Download presentation
Presentation is loading. Please wait.

1
Ali Alshehri, MD DHC, Saudi Aramco Sept, 29th, 2011
TEE and Aortic valve Ali Alshehri, MD DHC, Saudi Aramco Sept, 29th, 2011

2
Q #1 Gorlin formula has the following limitations except:
in AR, the area may be falsely elevated CO in Afib must be averaged on few beats peak – peak gradient is required SEP must be calculated

3
Q #2 All are true about planimetry for AV except
ME SAX view is preferred Correlates well with cath derived AVA Depends on adequate CO Significant calcifications decreases the accuracy

4
Q# 3 The following is true regarding pressure g across AV
Doppler derived MIG approximates catheter MIG Peak to peak gradient is the highest gradient Doppler MIG approximates cath PPG All true

5
Movements of the probe Turning: turning the shaft of the probe to the left or right. Rotating: rotating the transducer forward (towards 180°) or backward (towards 0°). Withdrawing and advancing: moving the probe further out of, or further into, the oesophagus. Anteflexing and retroflexing: moving the tip of the probe forwards or backwards.
 or backward (towards 0°). Withdrawing and advancing: moving the probe further out of, or further into, the oesophagus. Anteflexing and retroflexing: moving the tip of the probe forwards or backwards.")
6
Bicuspid AV

7
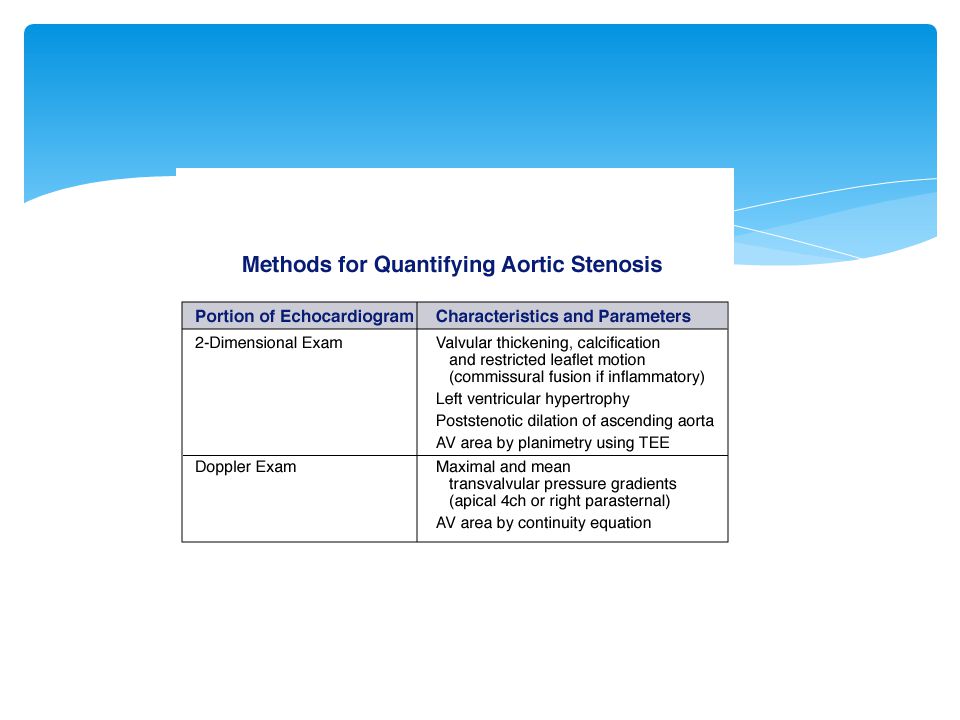
Normal Aortic valve area 2.6-3.5 cm2.
Severe AS defined as: Area <1.0cm2 Mean gradient >40 mmHg Peak velocity >4.0 m/s

8
Subaortic membrane

10
Bicuspid AV

13
Ascending aortic aneurysm

14
TEE views to assess AV ME short axis view ME long axis view
ME 5 chamber view ME short axis view ME long axis view TG long axis view DTG LAX view

15
ME 5 chamber view: Is part of the starting 4 chamber view with small withdrawal of the probe to show the aortic leaflets. Not used commonly because of better other views.

