Download presentation
Presentation is loading. Please wait.

1
Induction of Labor

2
Objectives Definitions Indications and contraindications
Pregnancy dating Comparison of methods Management considerations

3
Induction initiation of uterine activity and cervical change with fetal descent by pharmacological or other means in a woman who is not in labor.

4
Cervical Ripening promotion of cervical change by pharmacological or other means not primarily intended to induce labor but to increase the success of subsequent induction

5
Contraindications to Induction
Any contraindication to labor

6
Indications for Induction
when continuation of the pregnancy is a greater risk to the mother or fetus than the risk of induction and delivery must be convincing, compelling, fully discussed and documented

7
Indications - Emergent
severe gestational hypertension suspected acute fetal compromise severe IUGR significant maternal disease not responding to treatment significant APH chorioamnionitis

8
Indications - Urgent PROM at term or near term
IUGR without evidence of acute compromise poorly controlled diabetes mellitus isoimmune disease at term or near term

9
Indications - Non-Urgent
'post-term' pregnancy well controlled diabetes mellitus intrauterine death in a prior pregnancy intrauterine fetal demise logistic problems (rapid labours, distance to hospital)
")
10
Indications - NOT elective induction
induction, in the absence of maternal or fetal indication, should not be undertaken

11
Risks of Induction failure to achieve labour
uterine hyperstimulation with fetal compromise uterine hyperstimulation with uterine rupture increase risk of C/S

12
Labour Induction Methods Likelihood of Successful Vaginal Delivery
MOST MOST favourable multiparous previous vaginal cervix delivery unfavourable nulliparous cervix previous C/S LEAST LEAST

13
If attempted induction does not achieve labor reevaluate the indication and method of induction

14
Methods of induction include mechanical and pharmacological means.
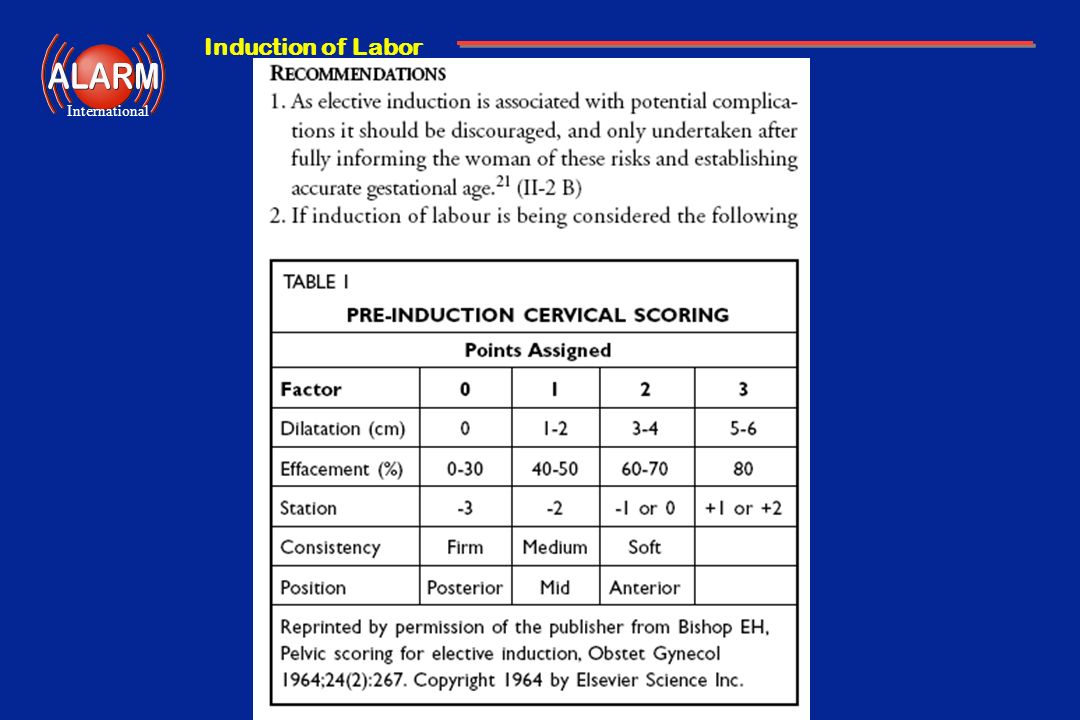
The best choice depends on the cervical score (A cervix is unfavorable if the Bishop score is < 6)
")
15
Bishop Scoring System Factor 1 2 3 Dilatation (cm) 1 - 2 3 - 4 > 5
Score Factor 1 2 3 Dilatation (cm) 1 - 2 3 - 4 > 5 Effacement (%) 0 - 30 > 80 Consistency Firm Medium Soft Position Posterior Mid Anterior Sp -3 or Sp +1 or Station Sp -2 Sp -1 or 0 above lower
 > 5. Effacement (%) > 80. Consistency. Firm. Medium. Soft. Position. Posterior. Mid. Anterior. Sp -3 or. Sp +1 or. Station. Sp -2. Sp -1 or 0. above. lower.")
16
Effect of Cervical Status on C/S Rate
50 Nulliparous Parous 40 34 30 23 20 Cesarean Section (%) 20 13 12 6 10 0-3 >3 Spontaneous Labour Cervical dilatation at induction Xenakis Obstet Gynecol (1997) 90: 235
 >3. Spontaneous Labour. Cervical dilatation at induction. Xenakis Obstet Gynecol (1997) 90: 235.")
17
Labour Induction - Unfavourable Cervix
Stripping of membranes Cervical ripening followed by oxytocin laminaria / artificial tents Foley catheter prostaglandins Prostaglandins (intracervical or vaginal) Amniotomy or oxytocin
 Amniotomy or oxytocin.")
18
Mechanical Methods catheters and tents
cause cervical softening and effacement this may facilitate an early amniotomy these methods are effective by producing local prostaglandin along with direct dilatation less hypertonus and FH rate abnormalities than with pharmacologic agent

