Download presentation
Presentation is loading. Please wait.

1
Treatment of Fungal infections in Hematologic Malignancies
George Samonis M.D. PhD Professor of Medicine The University of Crete

2
Challenges of Diagnosing Opportunistic Infections at the Bedside
At the bedside of a patient with an opportunistic infection, the clinician is often more concerned with treating signs and symptoms or diagnosing a syndrome than identifying and treating the causative pathogen, which may be of bacterial, viral, or fungal origin. 2

3
Challenges of Diagnosing Opportunistic Infections at the Bedside
In this presentation, we will focus on diagnostic challenges and treatment approaches in the management of invasive fungal infections. 3

4
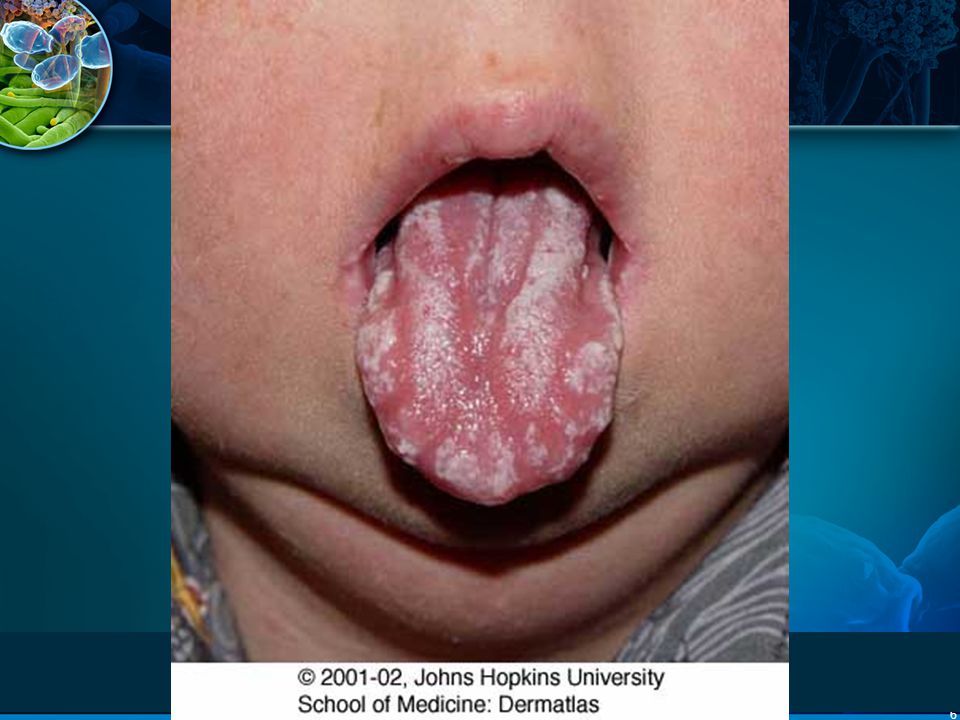
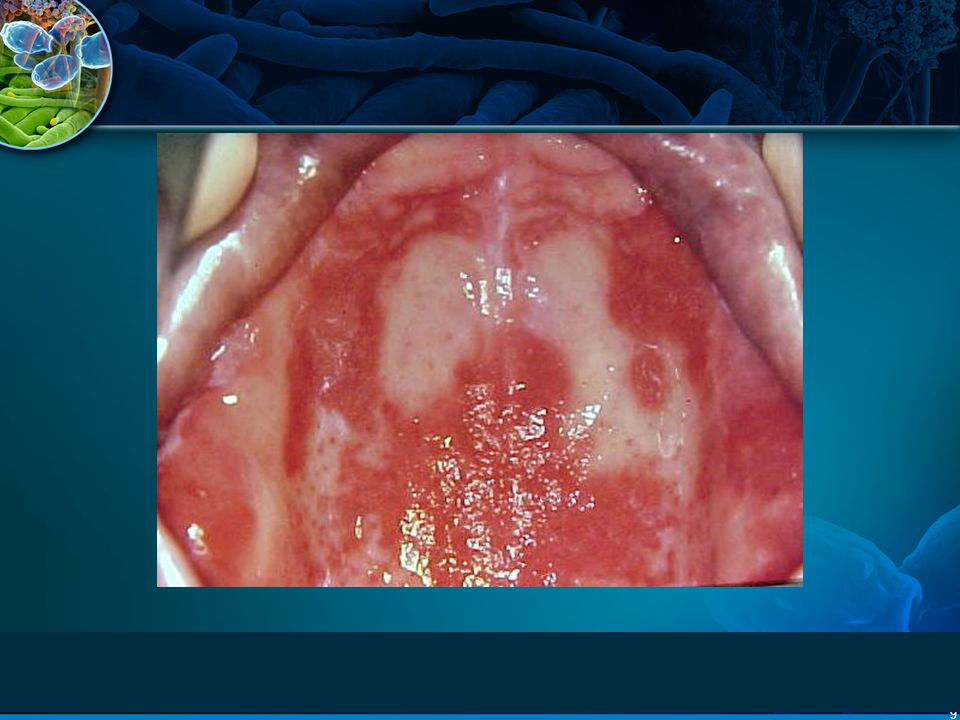
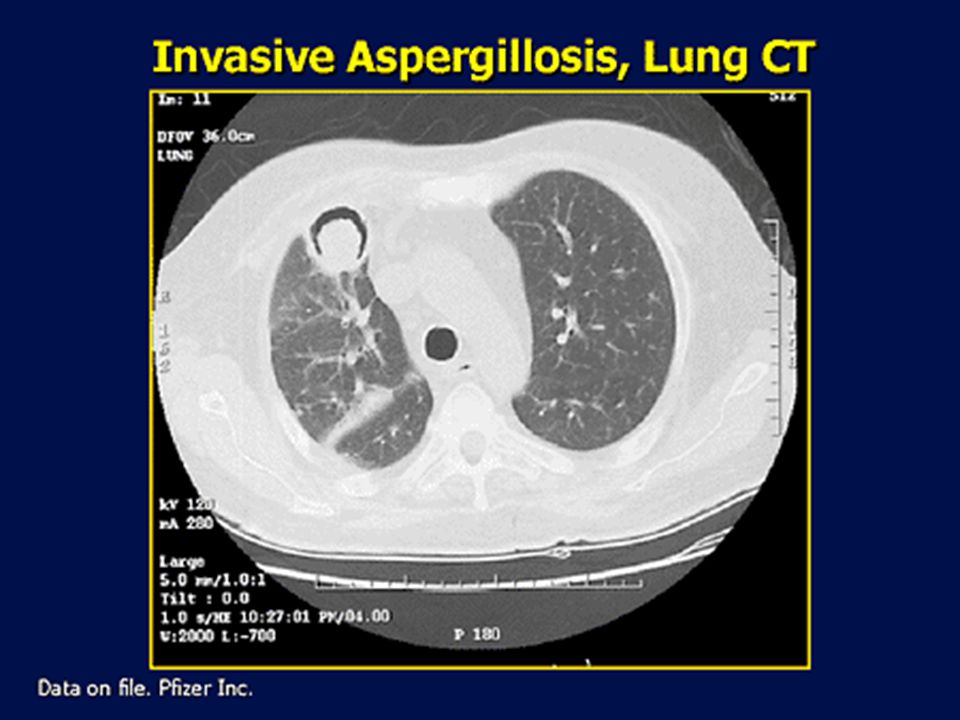
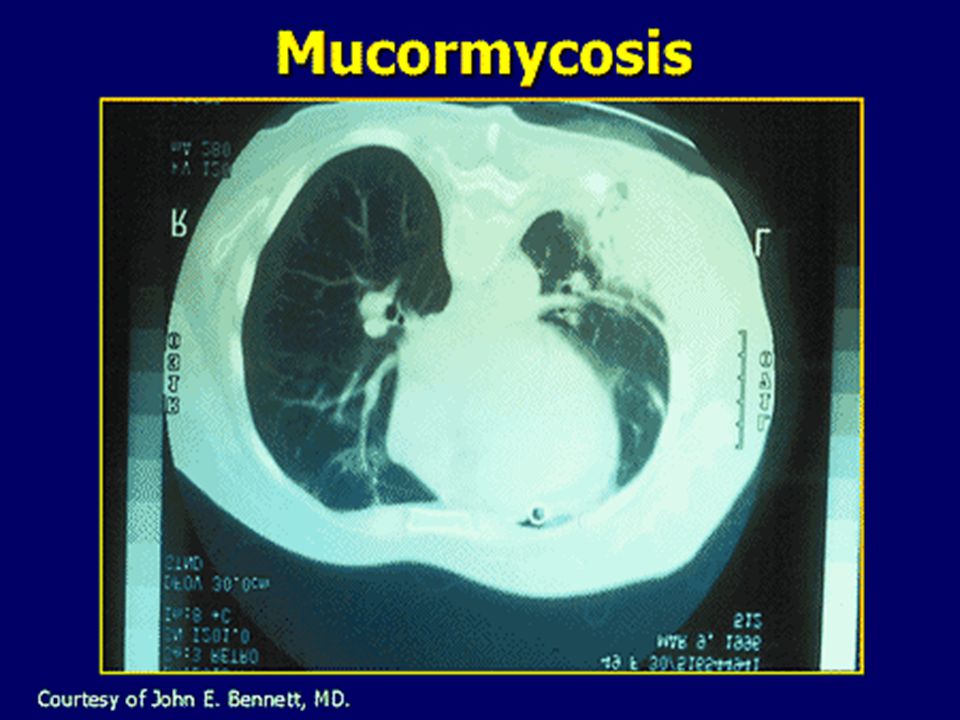
Usual fungal infections in immunocompromised patients
Candidiasis Aspergillosis Mucormycosis Fusariosis Cryptococcosis

