Download presentation
Presentation is loading. Please wait.

1
EBM 2.0 Incorporating values and preferences in clinical decision making Gordon Guyatt CLARITY research group, McMaster University Gordon Guyatt CLARITY research group, McMaster University

2
Patient Values in Clinical Decision-making EBM and the role of patient valuesEBM and the role of patient values patient values and physician valuespatient values and physician values how might we ensure decisions reflect patient values?how might we ensure decisions reflect patient values?

3
Principles of EBM 1. 1.for optimal decision-making, need systematic summary of best evidence 2. 2.hierarchy of evidence 3. 3.evidence is never sufficient for decision-making antibiotics for pneumococcal pneumonia? 95 year old man, severely demented, incontinent, contracted, lives in long-term care facility contracts pneumococcal pneumonia. treat with antibiotics?

4
Values + Preferences Patients perspectives, beliefs, expectations, and goals for health and life. Underlying processes used in considering the benefits, harms, costs, and inconveniences patients will experience with each management option and the resulting preferences for each option.

5
Clinical decision-making 2010 Research evidence Patient values and preferences Clinical state and circumstances Expertise

6
Case 75 y/o female admitted to the ICU with urosepsis 10 days ago. She now requires two inotropes to maintain a mean arterial pressure of 80 mm HG, is ventilator dependent, comatose, and in acute oliguric renal failure. Her APACHE II score is 38, suggesting a 10% chance of survival. Her past history includes long-standing depression, responsive to treatment. She has been walking with a cane due to a chronic deformity from polio.75 y/o female admitted to the ICU with urosepsis 10 days ago. She now requires two inotropes to maintain a mean arterial pressure of 80 mm HG, is ventilator dependent, comatose, and in acute oliguric renal failure. Her APACHE II score is 38, suggesting a 10% chance of survival. Her past history includes long-standing depression, responsive to treatment. She has been walking with a cane due to a chronic deformity from polio.

7
She used to run the family manufacturing business, which involved supervision of 10 people. Until just before admission, she continued to do the bookkeeping for the firm. She is single and lives alone in her own home. There are no known written or verbal advance directives. The patient has an older brother living in the United States, with whom she has not spoken for years, and whose current whereabouts are not known. There are no other living relatives. A few friends visit her in the ICU, but none want to be involved in decisions regarding her medical care.She used to run the family manufacturing business, which involved supervision of 10 people. Until just before admission, she continued to do the bookkeeping for the firm. She is single and lives alone in her own home. There are no known written or verbal advance directives. The patient has an older brother living in the United States, with whom she has not spoken for years, and whose current whereabouts are not known. There are no other living relatives. A few friends visit her in the ICU, but none want to be involved in decisions regarding her medical care.

8
Management strategies 1. D/C inotropes and ventilator but continue comfort measures1. D/C inotropes and ventilator but continue comfort measures 2. D/C inotropes and other maintenance therapy but continue ventilator and other comfort measures2. D/C inotropes and other maintenance therapy but continue ventilator and other comfort measures 3. Continue with current management but add no new therapeutic interventions3. Continue with current management but add no new therapeutic interventions 4. Continue with current management, add further inotropes, change antibiotics, and the like as needed, but do not start dialysis4. Continue with current management, add further inotropes, change antibiotics, and the like as needed, but do not start dialysis 5. Continue with full aggressive management and plan for dialysis if necessary5. Continue with full aggressive management and plan for dialysis if necessary

9
Withdrawal of life support Cook, Guyatt, JAMA. 1995 Cross sectional surveyCross sectional survey Staff from 37 university affiliated hospitals in 8 provincesStaff from 37 university affiliated hospitals in 8 provinces 1361 ICU health care workers completed the survey1361 ICU health care workers completed the survey –149 of 167 ICU attending staff –142 of 173 ICU house staff –1070 of 1455 ICU nurses Overall participation rate 76%Overall participation rate 76%