16
ME 5 chamber view

17
Quadricuspid AV

18
ME short axis view Image setting: Angle 25- 45 degrees Sector depth :10-12 cm Probe adjustment: Neutral Primary use: AS, valve morphology Required structures: 3 valve leaflets, commissures, coaptation point

19
ME short axis view

20
ME long axis view Image setting: Angle 115- 130 degrees Sector depth: 8-10 cm Probe adjustment: neutral Primary use: Aortic valve pathology, ascending aorta and root, LVOT pathology Required structures: LVOT (>1cm prox to AV) ascending Ao(>1cm distal to STJ)
 ascending Ao(>1cm distal to STJ)")
21
Aortic dissection

22
ME long axis view

23
TG long axis view Image setting: Angle degrees sector depth 12 cm probe adjustment: neutral- leftward Primary use: Doppler assessment of AV, LVEF AV and VOT at 4 o’clock Technique: from TG 2 chamber , the probe is rotated to 120 degrees with Lt ward rotation of the probe

24
TG long axis view

25
DTG LAX view Image setting: Angle 0 degrees Sector depth : 16cm Probe adjustment: Anteflexed Primary use: AV morphology, LVOT Doppler assessment of AV Technique: probe advanced to LV apex, anteflexed and slightly withdrawn with rotation of the probe to the Lt.

26
DTG LAX view

27
Fibroelastoma

28
Assessment of AS 2D assessment of valve morphology,
commissures, coaptation point. Doppler interrogation( Bernoulli equation) AVA ( continuity equation) Planimetry Dimensionless Index
 AVA ( continuity equation) Planimetry. Dimensionless Index.")
29
Planimetry All planimetric techniques are limited because of an inability to determine whether the actual minimal orifice is being imaged or whether the plain chosen for measurement is at an angle o the true minimal orifice.

30
Planimetry of AV

31
Planimetry Technique: 1- all 3 leaflets should be in view 2- use colour doppler with minimal gain to adjust depth and angle 3- gain setting to minimum to show orifice 4- use tracing caliber of machine to trace orifice Aim: get the narrowest orifice reduce the blooming artifact

32
Planimetry The accuracy of planimetry has been assessed by comparing it to the “ gold standard” reference used in cath lab, The Gorlin equation: AVA = CO/ 44.3(SEP)(HR) MG( square root) so AVA is dependent on CO and mean gradient
(HR) MG( square root) so AVA is dependent on CO and mean gradient")
33
Planimetry TEE is considered superior to TTE because of it’s higher resolution in measuring the AV orifice more accurately. Stoddard, reported good correlation with TTE and superior correlation with cath .(AHJ 1991)
")
34
Hoffman, showed excellent correlation of TEE with Gorlin formula determined area.(JACC, 1993) Planimetry is not affected by CO changes and is considered by some more accurate in high and low CO.
 Planimetry is not affected by CO changes and is considered by some more accurate in high and low CO.")
35
Hoffman et al, JACC 1993

36
This is mostly seen in heavily calcified valves

37
Doppler gradient Peak gradient = 4(Vmax)2( peak aortic velocity)
Mean gradient= 2.4 (Vmax)2 Excellent correlation with cath measured MG Echo measures peak instantaneous gradient Cath measures peak to peak gradient Use modified Bernoulli equation in AI or high CO : peak gradient = 4(V max) 2-(LVOT V)2
2. Excellent correlation with cath measured MG. Echo measures peak instantaneous gradient. Cath measures peak to peak gradient. Use modified Bernoulli equation in AI or high CO : peak gradient = 4(V max) 2-(LVOT V)2.")
39
Continuity equation AVA= TVI LVOT X AREALVOT/ TVI AV
LVOT measured endo-endo at mid systole at insertion point of the leaflets. Usually done in ME ling axis view. LVOT area 3.14X r2= 3.14X(D/2)2 Measured with PW at measurement site “Envelope in envelope” method also used
2. Measured with PW at measurement site. Envelope in envelope method also used.")
40
Continuity equation Unless a clearly defined velocity envelope can be seen, no quantitative estimate of severity should be done.

41
Dimensionless Index DI= LVOT TVI/ AV TVI Severe AS< 0.25
Helpful when LVOT measurement is in doubt( disproportionately high or low area to the measured gradient) For follow up of prosthetic aortic valve
 For follow up of prosthetic aortic valve.")
43
Case presentation History: Mr K, 56y old male, chemical engineer.
Newly diagnosed diabetes Seen in ophthalmology clinic for decreased Rt eye vision for 1 week and diagnosed with retinal He Admitted 1 week later with fatigability X1month, fever and intermittent memory lapses noted by wife. No recent dental work.