5
Risk factors for development of IFIs
Neutropenia Lymphopenia Corticosteroids Immunosuppressives Chemotherapy Bone Marrow Transplantation Broad-spectrum antibiotics Mucositis Parenteral alimentation Central venous catheters (CVCs) Hospital construction
 Hospital construction.")
32
Increased Incidence of Mould Infection
Aspergillus spp 13.0% 11.4% 11.0% 6.0% 4.0% A meta-analysis by Martino and Subira showed that a trend toward an increased incidence of infections after allogeneic HSCT caused by invasive mould infections, mostly Aspergillus. Relevant studies showed that the incidence of invasive candidiasis in these patients was demonstrated to be less than 5%. Martino R, Subira M. Invasive fungal infection in hematology: new trends. Ann Hematol. 2002;81: Wingard 1987 O’Donnell 1994 Morrison 1994 Baddley 2001 Martino 2002 Martino R, Subira M. Ann Hematol. 2002;81:

33
Distribution of IA in the Post-Engraftment Phase of HSCT
53% 30% Incidence of IA in HSCT 17% In a study that determined risks for IA in 1682 patients who received HSCTs between 1993 and 1998 at the Fred Hutchinson Cancer Research Center, 30% were diagnosed earlier than 40 days after stem cell transplantation and 53% were diagnosed between days 40 and 180. An additional 17% of infections developed more than 6 months after transplantation. This study confirmed a trend to later-onset IA in HSCT recipients (40 to 180 days post transplant). Marr KA, Carter RA, Boeckh M, et al. Invasive aspergillosis in allogeneic stem cell transplant recipients: changes in epidemiology and risk factors. Blood. 2002;100: <40 (n=57) (n=99) >180 (n=31) Number of Days Post HSCT Marr KA et al. Blood. 2002;100:
. Marr KA, Carter RA, Boeckh M, et al. Invasive aspergillosis in allogeneic stem cell transplant recipients: changes in epidemiology and risk factors. Blood. 2002;100: <40 (n=57) (n=99) >180 (n=31) Number of Days Post HSCT. Marr KA et al. Blood. 2002;100:")
34
Incidence of Aspergillosis in HSCT Recipients Is Growing
1-Year Cumulative Incidence of Aspergillosis at FHCRC* (%) 14 Allograft recipients Autograft recipients 12 10 8 Incidence (%) 6 4 Over the past 2 decades, infections caused by moulds, particularly Aspergillus spp., have become increasingly more common in HSCT recipients. The incidence of aspergillosis was evaluated at the Fred Hutchinson Cancer Research Center in HSCT recipients between 1992 and 1998.* Results from this study demonstrated that the incidence of aspergillosis in allograft recipients began to increase in 1992 and remained elevated though In autograft recipients, the incidence of invasive aspergillosis increased substantially after 1997, jumping from 1.1% in previous years to 5.3% in 1998. Marr KA, Carter RA, Crippa F, et al. Epidemiology and outcome of mould infections in hematopoietic stem cell transplant recipients. Clin Infect Dis. 2002;34: 2 1990 1991 1992 1993 1994 1995 1996 1997 1998 Year Data from 1990 through 1992 were obtained from another study. *FHCRC, Fred Hutchinson Cancer Research Center Adapted from Marr KA et al. Clin Infect Dis. 2002;34:
 14. Allograft recipients. Autograft recipients Incidence (%) Over the past 2 decades, infections caused by moulds, particularly Aspergillus spp., have become increasingly more common in HSCT recipients. The incidence of aspergillosis was evaluated at the Fred Hutchinson Cancer Research Center in HSCT recipients between 1992 and 1998.* Results from this study demonstrated that the incidence of aspergillosis in allograft recipients began to increase in 1992 and remained elevated though In autograft recipients, the incidence of invasive aspergillosis increased substantially after 1997, jumping from 1.1% in previous years to 5.3% in Marr KA, Carter RA, Crippa F, et al. Epidemiology and outcome of mould infections in hematopoietic stem cell transplant recipients. Clin Infect Dis. 2002;34: Year. Data from 1990 through 1992 were obtained from another study. *FHCRC, Fred Hutchinson Cancer Research Center. Adapted from Marr KA et al. Clin Infect Dis. 2002;34:")
35
Diminished T-cell function
Invasive Aspergillosis Risk Increases During the Post-Engraftment Period IA Risk IA Risk Neutropenia Immunosuppression: GVHD Corticosteroids Diminished T-cell function There is a bimodal distribution of risk for IFI during HSCT. Early risk for IA is associated with the neutropenic period, but the greatest risk period occurs late after transplantation in the setting of graft versus host disease (GVHD). This risk is particularly pronounced in non-myeloablative transplant regimens. In these regimens the duration of neutropenia is truncated, shifting the risk of IFI to the post-engraftment phase. In nonmyeloablative transplant, the strategy of using a graft versus tumor effect invariably leads to higher degrees of GVHD. This GVHD, and the immunosuppressive therapies used to manage it, place these patients at very high risk for IFI particularly due to moulds such as Aspergillus.1,2 Pre-engraftment Post-engraftment Marr KA. Oncology. 2001;15: Hagen EA et al. Clin Infect Dis. 2003;36:9-15. Marr KA. Antifungal prophylaxis in hematopoietic stem cell transplant recipients. Oncology. 2001;15:15-19. Hagen EA, Stern H, Porter D, et al. High rate of invasive fungal infections following nonmyeloablative allogeneic transplantation. Clin Infect Dis. 2003;36:9-15.
