Download presentation
Presentation is loading. Please wait.

1
Specifying clinical IT requirements for pathways: a national perspective Dr Mark Dancy Consultant Cardiologist National Clinical Lead CHD Collaborative

2
Potential benefits from NPfIT Readily available information Patients Clinicians looking after them Ease of communication Combined care Audit Health economics & Public Health

3
Current position Numerous systems All different Software Field definitions Architectures Not designed to communicate Need paper

4
Current position Many databases designed for audit Not designed around patient pathway ‘Minimum dataset’ Implies majority of mandatory fields Not suitable for EPR High cost of data gathering – audit clerks Integrated care pathways Within hospitals mostly paper-based Within primary care – templates

5
Datasets: different according to purpose Clinical processes history, exam, tests, diagnosis, treatment Audit and clinical governance local and national - NSF targets Information for patients general and personal Public health Service planning: demand and capacity Finance

6
Clinical datasets (EPR) Needs a lot of data – medicine is complex Choice between free text and defined data items (auditable) Needs a lot of data items Many/most will not be mandatory How much of the requirements for other uses will be met by a good clinical dataset?
 Needs a lot of data – medicine is complex Choice between free text and defined data items (auditable) Needs a lot of data items Many/most will not be mandatory How much of the requirements for other uses will be met by a good clinical dataset")
7
The ideal system design for clinical input Intuitive, fast Follows predicted workflows Accommodates the majority of clinical needs with minimal need for free text Data entered at point of care Supports workforce developments (PwSI) Platform independent Organisation independent
 Platform independent Organisation independent")
8
Potentially difficult areas Inpatient care Complex Changing differential diagnoses Changing firms Logistics of the bedside Multiple pathologies Systems often arranged around single diagnosis Best test-bed is single disease managed out of hospital

9
RAPCP Pilot Dataset development Clinical systems manufacturers Local developmentNational system Provisional national dataset Functional specification Pilot sites Maximum choice for end-users Understanding workflows

10
Disease management system project: DMSP Common principles Based on patient pathway Translated into workflows Platform and organisation independent Electronic communications Three conditions Heart Failure Breast Cancer Diabetes

11
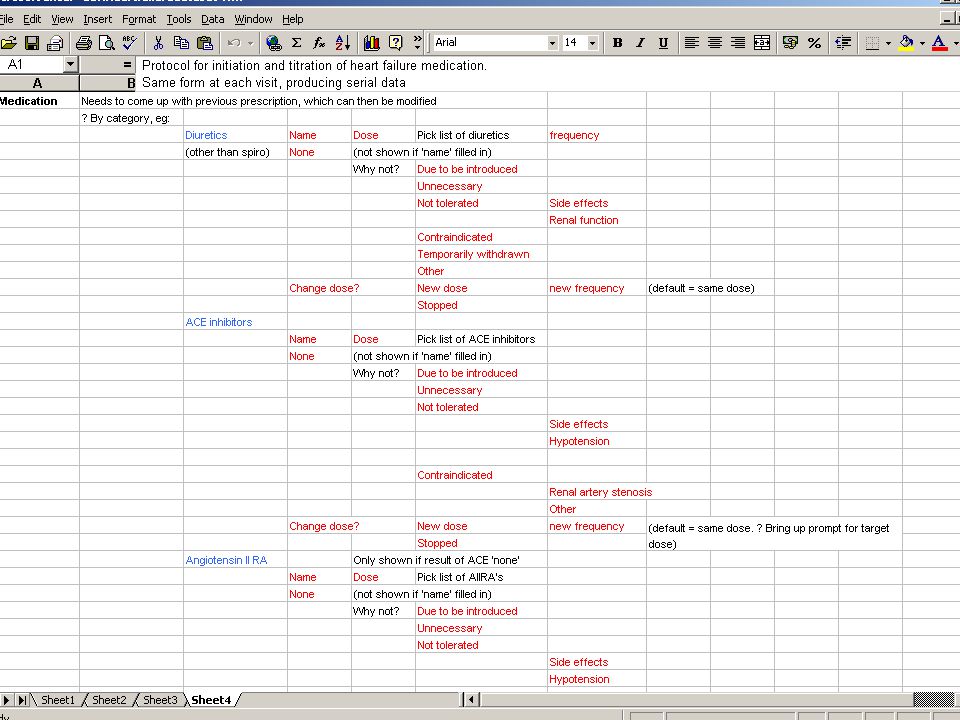
Referral proforma Call/recall systems for chronic disease management Placed on heart failure register Stabilisation Initiation of Beta blocker &/ spironolactone Up-titration of drugs Initiation of treatment with ACE and diuretics Requires further investigations Preliminary conclusions ? LVSD Heart failure clinic Primary care Either Secondary care Further treatment LV systolic dysfunction Transfer of referral data and e-booking Summary of conclusions from heart failure clinic Single message to put on register a* Sheet 1 Sheet 2 Sheet 4 Sheet 3 a*: if continuing care to be in acute trust initiates appropriate arrangements. If to be primary care initiates request message to 1y care to book patient into their clinic IP admission Yes No Discovered to have heart failure in OPD Heart failure suspected

15
Where to go from here? DMSP is proof of concept Direct communication between local systems may be unnecessary in NPfIT (via spine) Recognition that the interface between the clinician and the system is the most important element of design Extend into other more difficult areas Major task in ‘information out’
 Recognition that the interface between the clinician and the system is the most important element of design Extend into other more difficult areas Major task in ‘information out’.")
Similar presentations






 BOSSnet Victorian Account Manager>")

 dataset.>")











 Via Conservatorio, 7. 20122 Milano, Italy The P-medicine project:>")
