Download presentation
Presentation is loading. Please wait.

1
Connie Tsao, MD Noninvasive/Echo Conference July 29, 2009

2
Definition Discrete narrowing of the thoracic aorta Distal to left subclavian artery ○ At ductus arteriosis Proximal to left subclavian artery Abdominal aorta Rarely long segment or tubular hypoplasia

3
Epidemiology 6-8% of all congenital heart defects Male: Female 2-5:1 Sporadic; rare familial Turner Syndrome: XO Bicuspid aortic valve 30-40% incidence LVOT obstruction malformations Familial occurrence VSD PDA Aortic stenosis Mitral stenosis Intracerebral aneurysm Associations

4
Pathogenesis Congenital Most common Acquired Inflammation/Arteritis, eg, Takayasu ○ Mid-thoracic, abdominal aorta Severe atherosclerosis

5
Pathogenesis/Pathology Mechanism unknown Genetic defects? Intrauterine defects, eg impaired blood flow altered endothelial development? Medial thickening + intimal hyperplasia posterolateral ridge encircling lumen Surgical specimens: ↑ collagen ↓ smooth muscle mass in pre vs poststenotic areas Cystic medial necrosis: disarray of elastic tissue

6
Being born can be a problem In utero: High PVR, low SVR 90% cardiac output: PDA descending ao At birth: ↑ SVR ↓ PVR PFO and PDA closure CO through ascending aorta

7
Clinical Manifestations Neonates Absent/delayed femoral pulse Differential cyanosis if severe and large PDA R L shunt Heart failure/ shock in first day of life Children Delayed diagnosis 2/2 mild coarctation Chest pain with exercise, cold extremities, claudication Adults Hypertension Autoregulatory vasodilation/constriction maintains blood regional flow Claudication

8
Differential Blood Pressure Classic findings Hypertension in upper extremities Decreased/ delayed femoral pulse Low blood pressure in lower extremities Etiology of hypertension Mechanical obstruction ↑ renin secretion volume expansion

9
Neurologic Comorbitities Increased frequency of intracranial aneurysms Prospective study of 100 pts: 10% aneurysms Usually 10-30 years of age Persistence after normalization of BP Dilation of collateral spinal arteries compress spinal cord Connolly HM et al, Mayo Clin Proc 2003

10
Cardiac Exam Often normal without co-existing defects Continuous murmur if large collateral vessels Systolic ejection click and/or murmur if bicuspid aortic valve Short midsystolic murmur from flow across coarctation itself

11
Prenatal Diagnosis 16-18 weeks of gestation Helpful identifiers: Long segment Small LV Small mitral annulus Dilated RV Flow through ductus difficult to detect coarctation

12
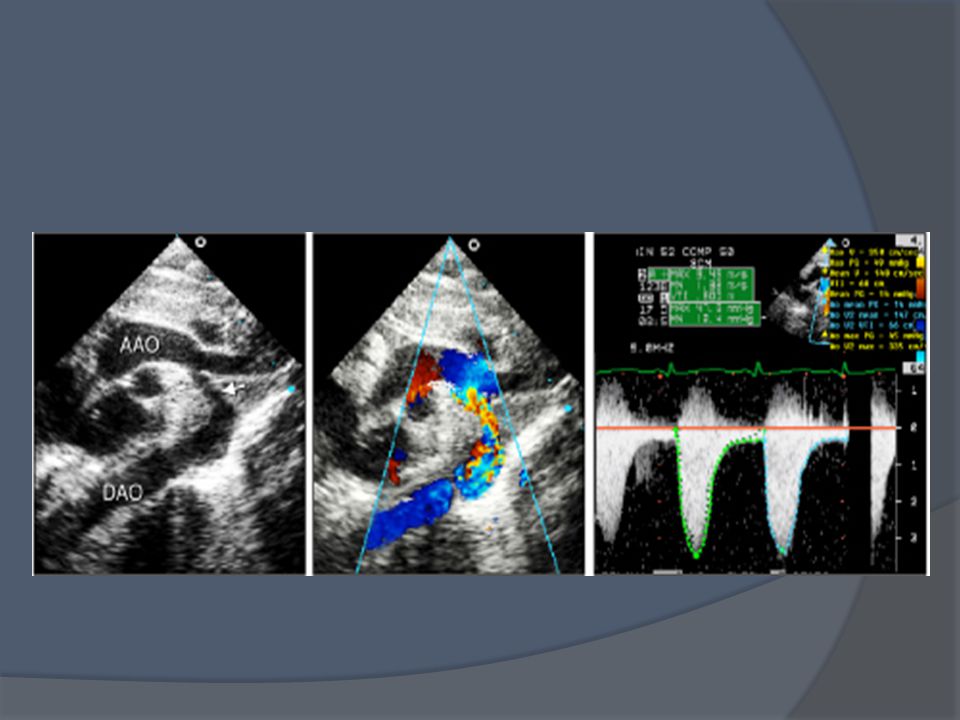
Echocardiography High parasternal, suprasternal long axis Shelf within lumen of thoracic aorta Color and pulse wave doppler to locate area Continuous wave doppler to detect maximum flow velocity

