Download presentation
Presentation is loading. Please wait.

1
Abnormal labor: Protraction and arrest disorders
E.Naghshineh M.D

3
labor abnormalities : protraction disorders (ie, slower than normal progress) arrest disorders (ie, complete cessation of progress) most common indication for primary cesarean delivery(68%) Prevalence :20 % The risk is highest in nulliparous women with term pregnancies
 Prevalence :20 % The risk is highest in nulliparous women with term pregnancies.")
4
three stages of labor: First stage :from onset of contractions to complete cervical dilation. Second stage :from complete cervical dilation to expulsion of the fetus Third stage :from expulsion of the fetus to expulsion of the placenta

5
two phases: Latent phase :regular contractions, typically mild and infrequent,change in cervical dilation and effacement is gradual, less than 1 cm dilation over a single hour. Active phase :painful contractions of increasing frequency, intensity, and duration accompanied by more rapid cervical change (at least 1 cm/hour)
")
6
Friedman divided labor :first and second stage
first stage :latent phase, acceleration phase, phase of maximum slope, and a deceleration phase (figure 1). acceleration phase :occur at 3 to 4 cm cervical dilation minimum rate of acceptable cervical dilation during the active phase of labor : 1.2cm/hour for nulliparous ,1.5 cm/hour for multiparous -relatively slow rate of cervical dilation until approximately 4 cm (ie, latent labor), followed by an abrupt acceleration in the rate of dilation until a deceleration phase at approximately 9 cm
. acceleration phase :occur at 3 to 4 cm cervical dilation. minimum rate of acceptable cervical dilation during the active phase of labor : 1.2cm/hour for nulliparous ,1.5 cm/hour for multiparous. -relatively slow rate of cervical dilation until approximately 4 cm (ie, latent labor), followed by an abrupt acceleration in the rate of dilation until a deceleration phase at approximately 9 cm.")
8
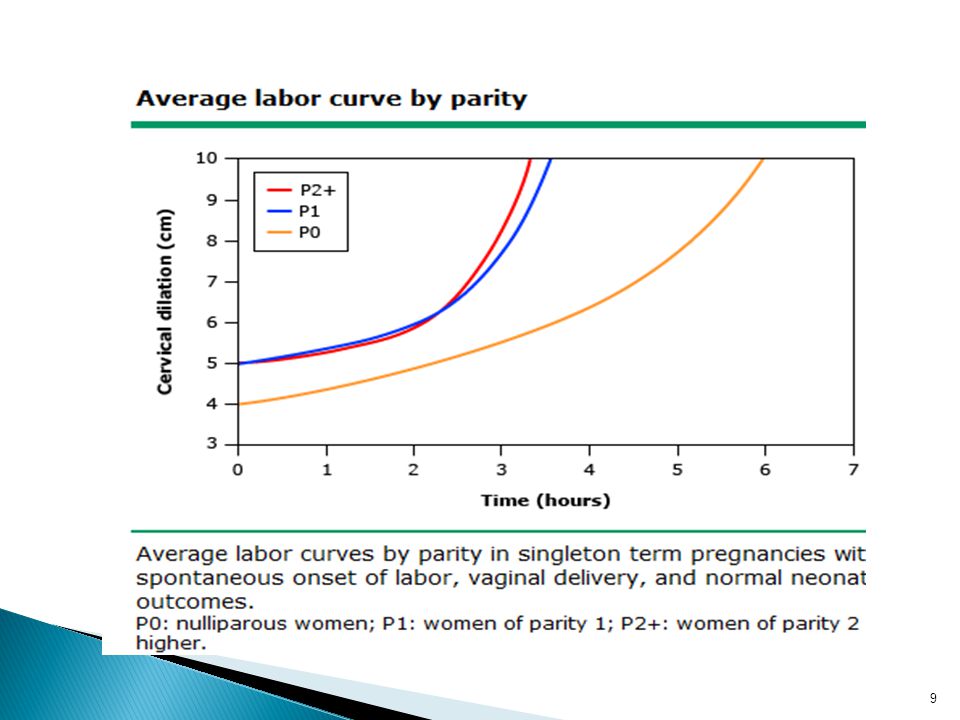
Friedman versus contemporary data Labor curve:
The shape of the labor curve generated from Zhang’s data (figure 2) is different from Friedman’s (figure 1). Zhang’s curves : increase more gradual, greater than 50 % do not dilate at a rate of >1 cm/hour until 5 to 6 cm dilation, not observe a deceleration phase
 is different from. Friedman’s (figure 1). Zhang’s curves : increase more gradual, greater than 50 % do not dilate at a rate of >1 cm/hour until 5 to 6 cm dilation, not observe a deceleration phase.")
10
Other authors’ : rate of cervical change between 3 and 6 cm much slower than previously thought , less than 1 cm per hour prior to 5 to 6 cm (table 1).
.")
11
Duration of the latent phase :
Average latent phase: -nulliparous:6.4 hours -multiparous:4.8 hours Prolonged latent phase: -nulliparous ≥20 hours -multiparous ≥14hours The duration of latent phase in the induced labor is controversial, but appears to be longer than in spontaneous labor

