Download presentation
Presentation is loading. Please wait.

1
Diabetic Neuropathy EMEGOAKOR NONSO

2
Outline Introduction Epidemiology Classification Risk factors
Pathogenesis Clinical presentation Physical examination Investigations Staging Differential diagnosis Treatment Prognosis Conclusion

3
INTRODUCTION Is the presence of symptoms and signs of nervous dysfunction in people with diabetes after exclusion of other causes It’s the commonest complication of long standing diabetes Up to 50% of diabetics will come down with one form of neuropathy or the other.

4
Epidemiology Up to 70% of people with diabetes will experience neuropathy Some form of neuropathy may already be present at time of making a diagnosis of type 2 DM 95.7% 0f patients with DFU had neuropathy(Ikem et al 2002 More than 60% of nontraumatic lower-limb amputations in the United States occur among people with diabetes following neuropathy

5
Classification of Diabetic Neuropathy
Somatic polyneuropathy Symmetrical sensory neuropathy(distal) Asymmetrical motor neuropathy(proximal), including amyotrophy Mononeuropathy and mononeuritis multiplex Autonomic neuropathy
 Asymmetrical motor neuropathy(proximal), including amyotrophy. Mononeuropathy and mononeuritis multiplex. Autonomic neuropathy.")
6
Risk Factors Poor glycaemic control Advanced age
Long duration of diabetes Hypertension dyslipidaemia HLA DR3/DR4 phenotype Smoking Heavy alcohol intake Height i.e tall stature

7
Pathogenesis Hyperglycaemia is directly toxic to cells;altering cell growth,gene and protein expression,hence increasing ECM and TGF beta production Formation of AGES(advanced glycosylation end products); may disrupt neuronal integrity by stimulation of pro-inflammatory cytokines and complements
; may disrupt neuronal integrity by stimulation of pro-inflammatory cytokines and complements.")
8
Pathogenesis ctd Polyol pathway; accumulation of sorbitol and fructose in schwann cells lead to decreased nerve myoinositol,reduced Na-k ATPase activity, impaired axonal transport,abnormal AP propagation and breakdown of nerve structure DAG/PKc pathway; pkc alters gene transcription for fibronectin,type 4 collagen,contractile proteins,ECM in the neurones

9
Pathogenesis Oxidative stress; increased free radicals and reactive oxygen species produced in DM cause direct damage to blood vessels(vasa nervorum) leading to nerve ischaemia and hypoxia This may be the major pathogenetic mechanism in mononeuropathies
 leading to nerve ischaemia and hypoxia. This may be the major pathogenetic mechanism in mononeuropathies.")
10
Other mechanisms Immune mechanisms
Decreased neurotrophic growth factors Decreased essential fatty acids Depletion of ATP by polyADP ribosylation

11
Symmetrical sensory polyneuropathy
Most common form of diabetic neuropathy Affects distal lower extremities and hands (“stocking-glove” sensory loss) Symptoms Feeling of numbness or deadness Tingling, prickling,aching, burning sensations Paresthesia(hyper/hypoasthesia,) Loss of vibratory sensation Loss of balance in the dark Loss of pain sensation
 Symptoms. Feeling of numbness or deadness. Tingling, prickling,aching, burning sensations. Paresthesia(hyper/hypoasthesia,) Loss of vibratory sensation. Loss of balance in the dark. Loss of pain sensation.")
12
Painless nature of diabetic foot disease
However, in the insensate foot, pain sensation is absent. A significant amount of damage can occur; people are completely oblivious to this until they notice blood or swelling. For this reason it is often said that people with insensate neuropathy can have quite major surgical procedures performed without the need for anaesthetic. Slides current until 2008

13
Sensory nerve damage This slide shows a person who attended a foot clinic for treatment of ulceration, completely unaware that they were walking with a thumb-tack stuck into their foot. Had the tack not been found, this injury could quite easily have become infected, leading to serious consequences. Slides current until 2008