13
Echo Characteristics Low amplitude continuous doppler flow in descending aorta below coarctation Persistence of flow in diastole Otto, CM, Textbook of Clinical Echocardiography, 3 rd Ed

14
Predictors of Fetal Coarctation 44 fetuses with suspected coarct Mean 24 wks gestation Isthmus Z score <-2 Isthmus to ductal ratio <0.74 Disturbance in doppler flow at isthmus Matsui H, et al, Circulation 2008

15
Fetal Diagnosis A: 27 week fetus B: 38 week postmortum C: Continuous low velocity doppler at isthmus Matsui H et al, Circ 2008

16
Normal Adult Aortic Arch

18
27 year old man with coarctation s/p balloon angioplasty in 1996

21
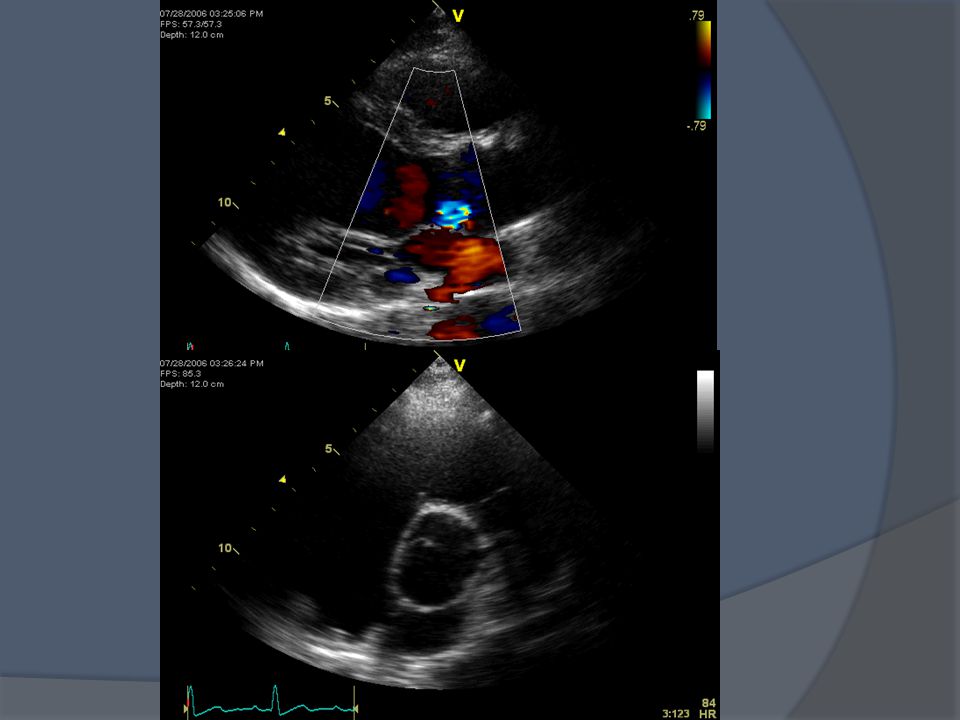
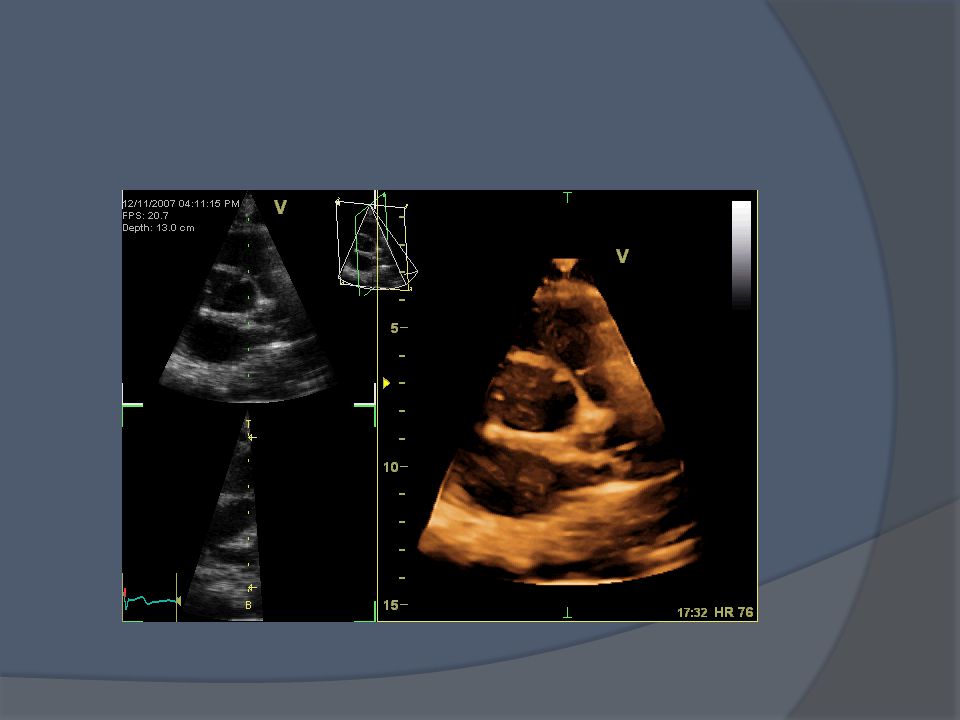
37 year old woman with history of coarctation s/p surgery as child