12
Duration of the active phase :
nulliparous =4.6 hour Friedman: multiparous=2.4hours Zhang :nulliparous=5.3hours- multiparous=3.8hours - duration of the first stage (defined as from 4 to 10 cm) was significantly longer in induced labor than in spontaneous labor
 was significantly longer in induced labor than in spontaneous labor.")
13
Duration of the second stage :
Induction does not affect the duration of the second stage of labor Friedman: nulliparous =3 hours, multiparous=1hours Zhang :nulliparous=0.6hours, multiparous=0.2hours

14
DIAGNOSIS OF LABOR ABNORMALITIES :
Protraction and arrest can occur anytime during labor. The thresholds are defined according to the phase or stage of labor when they occur.

15
1.2cm/hour for nulliparous ,1.5 cm/hour for multiparous Zhang’s :
Active phase: Friedman: minimum rate of acceptable cervical dilation during the active phase of labor : 1.2cm/hour for nulliparous ,1.5 cm/hour for multiparous Zhang’s : rates of dilation in the first stage slower , Labor accelerates much faster after 6 cm, and is significantly faster inregardless of parity. multiparas compared to nulliparas.

16
Second stage: longer than 2 hours in nulliparas , 1 hour in multiparas Zhang: in nulliparous over 2.5 to 3 hours ; in multiparous 1 hour

17
Precipitous labor : labor that lasts no more than 3 hours from onset of contractions to delivery

18
Etiology And Risk Factors :
Hypocontractile uterine activity : most common cause ،either not sufficiently strong or not appropriately coordinated to dilate the cervix and expel the fetus، 3 to 8%of parturients Normal uterine activity : palpation, external tocodynamometry, or internal uterine pressure catheter Cephalopelvic disproportion (CPD)
")
19
Neuraxial anesthesia : uterine activity, fetal malposition, ultimately arrest disorders, significant increases in the second stage of labor and use of oxytocin , more likely to undergo operative vaginal delivery Bandl's ring : An hourglass constriction ring of the uterus, not clear if it is the cause or the result of the associated dystocia Occiput posterior (OP) position : longer duration of active labor and the second stage, higher risk of arrest of descent requiring operative delivery Maternal obesity : increasing length of the first stage of labor, not independently correlated with the second stage of labor
 position : longer duration of active labor and the second stage, higher risk of arrest of descent requiring operative delivery. Maternal obesity : increasing length of the first stage of labor, not independently correlated with the second stage of labor.")
20
Management Patients With Protracted Latent Phase:
Therapeutic rest Uterotonic drugs