. This risk is particularly pronounced in non-myeloablative transplant regimens. In these regimens the duration of neutropenia is truncated, shifting the risk of IFI to the post-engraftment phase. In nonmyeloablative transplant, the strategy of using a graft versus tumor effect invariably leads to higher degrees of GVHD. This GVHD, and the immunosuppressive therapies used to manage it, place these patients at very high risk for IFI particularly due to moulds such as Aspergillus.1,2. Pre-engraftment. Post-engraftment. Marr KA. Oncology. 2001;15: Hagen EA et al. Clin Infect Dis. 2003;36:9-15. Marr KA. Antifungal prophylaxis in hematopoietic stem cell transplant recipients. Oncology. 2001;15: Hagen EA, Stern H, Porter D, et al. High rate of invasive fungal infections following nonmyeloablative allogeneic transplantation. Clin Infect Dis. 2003;36:9-15.")
36
Aspergillus-Related Mortality in Allogeneic HSCT Remains Relatively High
87.0% 71.0% 68.0% 56.0% 31.6%* The Aspergillus-associated mortality in HSCT recipients is between 32% and 87%. There has been a slight downward trend in associated mortality, perhaps due to coinciding with multiple changes in transplantation practices, including use of nonmyeloablative conditioning regimens, receipt of peripheral blood stem cells, more prompt diagnosis of IA, and the introduction of broad-spectrum triazoles and echinocandins.5 However, 32% associated mortality is still unacceptably high.1-5 Lin 20011 Cornet 20022 Thursky 20043 Cordonnier 20064 Upton 20075 Studies used crude mortality rate or attributable mortality rates. *Crude mortality rate at 4 months post IA diagnosis. 1. Lin SJ et al. Clin Infect Dis. 2001;32: Cornet M et al. J Hosp Infect. 2002;51: Thursky K et al. Bone Marrow Transplant. 2004;34: Cordonnier C et al. Clin Infect Dis. 2006;42: Upton A et al. Clin Infect Dis. 2007;44: Lin SJ, Schranz J, Teutsch SM. Aspergillosis case-fatality rate: systemic review of the literature. Clin Infect Dis. 2001;32: Cornet M, Fleury L, Maslo C, et al. Epidemiology of invasive aspergillosis in France: a six-year multicentric survey in the Greater Paris area. J Hosp Infect. 2002;51: Thursky K, Byrnes G, Grigg A, et al. Risk factors for post-engraftment invasive aspergillosis in allogeneic stem cell transplantation. Bone Marrow Transplant. 2004;34: Cordonnier C, Ribaud P, Hebrecht R, et al. Prognostic factors for death due to invasive aspergillosis after hematopoietic stem cell transplantation: a 1-year retrospective study of consecutive patients at French transplantation centers. Clin Infect Dis. 2006;42: Upton A, Kirby KA, Carpenter P, et al. Invasive aspergillosis following hematopoietic cell transplantation: outcomes and prognostic factors associated with mortality. Clin Infect Dis. 2007;44:

37
The Majority of IFIs Are Identified Post-mortem
Pre-mortem Post-mortem 33%† How Can We Better Identify Patients With IFI During Life? 12.3%* Identification of IFIs pre-mortem is significantly lower than the true incidence. In patients with hematologic malignancies, pre-mortem IFI incidence was 12.3%. Moulds were the predominant pathogens and 90% of the moulds were Aspergillus spp.1 When patients with hematologic malignancy who underwent autopsy exam at MD Anderson Cancer Center from were reviewed, prevalence of IFI at autopsy was 33%. Again, moulds were the predominant pathogens. Only 25% of the IFIs seen on autopsy were diagnosed pre-mortem.2 ` Pagano L, Caira M, Candoni A, et al. The epidemiology of fungal infections in patients with hematologic malignancies: the SEIFEM-2004 study. Haematologica 2006;91: Chamilos G, Luna M, Lewis RE, et al. Invasive fungal infections in patients with hematologic malignancies in a tertiary care cancer center: an autopsy study over a 15-year period ( ) Haematologica. 2006;91; Only 1/4 Diagnosed Pre-mortem Pagano 20061 Chamilos 20062 *Incidence of moulds and yeasts in AML patients (7.9% due to moulds). †Prevalence of invasive moulds and Candida (22% due to moulds). 1. Pagano L et al. Haematologica. 2006;91: Chamilos G et al. Haematologica. 2006;91:
 Haematologica. 2006;91; Only 1/4 Diagnosed Pre-mortem. Pagano Chamilos *Incidence of moulds and yeasts in AML patients (7.9% due to moulds). †Prevalence of invasive moulds and Candida (22% due to moulds). 1. Pagano L et al. Haematologica. 2006;91: Chamilos G et al. Haematologica. 2006;91:")
38
Invasive Aspergillosis Role of Early Diagnosis & Therapy
Have We Made Progress??