14
Asymmetric motor neuropathy
Proximal muscle weakness(proximal myopathy) There may be distal involvement too. DM AMYOTROPHY; painful wasting of quadriceps femoris. Neuropathic pain; burning,crawling pain in the feet,shins and anterior thigh Worse at night, with hyperaesthesias No muscle wasting Resolves with good glucose control
 There may be distal involvement too. DM AMYOTROPHY; painful wasting of quadriceps femoris. Neuropathic pain; burning,crawling pain in the feet,shins and anterior thigh. Worse at night, with hyperaesthesias. No muscle wasting. Resolves with good glucose control.")
15
Motor nerve damage As well as affecting the sensory nerves, peripheral neuropathy affects the motor nerves of the feet. This causes weakness in the intrinsic muscles of the feet, leading to contraction of the muscles and clawed toes. As the toes claw back, the fat pads are pulled forward from under the metatarsal heads, increasing the pressure under these metatarsal heads and on the tips of the toes (common places for neuropathic ulceration). Slides current until 2008
. Slides current until")
16
Diabetic Amyotrophy Diabetic amyotrophy. This syndrome is known by several names, including diabetic proximal motor neuropathy and diabetic polyradiculoneuropathy. Patients typically present with pain and weakness in the proximal large muscles of the legs and pelvic area. Muscle wasting may be unilateral or bilateral, but is usually asymmetric with bilateral involvement.4 Patients complain of severe pain in the lumbar and sacral regions. Many patients report a loss of appetite and depression as well. Improvement may take from 6 months to 2 years. Immunotherapy may be beneficial and accelerate recovery.11

17
Cheiroarthropathy

18
Trigger finger

19
Mononeuropathy Peripheral mononeuropathy
Single nerve damage due to compression or ischemia Pain and motor weakness of muscles supplied Any nerve may be involved CN 3, 6,7,peroneal nerve e.t.c Mononeuritis multiplex-Multiple ischemic nerve damage Occurs in wrist (carpal tunnel syndrome), elbow, or foot (unilateral foot drop)
, elbow, or foot (unilateral foot drop)")
20
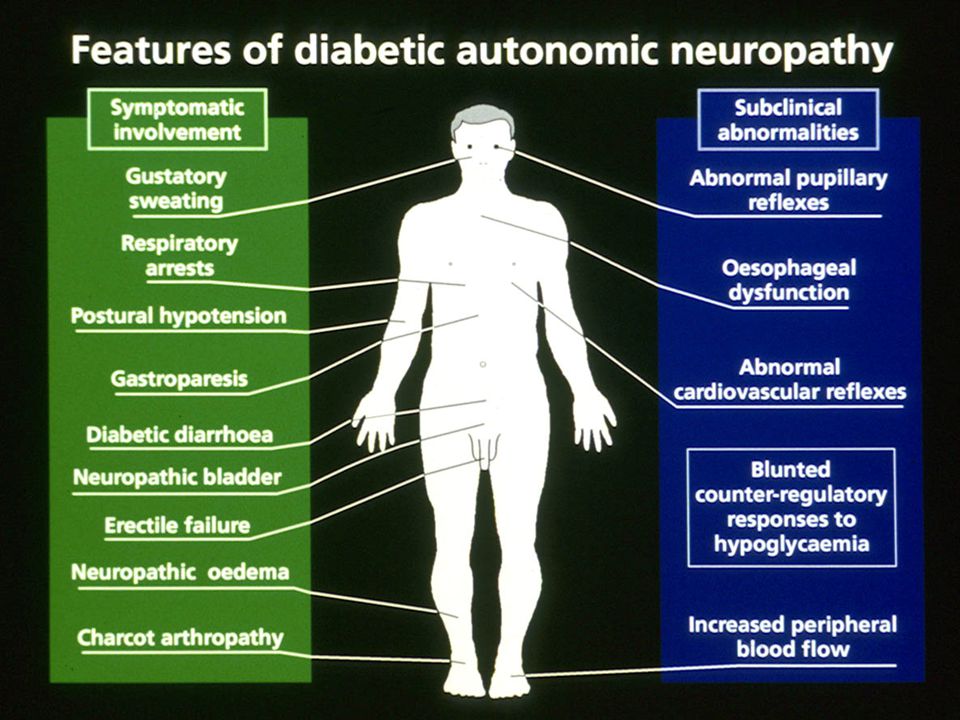
Autonomic neuropathy CVS; resting tachycardia, fixed heart rate, orthostatic hypotension, loss of sinus arrhythmia, reduced exercise tolerance silent MI, hypoglycemia unawareness GIT; gastroparesis, autonomic diarrhea alternating with constipation, abdominal pain, fecal incontinence, abdominal bloating