25
Other diagnostic modalities ECG Varies with severity RVH CXR MRI

26
CXR Infants with severe disease: cardiomegaly, heart failure Notching posterior ribs: erosion by collaterals “3” Sign: Indentation of aortic wall with pre and poststenotic dilatation

27
MRI

32
Cardiac Catheterization Fawzy ME et al, JACC 2004

33
Clinical Management Neonate in heart failure: Medial rx prior to surgery: Prostaglandin E1 PDA open, inotropic agents Indications for intervention: Hypertension Heart failure Peak gradient >20 mm Hg Collateral circulation on MRI

34
Surgical Options Resection with end- to-end anastamosis +/- graft material Developed in 1945 Especially in older children, adults Gross et al, Surgery 1945 Omeje IC et al, Images Paediatr Cardiol 2004

35
Subclavian flap aortoplasty Long-segment of coarctation

36
Prothetic patch aortoplasty Associated with aortic aneurysm/ rupture

37
At Surgery

38
Surgical Outcomes Mortality rare Postoperative paradoxical hypertension, left recurrent laryngeal nerve paralysis, phrenic nerve injury, subclavian steal Re-coarctation in 5-14% patients Young infants Inadequate aortic wall growth

39
Balloon Angioplasty (BA) Preferred for children, adults Native coarctation or after surgery Not infants <6 mos Initial success in 80-90% Gradient ≤ 20 mm Hg Rao PS,J Pediatrics 1987; Beekman RH et al, JACC 1987
 Preferred for children, adults Native coarctation or after surgery Not infants <6 mos Initial success in 80-90% Gradient ≤ 20 mm Hg Rao PS,J Pediatrics 1987; Beekman RH et al, JACC 1987")
40
Rao PS et al, Brit Heart J 1986