39
Non-Culture Based Diagnosis of Invasive Aspergillosis
Galactomannan Sandwich ELISA (Platelia) PCR 18s ribosomal DNA Multi-copy or single target genes b-D-glucan Amebocyte Limulus lysate Chromogenic (Glucatell, FungiTec G) Kinetic (Wako)
 PCR. 18s ribosomal DNA. Multi-copy or single target genes. b-D-glucan. Amebocyte Limulus lysate. Chromogenic (Glucatell, FungiTec G) Kinetic (Wako)")
40
Early diagnosis and treatment of invasive aspergillosis
Impact of early diagnosis of IA in patients with acute leukemia: 90% mortality when treatment instigated ≥ 10 days after first clinical or radiological sign of disease 40% mortality when treatment is instigated early Serial HR CT scanning: early and systematic high resolution CT scan in high-risk patients improves outcome Survival (%) IA: CT Scanning 100 Systematic CT 75 Non-Systematic CT 50 25 P = (Logrank Test) 50 100 150 200 Days After IPA (von Eiff M, et al. Ann Hematol. 1995) (Reprinted with permission from Caillot D, et al. J Clin Oncol. 1997)
 IA: CT Scanning Systematic CT. 75. Non-Systematic CT P = (Logrank Test) Days After IPA. (von Eiff M, et al. Ann Hematol. 1995) (Reprinted with permission from Caillot D, et al. J Clin Oncol. 1997)")
41
Hospital mortality (%) Delay in start of antifungal treatment (hours)
Relationship between hospital mortality and the timing of antifungal treatment 35 30 25 20 Hospital mortality (%) 15 10 This study provides further evidence that delayed treatment results in increased mortality.1 There is a need to focus on improved diagnosis of fungal infections, so that they can be treated early and adequately to reduce mortality. Morrell M, et al. Delaying the empiric treatment of Candida bloodstream infection until positive blood culture results are obtained: a potential risk factor for hospital mortality. Antimicrob Agents Chemother 2005; 49:3640–3645. 5 < 12 12–24 24–48 > 48 Delay in start of antifungal treatment (hours) Morrell M, et al. Antimicrob Agents Chemother 2005; 49:3640–5
 This study provides further evidence that delayed treatment results in increased mortality.1. There is a need to focus on improved diagnosis of fungal infections, so that they can be treated early and adequately to reduce mortality. Morrell M, et al. Delaying the empiric treatment of Candida bloodstream infection until positive blood culture results are obtained: a potential risk factor for hospital mortality. Antimicrob Agents Chemother 2005; 49:3640– < –24. 24–48. > 48. Delay in start of antifungal treatment (hours) Morrell M, et al. Antimicrob Agents Chemother 2005; 49:3640–5.")
42
Patients with Satisfactory Treatment Response categorized by Baseline CT Findings
62% 52% 42% 41% 29% 16% *Note: Required positive mycology Greene R et al. ECCMID 2003

43
Utility of Galactomannan Detection in BAL Samples
# pt 160 Sens (%) Spec PPV NPV Serum 47 93 73 82 BAL 85 100 88 GM detection in CT-based BAL fluid has a high PPV for diagnosing IPA early in untreated patients Becker et al. Br J Haematol 2003; 121: 448
 Spec. PPV. NPV. Serum BAL GM detection in CT-based BAL fluid has a high PPV. for diagnosing IPA early in untreated patients. Becker et al. Br J Haematol 2003; 121: 448.")
44
Treatment definitions
Prophylactic therapy: Use of antifungals from chemotherapy until prolonged febrile neutropenia Chance of infection: remote Empirical therapy: Use of antifungals from febrile neutropenia to culture and/or tissue evidence of fungal infection Chance of infection: possible Preemptive therapy: Use of antifungals based on early clinical and/or laboratory markers of invasive disease Chance of infection: probable

45
Lack of Consensus on the Use of Empirical Antifungal Therapy
Pros Persistent or recurring fever of unknown origin >38C Reduces mortality Addresses diagnostic concerns Persistent neutropenia Absolute neutrophil count <500 cells/mm3 Cons Development of resistance Toxicity Cost There is a lack of consensus on the value of empirical antifungal therapy. It can help reduce the morbidity and mortality associated with many fungal infections and it addresses concerns about diagnostic difficulties. However, shortcomings include over treatment and emerging resistance, potential toxicity, and increased treatment costs when patients get therapy who don’t need it. Newer diagnostic tools are needed to more accurately and quickly identify patients in greatest need of antifungal therapy.1,2 Wingard JR. Empirical antifungal therapy in treating febrile neutropenic patients. Clin Infect Dis. 2004;39(suppl):S38-S43. Walsh TJ, Pappas P, Winston DJ, et al, for the National Institute of Allergy and Infectious Diseases Mycoses Study Group. Voriconazole compared with liposomal amphotericin B for empirical antifungal therapy in patients with neutropenia and persistent fever. N Engl J Med. 2002;346: Broad-Spectrum antibiotics >96 h Wingard JR. N Engl J Med. 2002;346:
:S38-S43. Walsh TJ, Pappas P, Winston DJ, et al, for the National Institute of Allergy and Infectious Diseases Mycoses Study Group. Voriconazole compared with liposomal amphotericin B for empirical antifungal therapy in patients with neutropenia and persistent fever. N Engl J Med. 2002;346: Broad-Spectrum antibiotics >96 h. Wingard JR. N Engl J Med. 2002;346:")
46
Antifungal treatment evolution
AMB deoxycholate 5-fluocytosine 1st generation azoles (ketoconazole, miconazole) 2nd generation triazoles (fluconazole, itraconazole) Lipid and liposomal formulations of AMB Extended spectrum triazoles (voriconazole, posaconazole) Echinocandins (caspofungin, micafungin, anidulafungin)
 2nd generation triazoles (fluconazole, itraconazole) Lipid and liposomal formulations of AMB. Extended spectrum triazoles (voriconazole, posaconazole) Echinocandins (caspofungin, micafungin, anidulafungin)")
47
Cellular Targets of Antifungal Therapy
Echinocandins: Target cell wall synthesis Polyenes: Target membrane function This figure identifies the cellular targets of each main class of antifungal agents Polyenes target fungal membrane function Polyenes bind to ergosterol, a sterol that is an important component of the fungal membrane1 The most significant difference between fungal and human cell membranes is the type of sterol present Ergosterol is the primary sterol in the fungal membrane and cholesterol is the primary sterol in the human cell membrane Polyene binding to ergosterol causes pores or channels to form in the fungal membrane, causing increased membrane permeability, leakage, and cell death Azoles target ergosterol synthesis1,2 Azoles inhibit synthesis of ergosterol by binding to 14- sterol demethylase, an enzyme required for ergosterol biosynthesis Inhibiting ergosterol synthesis causes abnormal fungal cell membrane formation and accumulation of toxic ergosterol precursors Echinocandins target cell wall synthesis1 Echinocandins inhibit the synthesis of glucan, a major structural polymer in the cell wall, by blocking the enzyme 1,3-glucan synthase Inhibiting glucan synthesis compromises cell wall integrity 1. Balkis MM, Leidich SD, Mukherjee PK, Ghannoum MA. Mechanisms of fungal resistance: an overview. Drugs. 2002;62: 2. Sheehan DJ, Hitchcock CA, Sibley CM. Current and emerging azole antifungal agents. Clin Microbiol Rev. 1999;12:40-79. Azoles: Target ergosterol synthesis