19
Prostaglandin Preparations
Vaginal preparations are: easier to administer easier to remove less likely to be placed extra-amniotically less likely to cause patient discomfort

20
Prostaglandin E2 myometrial contraction cervix
causes collagen breakdown and proteoglycan deposition vasodilator bronchodilator GI motility and secretory effects

21
Prostaglandin E2 - Route and Dose
intracervical (Prepidil ) prostaglandin E mg into cervical canal vaginal (Prostin E2 vaginal gel ) prostaglandin E2 1 or 2 mg into posterior fornix vaginal (Cervidil vaginal insert) prostaglandin E2 10 mg into posterior fornix any formulation may be used for cervical ripening
 prostaglandin E2 0.5 mg into cervical canal. vaginal (Prostin E2 vaginal gel ) prostaglandin E2 1 or 2 mg into posterior fornix. vaginal (Cervidil vaginal insert) prostaglandin E2 10 mg into posterior fornix. any formulation may be used for cervical ripening.")
22
Guidelines for PGE2 Use insertion in hospital by experienced caregiver
monitor appropriately for FHR and uterine activity if labour develops manage as appropriate if no labour, reassess, repeat as necessary or choose an alternative induction method

23
Prostaglandin E2 - Advantages
improved patient acceptance lower operative delivery rate less need for oxytocin induction may be used in PROM cost considerations

24
Prostaglandin E2 - Disadvantages
adverse reactions hyperstimulation CVS events nausea, vomiting, diarrhea gel preparations are difficult to remove cost considerations

25
Precautions with Prostaglandins
avoid placing PG’s adjacent to myometrium use cautiously in patients with previous C/S do not repeat more frequently than every 6 hours wait 6 hours prior to oxytocin infusion following gels may be started 30 minutes after Cervidil removal do not use for augmentation

26
Labour Induction - Favourable Cervix
Stripping of membranes Amniotomy Oxytocin Vaginal prostaglandins

27
Amniotomy creates commitment to delivery
effective with favourable cervix often used in conjunction with oxytocin caution in cases of high presenting part ( risk of cord prolapse)
")
28
Oxytocin Effects myometrial contraction cervix - no direct effect
vasoactive hypotension possible with bolus IV administration antidiuretic activity water intoxication possible with high dose oxytocin

29
Oxytocin Guidelines cervix should be favourable
experienced caregivers and access to caesarean delivery auscultation or EFM depending on indication administration intravenous concentrations vary but avoid large free water load

30
Uterine Hypertonus discontinue oxytocin if in use intravenous bolus
prepare for emergency delivery consider tocolytic agents ritodrine at mg/min IV until desired effect nitroglycerin 50 mg IV push to maximum of 200 mg nitroglycerin spray sublingual

31
Post partum consideration:
if oxytocin was used in labor, PPH may occur for all induced patients , give oxytocin bolus post partum ( oxytocin 10 units I.M. 20 units 1L at 100 cc/hr for 2 hours or more

32
Conclusions reasons for induction must be compelling, convincing and documented risk and benefits must be discussed with patient patient preference must be considered ripen the cervix as much as possible match the method with the urgency and cervical status do not use oxytocin if cervix unfavourable don't overestimate your ability to succeed

33
happy baby + happy mom + vaginal delivery
Goal of Induction avert anticipated adverse outcome associated with continuation of pregnancy to effect uterine activity sufficient for cervical change and fetal descent without causing uterine hyperstimulation or fetal compromise to allow as natural a birthing experience as safely possible and maximize maternal satisfaction happy baby + happy mom + vaginal delivery

Similar presentations












>")