41
BA- Potential Complications 20% (up to 35%) incidence residual pressure >20 mm Hg Up to 25% incidence recoarctation 1-3% dissection, rupture 2-8% incidence aneurysm in f/u up to 5 yrs Up to 15% femoral artery complications Rao PS et al, JACC 1996; Fletcher SE et al, JACC 1995; Tynan M et al, Am J Cardiol 1990; Saba SE et al, J Invasive Cardiol 2000
 incidence residual pressure >20 mm Hg Up to 25% incidence recoarctation 1-3% dissection, rupture 2-8% incidence aneurysm in f/u up to 5 yrs Up to 15% femoral artery complications Rao PS et al, JACC 1996; Fletcher SE et al, JACC 1995; Tynan M et al, Am J Cardiol 1990; Saba SE et al, J Invasive Cardiol 2000")
42
54 patients (40 male), 22±7 (15-55) years Indication: Discrete coarctation ± pressure >20 mm Hg, + systemic hypertension unresponsive to medical rx Successful procedure in 49 (93%) Surgery in 3 pts: dissection, aneurysm, persistent gradient 2 lost to f/u 49 followed: Repeat cath in 1 year; yearly BP, ECG, CXR, echo, MRI Median 10.2 (9.1 ± 4.4 years) up to 15.3 years JACC 2004
, 22±7 (15-55) years Indication: Discrete coarctation ± pressure >20 mm Hg, + systemic hypertension unresponsive to medical rx Successful procedure in 49 (93%) Surgery in 3 pts: dissection, aneurysm, persistent gradient 2 lost to f/u 49 followed: Repeat cath in 1 year; yearly BP, ECG, CXR, echo, MRI Median 10.2 (9.1 ± 4.4 years) up to 15.3 years JACC 2004")
43
Results BP normal without medications in 31 pts (63%) Aneurysm in 4 pts at 1 year f/u (7.8%) Prior studies 2-6% occurrence
 Aneurysm in 4 pts at 1 year f/u (7.8%) Prior studies 2-6% occurrence")
44
Fawzy ME et al, JACC 2004

45
Angioplasty vs. Surgery 36 children (3-10 years) 20 BA/ 16 surgery Both 86%↓ peak systolic pressure gradient Similar frequency of bleeding; surgery with 2 neurologic events (paraplegia, vocal cord paralysis) Angioplasty 20% incidence aneurysm Restenosis after angioplasty 25% (vs 6%) Associated with isthmus/desc ao <0.65 and post- procedure pressure ≥12 mm Hg Shaddy RE et al, Circ 1993
 20 BA/ 16 surgery Both 86%↓ peak systolic pressure gradient Similar frequency of bleeding; surgery with 2 neurologic events (paraplegia, vocal cord paralysis) Angioplasty 20% incidence aneurysm Restenosis after angioplasty 25% (vs 6%) Associated with isthmus/desc ao <0.65 and post- procedure pressure ≥12 mm Hg Shaddy RE et al, Circ")
46
Angioplasty vs. Surgery, cont’d Extended follow up (10.6±4.7 years BA and 11.3±3.7 years surgery) 11 BA, 10 surgery No difference in resting BP, exercise performance, MRI dimensions of arch, need for repeat intervention BA: 35% incidence of aneurysm (none for surgery) Some forming after 5 years Cowley CG, et al, Circ 2005
 11 BA, 10 surgery No difference in resting BP, exercise performance, MRI dimensions of arch, need for repeat intervention BA: 35% incidence of aneurysm (none for surgery) Some forming after 5 years Cowley CG, et al, Circ")
47
Angioplasty vs. Surgery, cont’d Retrospective review of 4 Canadian tertiary centers, 12±10 years 50 BA (19 stent) vs. 30 surgery F/u 38 months Similar reduction in peak systolic gradient Surgery: procedure-related complications BA: 32% reintervention (none in surgery group) Aneurysm in 24% (vs. none in surgery) Rodes-Cabau J et al, Am Heart J 2007
 vs. 30 surgery F/u 38 months Similar reduction in peak systolic gradient Surgery: procedure-related complications BA: 32% reintervention (none in surgery group) Aneurysm in 24% (vs. none in surgery) Rodes-Cabau J et al, Am Heart J")
48
Stent Placement Initially for those with residual gradient after BA ↑ lumen diameter ↓ residual gradient Dilate stent with growth of aorta Not for pts <25 kg Ebeid MR et al, JACC 1997Ledesma M et al, Am J Cardiol 2001

