m2 iv over 2 hrs qw x 6 weeks every 8 weeks for 3 cycles Oxaliplatin (Eloxatin) 85 mg/m2 iv over 2 hrs before 5-FU and Leucovorin week 1, 3, 5 of each 8-week cycle for 3 cycles
 85 mg/m2 iv over 2 hrs before 5-FU and Leucovorin week 1, 3, 5 of each 8-week cycle for 3 cycles.")
37
XELOX Capecitabine (Xeloda) 1000 mg/m2 po bid x 14 days
Oxaliplatin (Eloxatin) 130 mg/m2 iv over 2 hrs d1 Q3w x 8 cycles
 130 mg/m2 iv over 2 hrs d1. Q3w x 8 cycles.")
38
Modified FOLFOX7 Leucovorin 200 mg/m2 iv d1
FU 2400 mg/m2 iv over 46 hrs Oxaliplatin (Eloxatin) 85 mg/m2 iv d1 Q2w x 12 cycles
 85 mg/m2 iv d1. Q2w x 12 cycles.")
39
Older patients derive as much benefit from 5-FU-based adjuvant chemotherapy as do younger patients, although the incremental benefit from oxaliplatin may be less We routinely recommend adjuvant chemotherapy for fit older patients with stage III and high-risk stage II colon cancer If an oxaliplatin regimen is chosen, we prefer the modified FOLFOX6 regimen in this population

40
For less fit individuals with stage III disease, patients who are deemed less likely to tolerate oxaliplatin, those with comorbid conditions that are likely to limit their five-year survival, and those with high-risk stage II disease, we suggest 5-FU/LV or single agent capecitabine rather than FOLFOX

41
Portal Vein Infusion Large, established hepatic metastases derive their blood supply primarily from the hepatic artery. However, tumors less than 5 mm in diameter obtain substantial portions of their blood supply from both the hepatic and portal circulations. Delivery of chemotherapy directly into the portal vein would appear to be a reasonable maneuver in the adjuvant treatment of colorectal cancer as the liver is the most common extraregional site of metastases. It would appear that cancer cells enter the liver through the portal vein along the same channels used by nutrients traveling from the gut. Initial dose-finding studies demonstrated that because of the extraction, or first-pass clearance of 5-FU by the liver, substantially higher doses of 5-FU can be safely given by intraportal than by intravenous infusion. The NSABP C-02 trial randomized 1,158 patients with Dukes A, B, or C colon cancers to either a 7-day portal vein infusion of 5-FU (600 mg/m2/day) or to surgery alone. A modest, albeit statistically significant, advantage in disease-free survival (74% vs. 64% at 4 years) was demonstrated for the group receiving intraportal chemotherapy; however, no difference was seen in the incidence of hepatic recurrences.
 or to surgery alone. A modest, albeit statistically significant, advantage in disease-free survival (74% vs. 64% at 4 years) was demonstrated for the group receiving intraportal chemotherapy; however, no difference was seen in the incidence of hepatic recurrences.")
42
Intraperitoneal Chemotherapy
The peritoneal cavity is drained by portal lymphatics into the portal vein. Intraperitoneal chemotherapy therefore delivers high concentrations of drug to the portal circulation, without the need for portal vein canalization. In addition, extremely high concentrations of chemotherapy can be given directly onto the peritoneal surfaces, thereby increasing local cytotoxicity. The high first-pass hepatic clearances of floxuridine and 5-FU make these drugs good agents for intraperitoneal administration. Pharmacokinetic studies of intraperitoneal 5-FU and floxuridine show that intraperitoneal administration of these agents results in intraperitoneal concentrations 200- to 400-fold higher than those achieved systemically. A randomized trial of 241 stage II and III patients compared intraperitoneal plus systemic 5-FU/leucovorin with systemic 5-FU/levamisole.With a 4-year median follow-up, no benefit was seen for the stage II patients. Among the 196 eligible patients with stage III disease, however, a 43% reduction in mortality was seen. This small trial is encouraging, but would require further corroboration before being accepted into standard practice.

43
STAGE IV

44
CEA measurements every 3 months, and
Follow up In summary, a rational postoperative surveillance program should include : CEA measurements every 3 months, and a yearly CT scan of the chest, abdomen, and pelvis (for rectal cancer) for the first 3 years. Colonoscopy can be performed every 3 to 5 years following the resection. COLON AND RECTUM
 for the first 3 years. Colonoscopy can be performed every 3 to 5 years following the resection. COLON AND RECTUM.")
45
Follow up At the time of CEA measurements, a physician encounter should be scheduled wherein a discussion of patient symptoms and a physical examination can be performed. If a rising serum CEA is detected on two consecutive measurements in the absence of imageable disease by CT scan, a PET scan with 18-FDG can be considered. COLON AND RECTUM

46
Follow up

47
Follow up

Similar presentations





 experience.>")





 Chemoimmunotherapy and Maintenance Lenalidomide in Relapsed/Refractory (R/R) Chronic Lymphocytic Leukemia (CLL) and Small.>")






![MOSAIC Stage ll+lll FOLFOX4 LV5FU2 Randomize. DFS DFS (months) Hazard ratio: 0.77 [0.65 – 0.92] p < 0.01 FOLFOX (n=1123) 77.9% LV5FU2 (n=1123) 72.8% FOLFOX.](/13/4012234/big_thumb.jpg "MOSAIC Stage ll+lll FOLFOX4 LV5FU2 Randomize. DFS DFS (months) Hazard ratio: 0.77 [0.65 – 0.92] p < 0.01 FOLFOX (n=1123) 77.9% LV5FU2 (n=1123) 72.8% FOLFOX.>")


