Download presentation
Presentation is loading. Please wait.

1
Dr Muhammad J Motiwala MD, FACP, Al Mafraq Hospital Abu Dhabi-UAE
Recent Update In The Management Of Invasive Candidiasis Dr Muhammad J Motiwala MD, FACP, Al Mafraq Hospital Abu Dhabi-UAE

2
Overview Invasive Fungal Infections Antifungal Agents
Polyenes Azoles Glucan Synthesis Inhibitors IDSA Treatment Guidelines

3
Review of our Fungal “Players”
Opportunistic fungi Normal flora Candida spp. Ubiquitous in our environment Aspergillus spp. Cryptococcus spp. Mucor spp. Endemic geographically restricted Blastomyces sp. Coccidioides sp. Histoplasma sp. Newly emerging fungi Fusarium Scedosporidium Trichosporin

4
Rank order of nosocomial bloodstream pathogens and their associated mortality
1 Coagulase negative-staphylococci 30.9 21 2 Staphylococcus aureus 15.7 25 3 Enterococci 11.1 32 4 Candida species 9 38 5 Escherichia coli 5.7 24 6 Klebsiella species 5.4 27 7 Enterobacter species 4.5 28 8 Pseudomonas species 4.4 33 Serratia species 1.4 26 10 Viridans streptococci 23

7
Predisposing Factors to Fungal Infections (IFI)
Broad spectrum antibiotics Immunosuppression Corticosteroids Prolonged hospitalization (ICU Stay) TPN (intravascular catheter use) Prolonged neutropenia Hemodialysis /Acute Renal Failure Diabetes Mellitus Mechanical Ventilation Recent gastrointestinal / Cardiac surgery Burns Colonization
 TPN (intravascular catheter use) Prolonged neutropenia. Hemodialysis /Acute Renal Failure. Diabetes Mellitus. Mechanical Ventilation. Recent gastrointestinal / Cardiac surgery. Burns. Colonization.")
9
Incidence of Invasive Fungal Infections
Solid Organ Transplant % Kidney – 14% Heart – 32% Heart-Lung/Lung 15 – 36% Pancreas 18 – 38% Liver – 42 % Bone Marrow Transplant % Intensive Care Unit 17% Singh, N. CID 2000; 31:545-53 Vincent JL. Intensive Care Med 1998; 24:

10
Mortality Rates Candidemia has a mortality rate of ~40%.
Invasive aspergillosis continues to be a highly lethal opportunistic infection: 375% increase in mortality due to Aspergillus species from 1980 to 1997. Overall mortality rate in patients with invasive aspergillosis is reported to be 58%. Mortality continues to be high regardless of the antifungal therapy used. Edmond MB et al. CID 1999;29: National Center for Health Statistics ( ) Lin S et al. CID 2001;32:
 Lin S et al. CID 2001;32:")
11
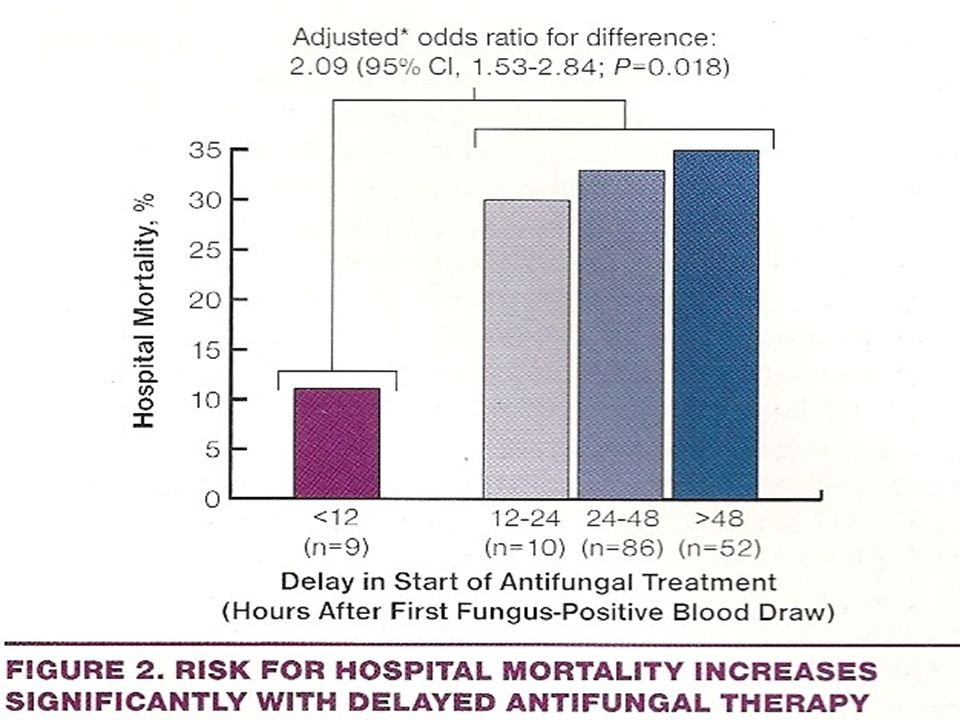
Challenges Delaying antifungal therapy until blood cultures are positive is associated with increased mortality Diagnostic limitations

13
Clinical approaches to assess risk
Fungal colonizing index: the greater the number of positive sites, the greater the increased risk for invasive infection Combine colonization with other risk factors: surgery on admission, TPN, and sepsis No colonisation index but include variables: ≥ 4 days in ICU, CVC, DM, new hemodialysis, TPN, and broad-spectrum antibiotics Pittet D. Ann Surg. 1994;220: Paphitou NI. Med Mycol. 2005;43:

14
Colonization in ICU patients
Prevalence of colonization in ICU is high (50% to 70% or more) compared with relatively low rate of infection, so predictive value of colonization is poor However colonisation with unexplained fever, leukocytosis, and hypotension may indicate invasive candidiasis Ostrosky-Zeichner L. Crit Care Med. 2006;34: Eggimann P. Lancet Infect Dis. 2003;3:
 compared with relatively low rate of infection, so predictive value of colonization is poor. However colonisation with unexplained fever, leukocytosis, and hypotension may indicate invasive candidiasis. Ostrosky-Zeichner L. Crit Care Med. 2006;34: Eggimann P. Lancet Infect Dis. 2003;3:")
15
CI is ratio of # of sites positive to total number of sites tested.
CCI is CI times the ratio of # of sites with heavy growth to the total # of positive sites.