10
Case Development cases scenarios, variable factorscases scenarios, variable factors –patients age (45 vs 75) –prior cognitive function (highly functional vs alzheimers) –likelihood of surviving current episode (50% vs 10%) –likelihood of long term survival (50% 1yr mortality breast CA vs no comorbidity affecting long term survival) fixed factors in the scenariosfixed factors in the scenarios –socioeconomic status –premorbid physical and emotional function –sex and employment
 –prior cognitive function (highly functional vs alzheimers) –likelihood of surviving current episode (50% vs 10%) –likelihood of long term survival (50% 1yr mortality breast CA vs no comorbidity affecting long term survival) fixed factors in the scenariosfixed factors in the scenarios –socioeconomic status –premorbid physical and emotional function –sex and employment")
12
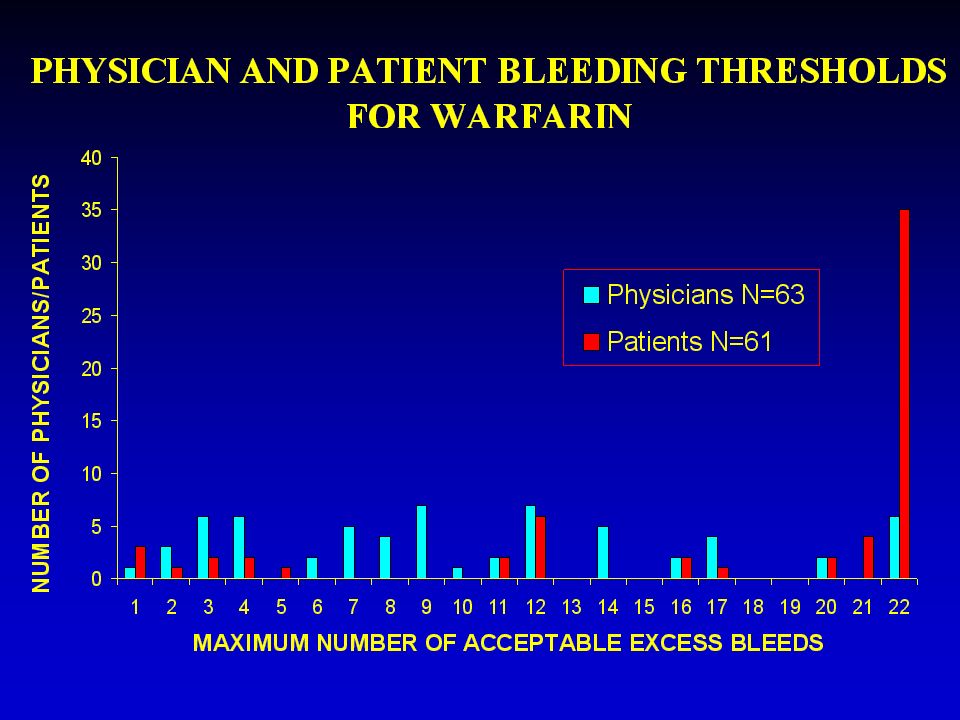
Comparison of patient and physician values to anticoagulate or not to anticoagulate patients with atrial fibrillation: differences between physician and patient perspectivesto anticoagulate or not to anticoagulate patients with atrial fibrillation: differences between physician and patient perspectives –Devereaux PJ et. al., BMJ, 2001 face to face interview of 63 physicians and 61 patientsface to face interview of 63 physicians and 61 patients probability trade-off tool to determine and compare physician and patient thresholds for how much stroke reduction is necessary and how much bleeding risk is acceptable for antithrombotic therapy in atrial fibrillationprobability trade-off tool to determine and compare physician and patient thresholds for how much stroke reduction is necessary and how much bleeding risk is acceptable for antithrombotic therapy in atrial fibrillation