48
Fluconazole: Not a good choice for
empirical therapy in certain patients Pts on azole prophylaxis Pts with sinusitis or pneumonia Pts with prolonged neutropenia (e.g. leukemia) Pts with history of invasive aspergillosis (IA) or positive surveillance cultures for Aspergillus spp. Pts at institutions undergoing construction
 Pts with history of invasive aspergillosis (IA) or positive. surveillance cultures for Aspergillus spp. Pts at institutions undergoing construction.")
49
L-AMB vs. AMB for empirical therapy of febrile neutropenia
Ambisome AMB Patients 343 344 Acute Leukemia 168 165 Success 50 49 BFI (%) * 3.2 7.8 Infusion Fever (%) † 17 44 Nephrotoxicity (%) 19 34 * p= † p<0.001 Walsh NEJM 1999; 340:764
 * Infusion Fever (%) † Nephrotoxicity (%) * p=0.009 † p< Walsh NEJM 1999; 340:764.")
50
Polyene Therapy for Invasive Aspergillosis
Response % Historical Control 23% DAMB 29% ABCD 18% L-AMB 52% ABLC 42% Note: ABLC=amphotericin B lipid complex; L-AmB=liposomal amphotericin B; ABCD=amphotericin B colloidal dispersion; D-AMB=amphotericin B deoxycholate Hiemenz JW et al. Blood 1995;86(suppl 1):849a; Leenders ACAP et al. Br J Haem 1998;103:205; Bowden RA et al. Clin Infect Dis 2002;35:
:849a; Leenders ACAP et al. Br J Haem 1998;103:205; Bowden RA et al. Clin Infect Dis 2002;35:")
51
Number of days of Therapy Probability of Survival
Comparative Aspergillosis Study: Better Outcomes & Survival of Voriconazole Number of days of Therapy Probability of Survival Amphotericin B arm Voriconazole arm Hazard ratio = 0.60 95% CI (0.40, 0.89) Outcomes at wk 12 Vori AmB Survival % 57.9% Response 56.8% 31.6% Poor efficacy of AmB prior “gold standard” Vori recommended for primary therapy Questions? Role of Other Licensed Antifungal therapy Lipid for primary therapy Efficacy in high risk Combinations Herbrecht R et al NEJM 2002;347:408-15
 Outcomes at wk 12. Vori AmB. Survival 70.8% 57.9% Response 56.8% 31.6% Poor efficacy of AmB prior gold standard Vori recommended for primary therapy. Questions Role of Other Licensed Antifungal therapy. Lipid for primary therapy. Efficacy in high risk. Combinations. Herbrecht R et al NEJM 2002;347:")
52
Voriconazole vs. Ambisome in febrile neutropenia
LAMB (N=422) P Composite success 26% 31% NS Breakthrough fungal infections 1.9% 5% 0.002 Survival rate 87% 90% Toxicity-related withdrawal 13% 10% Nephrotoxicity (SCr>1.5) 11% 19% <0.001 Visual changes 4.3% 0.5% Walsh et al. N Engl J Med. 2002; 346:
 P. Composite success. 26% 31% NS. Breakthrough fungal. infections. 1.9% 5% Survival rate. 87% 90% Toxicity-related withdrawal. 13% 10% Nephrotoxicity (SCr>1.5) 11% 19% < Visual changes. 4.3% 0.5% Walsh et al. N Engl J Med. 2002; 346:")
53
Voriconazole: need for monitoring

54
Voriconazole Treatment

55
Subtherapeutic Voriconazole - Omeprazole

56
Posaconazole Posaconazole: broad spectrum of activity
only oral formulation variable absorption variable bioavailability Established for prophylaxis in acute leukemia and HSCT

58
Posaconazole

59
Echinocandins Latest class of antifungal drugs
First discovered in 1970s in screening programs for new antibiotics Cell-wall active agents: nhibition of (1, 3)-β-D glucan synthetase cell wall glucan depletion osmotic instability cell lysis
-β-D glucan synthetase cell wall glucan depletion osmotic instability cell lysis.")
60
Echinocandins Formerly known as Pneumocandins due to activity
against Pneumocystis carinii Rapidly fungicidal against most Candidae including azole-resistant strains Fungistatic against most Aspergillus spp Limited or no activity against Fusarium spp and Zygomycetes. No activity against Cryptococcus neoformans