21
Autonomic neuropathy ctd
Urogenital system; incomplete bladder emptying, stasis, UTI,atonic painless distended bladder; erectile dysfunction and retrograde ejaculation, loss of libido, dyspareunia, Sudomotor symptoms; hyperhidrosis, anhidrosis, gustatory sweating, heat intolerance, dry skin

23
Physical Examination. Inspect feet for features/sequele of neuropathy; callousties, cracks,fissures, interosseous muscle wasting, flattened foot, high arch, claw toe, charcot arthropathy. Note following features on hand, wasting of small hand muscles, trigger finger, cheiroarthropathy

24
Autonomic nerve damage
Damage to the autonomic nervous system accompanies significant peripheral neuropathy. Normally, feet perspire, keeping the skin moist and supple. In autonomic neuropathy, people lose the ability to perspire; the skin dries out and becomes cracked. These cracks are a very common portals for infection. Slides current until 2008

25
Localized callus When an increase in pressure and discomfort occurs, people with normal sensation change their gait. People with neuropathy do not feel pain and continue to walk in the same way. This leads to a build up of callus at the site of most pressure. Ultimately this hard, localized callus can cause the tissue underneath to breakdown forming ulceration. As a preventive measure, all callus should be removed. It is particularly important to note that bleeding callus is indicative of possible ulceration and should be removed immediately. Slides current until 2008

26
Complications of Sensorimotor/poly neuropathy
Ulceration (painless) Neuropathic edema Charcot arthropathy Callosities
 Neuropathic edema. Charcot arthropathy. Callosities.")
27
NEUROLOGICAL ASSESMENT OF THE FOOT
Light touch using cotton wool. Pin prick Joint position sense Vibration sense Temperature perception- hot & cold Light pressure using Semmes-Weinstein monofilament Deep tendon reflexes. Heel toe walking test