13
Devereaux et. al., 2001 patients with atrial fibrillation at high risk of strokepatients with atrial fibrillation at high risk of stroke warfarin decreases risk at cost of increased gi bleedswarfarin decreases risk at cost of increased gi bleeds without treatment 100 patients will suffer:without treatment 100 patients will suffer: –12 strokes (six major, six minor), 3 serious gi bleeds in 2 years warfarin would decrease strokes in 100 patients to 4 per 2 years (8 fewer strokes, 4 major, minor)warfarin would decrease strokes in 100 patients to 4 per 2 years (8 fewer strokes, 4 major, minor) how many bleeds would you accept in 100 patients over two years, and still be willing to administer/take warfarin?how many bleeds would you accept in 100 patients over two years, and still be willing to administer/take warfarin?
, 3 serious gi bleeds in 2 years warfarin would decrease strokes in 100 patients to 4 per 2 years (8 fewer strokes, 4 major, minor)warfarin would decrease strokes in 100 patients to 4 per 2 years (8 fewer strokes, 4 major, minor) how many bleeds would you accept in 100 patients over two years, and still be willing to administer/take warfarin how many bleeds would you accept in 100 patients over two years, and still be willing to administer/take warfarin .")
14
STROKES CAN BE MINOR OR MAJOR IN SEVERITY MINOR STROKE MAJOR STROKE PHYSICAL SYMPTOMS MENTAL SYMPTOMS PAIN RECOVERY FURTHER RISK IF YOU HAVE A STROKE, YOUR CHANCE OF HAVING A MINOR OR MAJOR STROKE ARE EQUAL - You suddenly cannot move or feel one arm and one leg - You are unable to fully understand what is being said to you - You have difficulty expressing yourself - You feel no physical pain -You are admitted to hospital -Your weakness, numbness and problem with understanding improve but you still feel slightly weak or numb in one arm and one leg -You are able to do almost all the activities you previously did before the stroke -You can function independently - You have an increased risk of having more strokes - You suddenly are dizzy and blackout - You are unable to move one arm and one leg - You cannot swallow or control bladder and bowel - You are unable to understand what is being said - You are unable to talk - You feel no physical pain -You are admitted to hospital -You cannot dress -The nurse feeds you -You cannot walk -After 1 month with physiotherapy, you are able to wiggle your toes and lift your arm off the bed -You remain this way for the rest of your life - Another illness will likely cause your death

15
SEVERE BLEEDING AN EXAMPLE OF THIS IS A STOMACH BLEED PHYSICAL TREATMENT RECOVERY - You feel unwell for two days then suddenly you vomit blood -You are admitted to hospital -You stop taking warfarin -A doctor puts a tube down your throat to see where you are bleeding from -You receive sedation to ease the discomfort of the test -You do not need an operation -You receive blood transfusions to replace the blood you lost -You stay in hospital one week -You feel well at the end of your hospital stay -You need to take pills for the next six months to prevent further bleeding -You do not take warfarin any more -After that you are back to normal

16
Devereaux et. al., 2001 patients with to atrial fibrillation at high risk of strokepatients with to atrial fibrillation at high risk of stroke warfarin decreases risk at cost of increased gi bleedswarfarin decreases risk at cost of increased gi bleeds without treatment 100 patients will suffer:without treatment 100 patients will suffer: –12 strokes (six major, six minor), 3 serious gi bleeds in 2 years warfarin would decrease strokes in 100 patients to 4 per 2 years (8 fewer strokes, 4 major, minor)warfarin would decrease strokes in 100 patients to 4 per 2 years (8 fewer strokes, 4 major, minor) how many bleeds would you accept in 100 patients over a year, and still be willing to administer/take warfarin?how many bleeds would you accept in 100 patients over a year, and still be willing to administer/take warfarin?
, 3 serious gi bleeds in 2 years warfarin would decrease strokes in 100 patients to 4 per 2 years (8 fewer strokes, 4 major, minor)warfarin would decrease strokes in 100 patients to 4 per 2 years (8 fewer strokes, 4 major, minor) how many bleeds would you accept in 100 patients over a year, and still be willing to administer/take warfarin how many bleeds would you accept in 100 patients over a year, and still be willing to administer/take warfarin .")
18
Is this real? retrospective review through record linkage across population based databases in Canadaretrospective review through record linkage across population based databases in Canada 530 MDs cared for:530 MDs cared for: –3120 afib patients with warfarin bleed (intracraneal or GI) –for a patient with afib 90 days prior to bleed –for a patient with afib 90 days after the event –(some of these MDs also cared for patients up 1 y post) –90% of patients were at high risk for afib-related stroke how likely are patients seen after an afib patient bled while on warfarin to receive a warfarin prescription (compared to those seen 90 days before the bleed)?how likely are patients seen after an afib patient bled while on warfarin to receive a warfarin prescription (compared to those seen 90 days before the bleed)?
 –for a patient with afib 90 days prior to bleed –for a patient with afib 90 days after the event –(some of these MDs also cared for patients up 1 y post) –90% of patients were at high risk for afib-related stroke how likely are patients seen after an afib patient bled while on warfarin to receive a warfarin prescription (compared to those seen 90 days before the bleed) how likely are patients seen after an afib patient bled while on warfarin to receive a warfarin prescription (compared to those seen 90 days before the bleed) .")
19
Likelihood of warfarin prescription 1.0 0.79 (0.62-1.00) 0.60 (0.46-0.69) 0.61 (0.46-0.81) 0.72 (0.54-0.97) 1.00 90 d prior 0-90 d post 91-180 d post 181-270 d post 271-360 d post Odds ratio (95% CI) Less warfarin after bleeding Days relative to bleed
 0.60 ( ) 0.61 ( ) 0.72 ( ) d prior 0-90 d post d post d post d post Odds ratio (95% CI) Less warfarin after bleeding Days relative to bleed")
20
Conclusions average patient preferences/values differ from average physician preferencesaverage patient preferences/values differ from average physician preferences –if physician values determine the decision, patients wont get what they want physician values/preferences differphysician values/preferences differ –if physician preferences determine decisions, then your treatment depends on your physician patient values/preferences differpatient values/preferences differ –if use average patient preferences, many patients wont get what they want

