Download presentation
Presentation is loading. Please wait.

1
ACUTE CORONARY SYNDROME Jarrod D. Frizzell, MD, MS Fellow, Cardiovascular Medicine July 10, 2014

2
A Case 37yoM awoke with chest pressure Radiating to left shoulder Still present after 1h. Tachy, “JVD to ears”, lungs clear Just diagnosed with DM last night iStat Tn: 0

6
Outline Definitions ACS MI STEMI NSTEMI UA Pearls

7
Acute Coronary Syndrome

9
Syndrome Chest pain (angina?) Most common: upper body discomfort & SOB Diaphoresis Nausea/vomiting Dizziness Isolated atypical sx are uncommon (women, elderly, DM) Entire picture must be set in clinical context ECG or isolated Tn alone does not make it
 Most common: upper body discomfort & SOB Diaphoresis Nausea/vomiting Dizziness Isolated atypical sx are uncommon (women, elderly, DM) Entire picture must be set in clinical context ECG or isolated Tn alone does not make it")
10
Acute Coronary Syndrome Goldacre, Acad Emer Med 2003

11
Acute Coronary Syndrome ACS typically implies “type I event” Divided into: STEMI NSTEMI UA

12
Braunwald, AJRCCM 2012

13
Types of MI

14
Universal Definition of MI Detection of rise and/or fall of cardiac biomarkers with at least 1 value above the 99 th %ile reference limit and with at least 1 of the following Sx of ischemia New or presumed new significant ST-T changes or LBBB Development of pathologic Q waves Imaging evidence of new loss of viable myocardium or new WMA Identification of an intracoronary thrombus (cath or autopsy) Circulation 2012
 Circulation 2012")
15
Features Braunwald, 9 th ed.

16
ECG

17
STEMI ST elevations—measured at the J point V2-V3—age/gender dependent Women: 1.5mm Men ≥40: 2mm Men <40: 2.5mm 1mm in all other leads “Injury pattern”

18
STEMI ECG.utah.edu

19
STE Ecginterpretation.blogspot.com

20
ECG

24
STEMI vs everything else Why? Very specific for transmural ischemia (diagnosis & location) “Time is muscle”
 Time is muscle .")
25
THE Graph Gersh, JAMA 2005

26
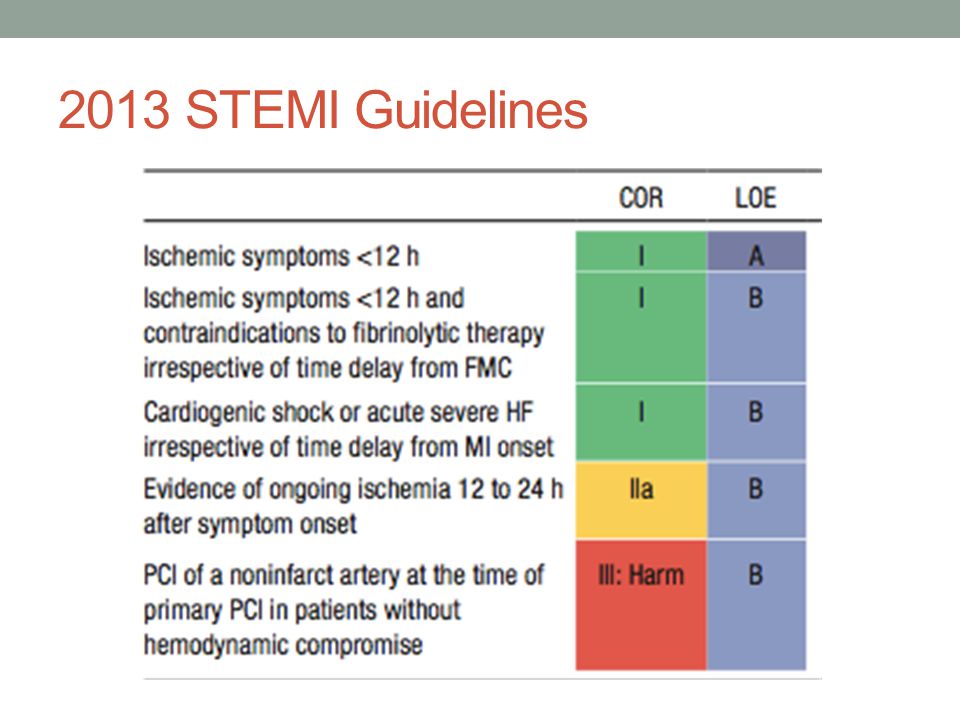
2013 STEMI Guidelines

28
STEMI Meds—Before Cath Anti-platelet load ASA Thienopyridine (clopidogrel) Anticoagulation Heparin/LMWH Bivalirudin (if PCI—started in cath lab) Not fonda IIb/IIIa fallen out of favor except special circumstances Pain relief NTG Morphine? If need beyond, call fellow (for boards: CCB, BB)
.")
29
Back to ACS

30
NSTEMI Still presentation of ACS, but not STE Elevated Tn TIMI Score

31
Braunwald, AJRCCM 2012

32
NSTEMI

33
If low risk, probably go with noninvasive imaging Dob echo Dipy/cardiolite Initial meds overall similar to STEMI ASA/clopidogrel Heparin/LMWH Time is less pressing Urgent (<120min) Early invasive (<72h) Conservative (not cath)
 Early invasive (<72h) Conservative (not cath)")
34
Unstable Angina Definition CP that occurs at rest or with minimal exertion, lasts >20min Onset within past month Crescendo pattern A dying breed? Broadly speaking, treat like NSTEMI

35
“Routine Medical Therapy” Within 24h: Beta-blocker ACEI High-intensity statin Also get TTE

36
When to call? Whenever you feel uncomfortable Not the resident’s job to “rule out STEMI” on ECG You will only regret not calling If cannot get CP-free

37
Miscellany Elevated Tn—when to heparinize? DAPT—duration DES: 1y BMS: at least 1mo, up to 1y ACS but no intervention—1 year “No breakfast on 7S” (NPO for tests) “No coffee at the VA” (NPO for nuc, caffeine interferes)
 No coffee at the VA (NPO for nuc, caffeine interferes).")
38
Boards Odds & Ends RV Infarct Inferior STE (get right-sided ECG) +JVD but clear lungs (Borderline) Hypotensive fluids Avoid NTG STEMI is not only cause of STE If STEMI at non-PCI OSH: Transfer if PCI within 120min Lytics if transfer outside window Idioventricular rhythm post reperfusion Looks like VT, but slower No additional therapy
 +JVD but clear lungs (Borderline) Hypotensive fluids Avoid NTG STEMI is not only cause of STE If STEMI at non-PCI OSH: Transfer if PCI within 120min Lytics if transfer outside window Idioventricular rhythm post reperfusion Looks like VT, but slower No additional therapy")
Similar presentations









>")











 in leads V2-V4. Upper arrow points at the positive deflection, negative.>")

 Definition of ACS Signs and symptoms of ACS Gender and age related difference in ACS Pathophysiology.>")
 CAD is most common form of heart disease and causes premature death. In UK, 1 in 3 men and.>")