21
Therapeutic rest Morphine SC (15 to 20 mg) or IM (10 mg), 85%wake up in the active phase of labor, 10 % will not be in labor ( false labor), 5 % will have a persistent dysfunctional; zolpidem (5 mg PO) and secobarbital (100 mg PO) are two commonly prescribed agents.
 and secobarbital (100 mg PO) are two commonly prescribed agents.")
22
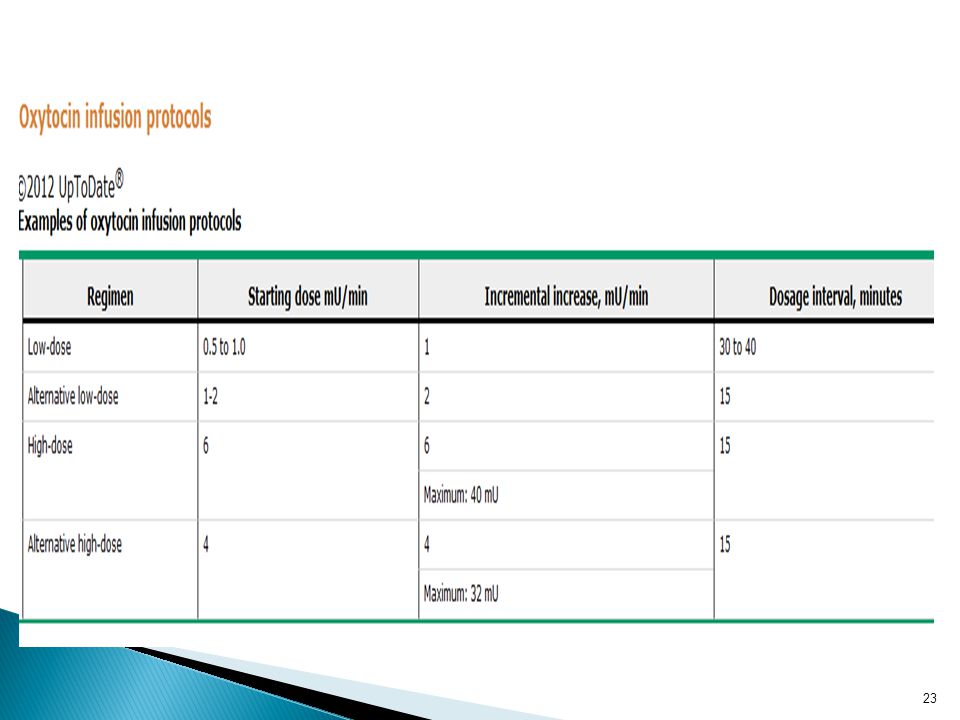
Oxytocin Friedman :oxytocin and therapeutic rest equally efficacious and safe,average interval between initiation of oxytocin and active labor was 3.4 hours Prostaglandins not been studied as a treatment for women diagnosed with prolonged latent phase Amniotomy increase in maternal plasma prostaglandin concentration , the effects on the uterus and cervix are probably insufficient to result in significant augmentation of labor

24
Cesarean delivery should not be performed in women in latent phase unless evidence of maternal or fetal deterioration necessitating prompt delivery, a contraindication to vaginal delivery, or induction of labor with oxytocin fails

25
Consequences Of Prolonged Latent Phase
associated with a higher risk of C/S Friedman : not more prone to developing active phase protraction and arrest disorders, perinatal mortality was not increased Others:associated with a higher risk of subsequent labor abnormalities, newborns are more exposed to thick meconium, have depressed five-minute Apgar scores, and require NICU admission

26
Patients with protracted active phase :
confirm that the patient is in the active phase (cervix is at least 5 to 6 cm), administer oxytocin, and wait four hours Oxytocin augmentation : Oxytocin is the only medication (FDA approved) for labor stimulation in the active phase. Decreased the c/s rate , increased rate NVD Decreased the total duration of labor Increased the frequency of tachysystole Resulted in similar maternal and neonatal morbidities
, administer oxytocin, and wait four hours. Oxytocin augmentation : Oxytocin is the only medication (FDA approved) for labor stimulation in the active phase. Decreased the c/s rate , increased rate NVD. Decreased the total duration of labor. Increased the frequency of tachysystole. Resulted in similar maternal and neonatal morbidities.")
27
Assessing progress after initiating oxytocin :
the 2hour threshold is not highly predictive that the patient will fail to deliver vaginally. A better threshold is a minimum change in cervical dilation of 2 cm over4 hours , safe and increased the rate of vaginal delivery Intrauterine pressure catheter : no reduction in the rate of operative delivery or improvement in perinatal outcome

28
Other approaches Amniotomy —not accelerate spontaneous labor Prostaglandins —not Evaluation of maternal hydration status and increased intravenous fluids(250 ml/h) DW5%:lower frequency of prolonged labor,less need for oxytocin Ambulation and continuous labor support : increase the comfort of the parturient, no effective
 DW5%:lower frequency of prolonged labor,less need for oxytocin. Ambulation and continuous labor support : increase the comfort of the parturient, no effective.")
29
OUTCOME increased risk of chorioamnionitis and cesarean delivery, not at significantly increased risk of adverse outcome

30
PREVENTION no strong evidence any intervention prevent protracted labor. The best evidence is for the combination of early initiation of oxytocin and amniotomy

Similar presentations