49
Stent Placement Retrospective review of 71 consecutive pts (44M, mean 22±6 years), 52 native coarctation 74 stents implanted Diameter 8±3 16±4 mm Peak systolic gradient 39±15 3.6±5 mm Hg Mean f/u 3.1 years– MG 13±4 mm Hg 4 pts required stent re-dilation Complications: 1 death (rupture, dislodge), 1 aneurysm Chessa M et al, Eur Heart J 2005
, 52 native coarctation 74 stents implanted Diameter 8±3 16±4 mm Peak systolic gradient 39±15 3.6±5 mm Hg Mean f/u 3.1 years– MG 13±4 mm Hg 4 pts required stent re-dilation Complications: 1 death (rupture, dislodge), 1 aneurysm Chessa M et al, Eur Heart J 2005")
50
Longterm Morbidities- Recoarctation 5-14% after surgery 20-30% BA without stenting Predictors Neonates and <1 year of age <3.5 mm pre-dilation, <6 mm post-dilation Isthmus hypoplasia Monitor for HTN, gradient >20 mm Hg Intervention: stenting vs. surgery (arch hypoplasia, aneurysm)
.")
51
Longterm– Aneurysms Patch repair (up to 90% of all aneurysms) 2-8% with BA Coexisting bicuspid aortic valve/dilated ao Medial tissue abnormalities MRI 1 month, 6 months, then q3-5 years Treatment: Surgery associated with neurologic morbidity Endovascular stenting– no morbidity/ mortality in small study (6 pts) Ince H et al, Circ 2003
 2-8% with BA Coexisting bicuspid aortic valve/dilated ao Medial tissue abnormalities MRI 1 month, 6 months, then q3-5 years Treatment: Surgery associated with neurologic morbidity Endovascular stenting– no morbidity/ mortality in small study (6 pts) Ince H et al, Circ 2003")
52
Longterm– Hypertension Persistent or inappropriate ↑ with exercise BP response more common if repair in childhood ↑ frequency if repair > age 20 Structural/functional abnormalities ↓ compliance Toro-Salazar OH et al, Am J Cardiol 2002 Fawzy ME et al, JACC 2004

53
Aortic Stiffness and Coarctation 17 newborns with coarctation (no other congenital defects) studied pre and post (10d) surgery, compared with 17 controls M-mode echo, aortic pulse pressure Ascending + descending aorta measurements Distensibility= (A s -A d )/[A d (P s -P d )1333]*10 7 Stiffness index= [ln(P s /P d )]/[(D s -D d )/D d ] Circulation 2005;111: 3269-73
![Aortic Stiffness and Coarctation 17 newborns with coarctation (no other congenital defects) studied pre and post (10d) surgery, compared with 17 controls M-mode echo, aortic pulse pressure Ascending + descending aorta measurements Distensibility= (A s -A d )/[A d (P s -P d )1333]*10 7 Stiffness index= [ln(P s /P d )]/[(D s -D d )/D d ] Circulation 2005;111:](http://images.slideplayer.com/9/2490030/slides/slide_53.jpg "Aortic Stiffness and Coarctation 17 newborns with coarctation (no other congenital defects) studied pre and post (10d) surgery, compared with 17 controls M-mode echo, aortic pulse pressure Ascending + descending aorta measurements Distensibility= (A s -A d )/[A d (P s -P d )1333]*10 7 Stiffness index= [ln(P s /P d )]/[(D s -D d )/D d ] Circulation 2005;111:")
54
↑ ascending aortic stiffness, ↓ distensibility Persist early postoperatively despite surgery Innate vascular defects? Longterm consequences not addressed

55
Pregnancy Uncommon risks: aortic rupture/ dissection, intracranial hemorrhage, CHF Careful monitoring BP BA or stenting for uncontrolled HTN Higher risk of miscarriage, preeclampsia Vriend JW et al, Eur Heart J 2005

56
Survival Mayo Clinic 571 pts s/p surgery for coarctation 1946-1981 Mean age at f/u 34 Survival rates 91%, 84%, 72% at 10, 20, 30 years after surgery Best prognostic factors age, preoperative BP Euro Heart Study 551 pts with coarctation, 90% prior repair, 1998- 2000, followed until 2004 Mean age 26 5-year mortality 0.7% Cohen M et al, Circ 1989 Engelfriet P et al, Eur Heart J 2005

57
Summary Aortic coarctation is common (6-8%) among congenital CV abnormalities Associated with bicuspid aortic valve Intrinsic defects in aortic tissue abnormalities in tissue compliance Repair in childhood or as soon as diagnosed in adulthood ↓ risk persistent hypertension Surgery for <6 mos, angioplasty ± stent if older Favorable longterm outcomes HTN, recoarctation risks
 among congenital CV abnormalities Associated with bicuspid aortic valve Intrinsic defects in aortic tissue abnormalities in tissue compliance Repair in childhood or as soon as diagnosed in adulthood ↓ risk persistent hypertension Surgery for <6 mos, angioplasty ± stent if older Favorable longterm outcomes HTN, recoarctation risks")
Similar presentations




















 tricuspid valve 2. Hypoplastic right ventricle 3. Ventricular septal defect 4. Atrial.>")