44
Exam: BP 140/50. PR 90/min, temp 39.0C No peripheral sings if IE Grade II diastolic murmur at Rt upper chest

45
Labs: WBC 20.0, Hb 11.8, plat 328,000 ESR 80, CRP 14, crea 1.2 ECG: normal CXR: mild cardiomegaly, no congestion B culture: Sterptococcus aginiosus

46
Further W/U TTE TEE CT chest: 5.1 cm aortic root and ascending aorta.

47
TTE: Ejection Fraction = 50-55%. Left ventricular systolic function is normal. There is mild mitral regurgitation. There is a moderate size vegetation or mass on the aortic valve. Aortic valve is thickened looks morphologically Bicuspid and prolapsing in diastole. Moderate to sever aortic regurgitation. There is an eccentric jet of aortic insufficiency directed against the anterior mitral leaflet. The right ventricular systolic function is normal. The left ventricle is severely dilated. Possible mitral vegetation also seen.

48
TEE: TEE confirms endocarditis on congenital bicuspid aortic valve The aortic valve is bicuspid. There is a large vegetation or mass o the aortic valve. Moderate aortic regurgitation. Volume overloaded LV due to aortic regurgitation .Vegetation length is approximately 16 mm. There i also significant thickening of the large non coronary cusp which could be a vegetation. No abscess is seen. Possible mitral vegetations also.

49
CT chest: 5.1 cm aortic root and ascending aorta.

60
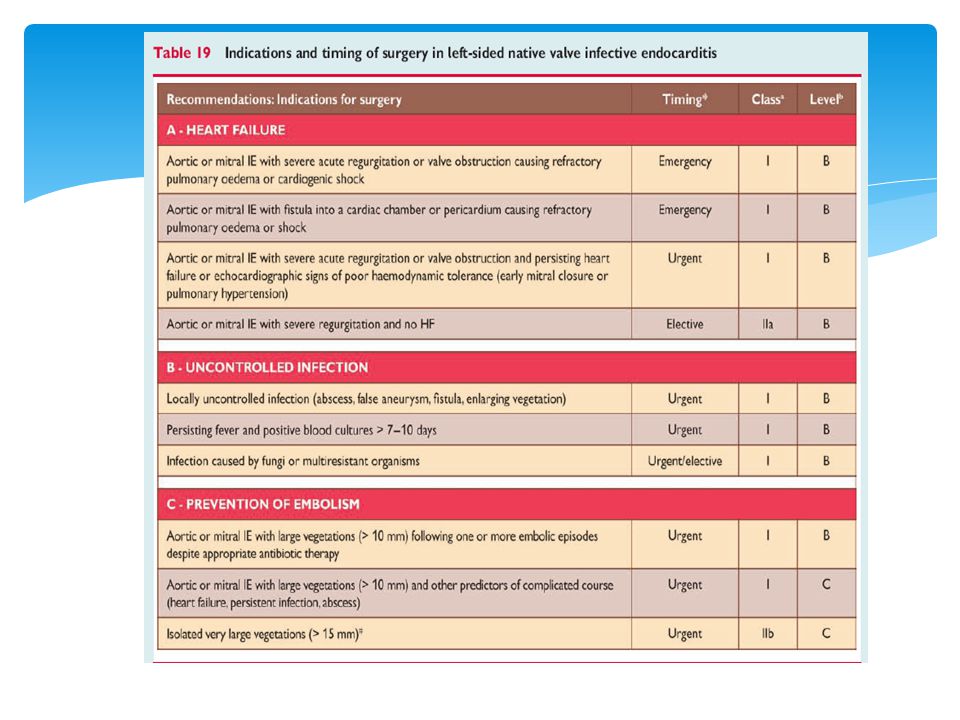
Back to our patient Patient became a febrile. No heart failure. Memory lapses improved. Referred to KFSH for surgery after completing 3 weeks of IV antibiotics. At surgery, both AV and MV infected with perforation. No abscess seen. 29mm carbomedics valved conduit+ MVR done Completed another 3 weeks of IV antibiotics.

61
Thank you

Similar presentations



















. - a spherical occluder is contained by metal.>")