21
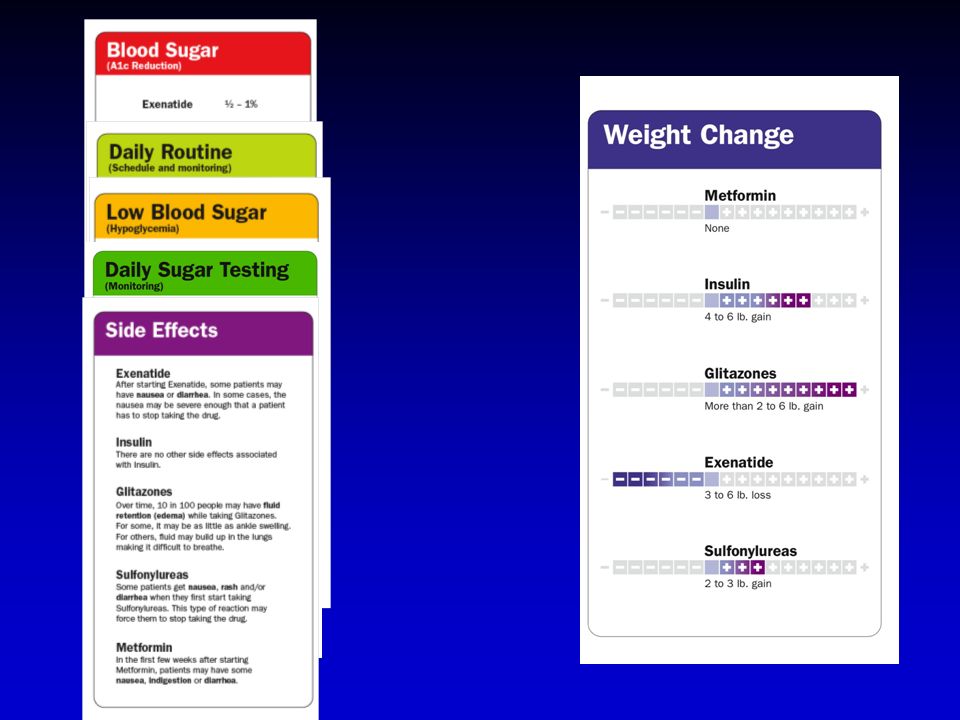
Giving patients what they want traditional methodstraditional methods decision aidsdecision aids –decision boards –decision booklets –flip charts –videos –audiotapes –computerized decision instruments

28
Do decision aids work? systematic review of 34 RCTs compared to usual care, decision aids: – –increased patient participation in decision making (RR 1.4, 95% CI: 1.0-2.3) – –improved patient knowledge (19, 95% CI 13-24, points out of 100 in knowledge surveys) – –reduced decisional conflict (9.1 of 100, 95%CI: 6-12)
 – –improved patient knowledge (19, 95% CI 13-24, points out of 100 in knowledge surveys) – –reduced decisional conflict (9.1 of 100, 95%CI: 6-12).")
29
Conclusions health care provider and patient values influence decision making and the two are not always the samehealth care provider and patient values influence decision making and the two are not always the same decision aidsdecision aids –lead to more certain and informed decisions –increase knowledge about treatment options and outcomes –in some instances lead to decreased preferences for interventions, therapies, and screening

Similar presentations






 The Inaugural Conference.>")


