61
Mechanism of action1-4 Mechanism of action involves a target specific for fungus4 Glucan is essential to fungal cell wall integrity2-4 Without it, fungal cells are osmotically fragile and easily lysed4 inhibitor of 1,3--D-glucan synthase1 Enzyme is present in fungal, but not mammalian, cells1 1- ECALTA® SPC. 2- Odds F.C., Brown A.J.P., Gow N.A.R. Antifungal agents: mechanism of action. Trends Microbiol. 2003;11: Debono M., Turner W.W., LaGrandeur L. et al. Semisynthetic chemical modification of the antifungal lipopeptide echinocandin B (ECB): structure-activity studies of the lipophilic and geometric parameters of polyarylated acyl analogs of ECB. J Med Chem. 1995;38(17): Raasch R.H. Anidulafungin: review of a new echinocandin antifungal agent. Expert Rev Anti Infect Ther. 2004;2:
: structure-activity studies of the lipophilic and geometric parameters of polyarylated acyl analogs of ECB. J Med Chem. 1995;38(17): Raasch R.H. Anidulafungin: review of a new echinocandin antifungal agent. Expert Rev Anti Infect Ther. 2004;2:")
62
CNS penetration: poor Dose: once daily
Echinocandins IV administration Long half life CNS penetration: poor Dose: once daily Little infusion related toxicity Little or no renal and hepatic toxicity Drug-drug interaction limited (cyclosporin) Potential combination with other antifungals (AMB or azoles) Animal data suggest synergistic effect Echinocandins: Caspofungin Anidulafungin Micafungin
 Potential combination with other antifungals (AMB or azoles) Animal data suggest synergistic effect. Echinocandins: Caspofungin Anidulafungin Micafungin.")
63
Echinocandins : In vitro activity1
Minimum inhibitory concentrations of the echinocandins against Candida species Anidulafungin Micafungin* Caspofungin Candida species MIC50 (µg/ml) MIC90 albicans 0.03 0.06-1 glabrata 0.13 0.03-1 0.06-2 tropicalis 0.06 0.25-1 dubliniensis 0.033 0.5 krusei 0.12-2 0.25-2 lusitaniae 0.25 2 0.5-1 1-2 parapsilosis 1 1-4 guilliermondii ND 2 -> 8 MIC50 or MIC90 = minimum inhibitory concentration for 50% or 90%, respectively, of tested strains; ND = not done. 1- Cappelletty D. et al. Reviews of therapeutics : the echinocandins Pharmacotherapy 2007, 27(3):
 MIC90. albicans glabrata tropicalis dubliniensis krusei lusitaniae parapsilosis guilliermondii. ND. 2 -> 8. MIC50 or MIC90 = minimum inhibitory concentration for 50% or 90%, respectively, of tested strains; ND = not done. 1- Cappelletty D. et al. Reviews of therapeutics : the echinocandins Pharmacotherapy 2007, 27(3):")
64
Caspofungin in Invasive Aspergillosis
% Well-documented disease Efficacy High risk pts Progressive infection Multiple prior antifungals Excellent tolerability Clinical utility No data for primary therapy Combination therapy Optimal dose not known Maertens J, et al. Clin Infect Dis 2004;39:

65
Efficacy of Caspofungin vs Empirical L-AmB in Neutropenic Patients*
Caspo (556) L-AmB (539) Composite Success % 33.7% Success Baseline Infections 14/27 (52%) 7/27 (26%) Breakthrough Infections (5.2%) 24 (4.5%) Etiological Agents* Aspergillus Candida Fusarium Zygomycetes Other *Patients may have had more than one organism Walsh TJ et al, New Eng J Med, 2004;351:
 L-AmB (539) Composite Success 33.9% 33.7% Success Baseline Infections 14/27 (52%) 7/27 (26%) Breakthrough Infections 29 (5.2%) 24 (4.5%) Etiological Agents* Aspergillus Candida Fusarium 1 0. Zygomycetes 2 0. Other 1 1. *Patients may have had more than one organism. Walsh TJ et al, New Eng J Med, 2004;351:")
66
Anidulafungin versus Fluconazole for Invasive Candidiasis.
Clinical data Anidulafungin vs Fluconazole Reboli A.C. et al. Anidulafungin versus Fluconazole for Invasive Candidiasis. N Engl J Med 2007;356:

67
Primary endpoint1 Global success at the end of IV therapy
ECALTA® demonstrated superiority vs fluconazole: Significantly greater response rate in the anidulafungin group Difference: 15.4% (95% CI: 3.9% to 27.0%) Mean (median) duration of IV therapy: fluconazole: (11) days anidulafungin: (14) days 1- Reboli A.C., Rotstein C., Pappas P.G. et al. Anidulafungin versus Fluconazole for Invasive Candidiasis. N Engl J Med 2007;356:
 Mean (median) duration of IV therapy: fluconazole: 12.1 (11) days. anidulafungin: 13.5 (14) days. 1- Reboli A.C., Rotstein C., Pappas P.G. et al. Anidulafungin versus Fluconazole for Invasive Candidiasis. N Engl J Med 2007;356:")
68
Phase III study micafungin vs. L-AmB Study design
Randomisation (1:1) Micafungin 100 mg/day* L-AmB 3 mg/kg/day Treatment period† 2–4 weeks‡ Post-treatment period 12 weeks Kuse et al. demonstrated the non-inferiority of micafungin to L-AmB in the treatment of adults with SCIs. Efficacy was assessed in both the modified intent-to-treat (mITT) and the per-protocol (PP) populations: In the mITT population, 247 patients received micafungin and 247 patients received L-AmB In the PP population, 202 patients received micafungin while 190 patients received L-AmB. Kuse ER, et al. Micafungin versus liposomal amphotericin B for candidaemia and invasive candidosis: a phase III randomised double-blind trial. Lancet 2007; 369:1519–1527. *2.0 mg/kg/day in patients weighing ≤ 40 kg †Treatment continued until at least one week after resolution of clinical signs and symptoms and obtaining of two sequential negative blood cultures ‡Maximum 8 weeks in chronic disseminated candidiasis, Candida osteomyelitis or Candida endocarditis Kuse ER, et al. Lancet 2007; 369:1519–27
 Micafungin 100 mg/day* L-AmB 3 mg/kg/day. Treatment period† 2–4 weeks‡ Post-treatment period. 12 weeks. Kuse et al. demonstrated the non-inferiority of micafungin to L-AmB in the treatment of adults with SCIs. Efficacy was assessed in both the modified intent-to-treat (mITT) and the per-protocol (PP) populations: In the mITT population, 247 patients received micafungin and 247 patients received L-AmB. In the PP population, 202 patients received micafungin while 190 patients received L-AmB. Kuse ER, et al. Micafungin versus liposomal amphotericin B for candidaemia and invasive candidosis: a phase III randomised double-blind trial. Lancet 2007; 369:1519–1527. *2.0 mg/kg/day in patients weighing ≤ 40 kg †Treatment continued until at least one week after resolution of clinical signs and symptoms and obtaining of two sequential negative blood cultures. ‡Maximum 8 weeks in chronic disseminated candidiasis, Candida osteomyelitis or Candida endocarditis. Kuse ER, et al. Lancet 2007; 369:1519–27.")
69
Phase III study micafungin vs. L-AmB Overall treatment success
100 Micafungin L-AmB 89.6 89.5 80 74.1 69.6 Treatment success rate (%) 60 40 Statistical analysis showed that micafungin was equivalent (non-inferior) to L-AmB on the primary endpoint of treatment success in both the mITT and PP populations. 1. Kuse ER, et al. Micafungin versus liposomal amphotericin B for candidaemia and invasive candidosis: a phase III randomised double-blind trial. Lancet 2007; 369:1519–1527. 20 n = 247 247 202 190 mITT PP Kuse ER, et al. Lancet 2007; 369:1519–27 mITT = modified intent-to-treat; PP = per-protocol set
 Statistical analysis showed that micafungin was equivalent (non-inferior) to L-AmB on the primary endpoint of treatment success in both the mITT and PP populations. 1. Kuse ER, et al. Micafungin versus liposomal amphotericin B for candidaemia and invasive candidosis: a phase III randomised double-blind trial. Lancet 2007; 369:1519– n = mITT. PP. Kuse ER, et al. Lancet 2007; 369:1519–27. mITT = modified intent-to-treat; PP = per-protocol set.")
70
Phase III study micafungin vs. caspofungin Study design
Patients were stratified by region and APACHE II score (≤ 20 or > 20) Randomisation (1:1:1) Micafungin 100 mg/day Micafungin 150 mg/day CAS 50 mg/day* Treatment period† Max 4 weeks† Post-treatment period 6 weeks‡ Pappas et al. compared two doses of micafungin with the standard dose of caspofungin in patients with confirmed SCIs. The primary efficacy population was the mITT population, which included 191 patients that received micafungin 100 mg/day, 199 patients that received micafungin 150 mg/day and 188 patients that received caspofungin. Pappas PG, et al. Micafungin versus caspofungin for treatment of candidemia and other forms of invasive candidiasis. Clin Infect Dis 2007; 45:883–893. *70 mg loading dose on Day 1 †8 weeks in chronic disseminated candidiasis or Candida endophthalmitis; switch to oral fluconazole permitted after 10 days in patients meeting protocol-specified criteria ‡Time from last dose day of protocol-defined antifungal therapy to final evaluation Pappas PG, et al. Clin Infect Dis 2007; 45:883–93 CAS = caspofungin
 Randomisation. (1:1:1) Micafungin 100 mg/day. Micafungin 150 mg/day. CAS 50 mg/day* Treatment period† Max 4 weeks† Post-treatment period. 6 weeks‡ Pappas et al. compared two doses of micafungin with the standard dose of caspofungin in patients with confirmed SCIs. The primary efficacy population was the mITT population, which included 191 patients that received micafungin 100 mg/day, 199 patients that received micafungin 150 mg/day and 188 patients that received caspofungin. Pappas PG, et al. Micafungin versus caspofungin for treatment of candidemia and other forms of invasive candidiasis. Clin Infect Dis 2007; 45:883–893. *70 mg loading dose on Day 1 †8 weeks in chronic disseminated candidiasis or Candida endophthalmitis; switch to oral fluconazole permitted after 10 days in patients meeting protocol-specified criteria ‡Time from last dose day of protocol-defined antifungal therapy to final evaluation. Pappas PG, et al. Clin Infect Dis 2007; 45:883–93. CAS = caspofungin.")
71
Phase III study micafungin vs. caspofungin Treatment success
80 76.4 71.4 72.3 60 Treatment success rate (%) 40 20 Analysis of the primary efficacy endpoint showed that treatment success rates were comparable between micafungin 100 mg/day, micafungin 150 mg/day and caspofungin, demonstrating similar efficacy across all three treatment arms. Micafungin was associated with treatment success in both candidaemia and deep invasive Candida infections. In the statistical analysis, the 95% CIs for the treatment difference between caspofungin and both micafungin 100 and micafungin 150 had lower bounds that were higher than –15%, the predefined limit of non-inferiority, and were therefore both non-inferior to caspofungin. On the secondary efficacy endpoints, there were no significant differences between the three treatment arms in terms of site of infection or incidence of recurrent invasive fungal infections (relapse) during the post-treatment period. As the lower daily dose of 100 mg/day was as effective as the higher 150 mg dose, 100 mg/day was selected as the dose of choice for the treatment of adult patients with SCIs. Pappas PG, et al. Micafungin versus caspofungin for treatment of candidemia and other forms of invasive candidiasis. Clin Infect Dis 2007; 45:883–893. n = 191 n = 199 n = 188 n = 191 199 188 Micafungin 100 mg/day Micafungin 150 mg/day Caspofungin 50 mg/day* Pappas PG, et al. Clin Infect Dis 2007; 45:883–93 *Loading dose 70 mg; mITT population
 Analysis of the primary efficacy endpoint showed that treatment success rates were comparable between micafungin 100 mg/day, micafungin 150 mg/day and caspofungin, demonstrating similar efficacy across all three treatment arms. Micafungin was associated with treatment success in both candidaemia and deep invasive Candida infections. In the statistical analysis, the 95% CIs for the treatment difference between caspofungin and both micafungin 100 and micafungin 150 had lower bounds that were higher than –15%, the predefined limit of non-inferiority, and were therefore both non-inferior to caspofungin. On the secondary efficacy endpoints, there were no significant differences between the three treatment arms in terms of site of infection or incidence of recurrent invasive fungal infections (relapse) during the post-treatment period. As the lower daily dose of 100 mg/day was as effective as the higher 150 mg dose, 100 mg/day was selected as the dose of choice for the treatment of adult patients with SCIs. Pappas PG, et al. Micafungin versus caspofungin for treatment of candidemia and other forms of invasive candidiasis. Clin Infect Dis 2007; 45:883–893. n = 191. n = 199. n = 188. n = Micafungin 100 mg/day. Micafungin 150 mg/day. Caspofungin 50 mg/day* Pappas PG, et al. Clin Infect Dis 2007; 45:883–93. *Loading dose 70 mg; mITT population.")
72
Micafungin vs Caspofungin in febrile neutropenia