16
Which antifungal to choose?
Candida speciation may take up to 5 days and fluconazole susceptibility testing may take an additional 5 days In patients who are critically ill, hypotensive with multi-organ failure, most authorities would favour the initial use of IV amphotericin. This recommendation was based on efficacy trends that favoured IV amphotericin over Iv fluconazole (but were not statistically different) and that candidemia was cleared faster with IV amphotericin compared to fluconazole
 and that candidemia was cleared faster with IV amphotericin compared to fluconazole.")
17
Targeted anti-fungal therapy The “challenging” wisdom
Withhold Antifungal therapy unless positive diagnostic test Advantages Directed therapy, ?less cost, less anti-fungal toxicity Disadvantages Variable sensitivity and specificity diagnostic tests Unproven benefit in reducing mortality, ?costs 17

19
Treatment options of invasive fungal infections in adults
Treatment options of invasive fungal infections in adults. Swiss Med Wkly Jul 22;136(29-30):447-63
:")
20
Spellberg BJ et al. Clin Infect Dis. 2006 Jan 15;42(2):244-51
:244-51")
21
Diagnostic Dilemma Clinical Setting: with other risk factors
Radiology: applicable more for Aspergillus Cultures: Low yield and longer time Staining: GMS and Calcofluor white PCR Assay: not widely available 1-3 Beta Glucan Assay: Galactomannan Assay: For Aspergillus PNA FISH:

23
PNA FISH: Clinical Benefits Summary
Rapid and accurate identification of bloodstream pathogens direct from positive blood cultures Simple to implement and easy to use Maintains species morphology Actionable PNA FISH results for 95% of BC+ Development of new therapeutic guidelines Improved patient safety Early appropriate and effective antibiotic therapy Reduction in mortality Reduction in unnecessary antimicrobial and antifungal use Reduction in hospital length of stay (LOS) Significant cost savings 25 March 2017 23
 Significant cost savings. 25 March")
24
Antifungal choice Organism (proven, suspected) Site of disease
Host factors (eg age, neutropenia, mucositis) History of antifungal therapy and/or prophylaxis Tolerability/ side effects Drug-Drug interactions Costs 24
 History of antifungal therapy and/or prophylaxis. Tolerability/ side effects. Drug-Drug interactions. Costs. 24.")
25
ANTI FUNGAL AGENTS

26
Antifungal Drug Development
1950s 1960s 1970s 1980s 1990s 2000s Griseofulvin Ketaconazole Fluconazole Itraconazole Terbinafine AMB lipid Formulations Econazole, miconazole(IV) Itra (IV) Caspofung Voricon Micafung Anidulofung Posacon Ravucon AMBd 5FC miconazole (top) clotrimazole (top)
 Itra (IV) Caspofung. Voricon. Micafung. Anidulofung. Posacon. Ravucon. AMBd. 5FC. miconazole (top) clotrimazole (top)")
27
Antifungal agents Polyenes (cell membrane)
Conventional Amphotericin B Lipid formulations Ambisome, Abelcet, Amp B Colloidal Dispersion Triazoles (sterol synthesis) Fluconazole, Itraconazole, Voriconazole, Posaconazole Ravuconazole Echinocandins (cell wall) Caspofungin Anidulofungin, Micafungin Allyamines (sterol synthesis) Terbinafine
 Fluconazole, Itraconazole, Voriconazole, Posaconazole. Ravuconazole. Echinocandins (cell wall) Caspofungin. Anidulofungin, Micafungin. Allyamines (sterol synthesis) Terbinafine.")
28
Biochemical Targets for Antifungal Chemotherapy
Arrangement of the biomolecular components of the cell wall accounts for the individual identity of the organism. Although, each organism has a different biochemical composition, their gross cell wall structure is similar. Antifungal agents targeted towards: Inhibition of fungal cell wall synthesis – caspofungin is a -glucan synthesis inhibitor; several more compounds are under investigation Inhibition of fungal cell membrane synthesis – ergosterol is the target (cell membranes of fungi and mammals contain different sterols): polyenes, azoles, triazoles, alkylamines Inhibition of cell division – microtubule effects: griseofulvin; DNA: flucytosine.
: polyenes, azoles, triazoles, alkylamines. Inhibition of cell division – microtubule effects: griseofulvin; DNA: flucytosine.")
29
Antifungal Agents- Sites of action
Echinocandins Inhibit fungal cell wall biosynthesis Griseofulvin Inhibits mitotic spindle formation

30
B-1,3 Glucan Synthase Caspofungin B-1,6 Glucan B-1,3 Glucan Cell Wall Phospholipid Bilayer AMB Ergosterol Zymosterol 14 Me-fecosterol Azoles Lanosterol Azoles Terbinafine Squalene

Similar presentations

















 can be both superficial and systemic. Superficial infections (Oral and vulvovaginal candidiasis, Dermatophytosis,>")


 to lanosterol.>")