73
Micafungin vs Caspofungin in febrile neutropenia
Conclusions Micafungin as effective and safe as caspofungin in empirical treatment of fungal infections in patients with febrile neutropenia

74
Empirical micafungin treatment of IFIs in hematologic malignancies

75
Empirical micafungin treatment of IFIs in hematologic malignancies

76
Micafungin vs fluconazole for prophylaxis of invasive fungal infections during neutropenia in hematopoietic stem cell transplantation patients Study endpoints Primary endpoint: treatment success (absence of proven, probable, or suspected systemic fungal infection until the end of prophylaxis therapy and the absence of a proven or probable systemic fungal infection until the end of the 42-day post-treatment period) Secondary endpoints included: use of systemic antifungal agents for treatment of suspected fungal infections; frequency of proven or probable fungal infections throughout the post-treatment period; pathogen-based frequency of proven infections The primary efficacy endpoint was treatment success, defined as absence of proven, probable, or suspected systemic fungal infection until the end of prophylaxis therapy and as the absence of a proven or probable systemic fungal infection until the end of the 4-week post-treatment period. Secondary efficacy endpoints included: use of systemic antifungal agents for treatment of suspected fungal infections, frequency of fungal colonisation, time to treatment failure and mortality. Safety analyses included adverse events, results of clinical laboratory tests and vital signs. van Burik JA, et al. Micafungin versus fluconazole for prophylaxis against invasive fungal infections during neutropenia in patients undergoing hematopoietic stem cell transplantation. Clin Infect Dis 2004; 39:1407–1416. van Burik JA, et al. Clin Infect Dis 2004; 39:1407–16
 Secondary endpoints included: use of systemic antifungal agents for treatment of suspected fungal infections; frequency of proven or probable fungal infections throughout the post-treatment period; pathogen-based frequency of proven infections. The primary efficacy endpoint was treatment success, defined as absence of proven, probable, or suspected systemic fungal infection until the end of prophylaxis therapy and as the absence of a proven or probable systemic fungal infection until the end of the 4-week post-treatment period. Secondary efficacy endpoints included: use of systemic antifungal agents for treatment of suspected fungal infections, frequency of fungal colonisation, time to treatment failure and mortality. Safety analyses included adverse events, results of clinical laboratory tests and vital signs. van Burik JA, et al. Micafungin versus fluconazole for prophylaxis against invasive fungal infections during neutropenia in patients undergoing hematopoietic stem cell transplantation. Clin Infect Dis 2004; 39:1407–1416. van Burik JA, et al. Clin Infect Dis 2004; 39:1407–16.")
77
Phase III study micafungin vs. fluconazole Overall treatment success
90 80 80.0 70 73.5 60 50 Treatment success (%) 40 30 Overall treatment success with micafungin as antifungal prophylaxis during the post-HSCT neutropenic phase was superior to that of fluconazole (primary efficacy endpoint of overall treatment success: 80% versus 73.5%; p = 0.03). The treatment difference between micafungin and fluconazole was consistent across both allogeneic and autologous transplants. van Burik JA, et al. Micafungin versus fluconazole for prophylaxis against invasive fungal infections during neutropenia in patients undergoing hematopoietic stem cell transplantation. Clin Infect Dis 2004; 39:1407–1416. 20 10 n = 425 457 Micafungin Fluconazole van Burik JA, et al. Clin Infect Dis 2004; 39:1407–16
 Overall treatment success with micafungin as antifungal prophylaxis during the post-HSCT neutropenic phase was superior to that of fluconazole (primary efficacy endpoint of overall treatment success: 80% versus 73.5%; p = 0.03). The treatment difference between micafungin and fluconazole was consistent across both allogeneic and autologous transplants. van Burik JA, et al. Micafungin versus fluconazole for prophylaxis against invasive fungal infections during neutropenia in patients undergoing hematopoietic stem cell transplantation. Clin Infect Dis 2004; 39:1407– n = Micafungin. Fluconazole. van Burik JA, et al. Clin Infect Dis 2004; 39:1407–16.")
78
Is combination of antifungals indicated?

79
Randomized blinded trial of high-dose fluconazole plus placebo vs fluconazole plus AMB as therapy for candidemia in non-neutropenic patients . The combination of fluconazole and AMB was evaluated versus monotherapy with high-dose fluconazole in 219 non-neutropenic patients No difference in survival between the two groups; however, candidemia cleared more rapidly with combination therapy, suggesting potential use in persistent Candida infections Rex JH, et al. Clin Infect Dis 2003; 36:1221-8

80
. Efficacy and Toxicity of Caspofungin in Combination with L-AMB as Primary or Salvage treatment of Invasive Aspergillosis in Patients with Hematologic Malignancies Kontoyiannis DP, et al Cancer 2003; 98: 292-9 48 patients with documented or possible IA The majority (65%) received CAS/L-AMB as salvage therapy for progressive IA despite 7 days of previous L-AMB monotherapy Overall response rate 42% No significant toxicity Factors associated with failure: documented IA, significant steroid use, duration of combination therapy < 14 days Response rate in patients with progressive documented IA 18% Conclusions: The CAS/L-AMB combination is a promising preemptive therapy
 received CAS/L-AMB as salvage therapy for progressive IA despite 7 days of previous L-AMB monotherapy. Overall response rate 42% No significant toxicity. Factors associated with failure: documented IA, significant steroid use, duration of combination therapy < 14 days. Response rate in patients with progressive documented IA 18% Conclusions: The CAS/L-AMB combination is a promising preemptive therapy.")
81
Combination antifungal therapy for invasive aspergillosis
Combination antifungal therapy for invasive aspergillosis Marr KA, et al. Clin Infect Dis. 2004; 39: Salvage therapy with the combination of voriconazole and caspofungin was associated with reduced mortality, compared with voriconazole monotherapy

84
Br J Haematol. 2004; 126:

85
Conclusions Patients at high risk may benefit from empirical therapy
Patients under close surveillance may receive preemptive treatment after early prodromal clues of infection No clear drug of choice, decisions should be individualized Lipid AMB, voriconazole and echinocangins: high risk pts Fluconazole, itraconazole: lower risk pts Limited data point out to combination treatments for selected high risk pts

86
Future issues Should we move from empirical to preemptive therapy based on surrogate markers of early diagnosis of IFIs? Is sequence of antifungals important? Which combinations are more effective?

Similar presentations































>")