28
Screening for Neuropathy
128 Hz tuning fork for testing of vibration perception 10g Semmers monofilament The main reason is to identify patients at risk for development of diabetic foot(LOPS)
")
29
Diabetic peripheral neuropathy screening tests
Test sensation Biothesiometer Tuning fork 10 gm monofilament Ankle reflexes As with the other long-term complications of diabetes, it is important to screen all people on a regular basis so that they can be stratified according to their level of risk. Those who are identified as being at high risk of ulceration require more intensive medical and podiatry treatment (where available) and education. In some clinics, vibration perception can be tested using a biothesiometer. This is a semi-quantitative instrument that allows serial measurement of vibration perception over time. The vibration probe is applied to the dorsal of the foot, between the first and second metatarsal heads. The voltage is gradually increased from 0 up to 50 if necessary and the result recorded when the person indicates that they can feel the vibration. People with neuropathy defined as a VPT of more than 30 volts are considered to be at high risk of developing neuropathic ulceration. Sensation deteriorates with age, and a high biothesiometer reading can result from this alone. Therefore, in order to determine the risk of foot ulceration in elderly people, consideration of other factors – such as the condition of the skin and feet – is most important. A more cost-effective and, hence, more widely available tool for testing the ability of the foot to detect pressure is the 10 g Semmes Weinstein monofilament. The person should be asked to close their eyes while the monofilament is pressed perpendicularly to the plantar surface of the foot at the first and fifth metatarsal heads. Pressure is increased until the monofilament buckles, exerting a force of 10 g. If the person cannot feel the pressure at one or both sites, this is considered to be abnormal and recorded as ‘cannot feel’. An inability to feel the monofilament indicates a loss of pressure sensation sufficient to increase significantly the risk of ulceration. Both ankle reflexes should be tested in the usual manner and recorded as absent or present. Slides current until 2008
 and education. In some clinics, vibration perception can be tested using a biothesiometer. This is a semi-quantitative instrument that allows serial measurement of vibration perception over time. The vibration probe is applied to the dorsal of the foot, between the first and second metatarsal heads. The voltage is gradually increased from 0 up to 50 if necessary and the result recorded when the person indicates that they can feel the vibration. People with neuropathy defined as a VPT of more than 30 volts are considered to be at high risk of developing neuropathic ulceration. Sensation deteriorates with age, and a high biothesiometer reading can result from this alone. Therefore, in order to determine the risk of foot ulceration in elderly people, consideration of other factors – such as the condition of the skin and feet – is most important. A more cost-effective and, hence, more widely available tool for testing the ability of the foot to detect pressure is the 10 g Semmes Weinstein monofilament. The person should be asked to close their eyes while the monofilament is pressed perpendicularly to the plantar surface of the foot at the first and fifth metatarsal heads. Pressure is increased until the monofilament buckles, exerting a force of 10 g. If the person cannot feel the pressure at one or both sites, this is considered to be abnormal and recorded as ‘cannot feel’. An inability to feel the monofilament indicates a loss of pressure sensation sufficient to increase significantly the risk of ulceration. Both ankle reflexes should be tested in the usual manner and recorded as absent or present. Slides current until")
30
Diagnosis Tests for peripheral neuropathy Light touch and pin prick
Vibration Deep tendon reflexes Muscle bulk and power Vibration-tuning fork or biothesiometer, N < 25V LT: Semmes-Weinstein monofilament. (10g 6 places) Thermal thresholds: research devices Pain: pinchometer or weighted needles
 Thermal thresholds: research devices. Pain: pinchometer or weighted needles.")
31
Tests for autonomic neuropathy
Resting heart rate >100bpm HR variation during deep breathing (6 breaths per minute) Max-min > 15bpm (<10 is abnormal) R-R interval >1.17 HR response to vasalva-R-R>1,2 <16mmHg diastolic pressure rise during sustained hand grip Postural BP-2 mins after standing Fall< 10mmHg normal >30 mmHg abnormal
 Max-min > 15bpm (<10 is abnormal) R-R interval >1.17. HR response to vasalva-R-R>1,2. <16mmHg diastolic pressure rise during sustained hand grip. Postural BP-2 mins after standing. Fall< 10mmHg normal. >30 mmHg abnormal.")
32
Investigations FBS and HbA1c EMG Nerve biopsy ECG FBC SEUC
Vitamin B12 and folate levels ESR,CRP TFT ANA RF Serum protein electrophoresis MRI and CT

33
Staging N0-No neuropathy N1-Signs but no symptoms
N2a-Mild symptomatic,pxt able to heel walk N2b-Severe symptomatic,pxt unable to heel walk N3-disabling diabetic polyneuropathy

34
Differential diagnosis
Herpes Simplex mononeuropathy Ethanol neuropathy Vasculitic neuropathy Amyloid polyneuroathy Chronic inflammatory demyelinating olyradiculopathy B12/folate Malignancy Myocardial infarction Renal failure Drugs Cord problems Leprosy HIV/AIDS

35
Treatment Tight and stable glucose control slows the progression of neuropathy Drugs used in peripheral neuropathy include the antidepressants(amitryptiline, desipramine, imipramine, nortriptyline) SSRIs e.g duloxetine anticonvulsants like pregabalin, gabapentin, carbamazepine, lamotrigine However response haven’t been satisfactory and patients need lots of psychological support.
 SSRIs e.g duloxetine anticonvulsants like pregabalin, gabapentin, carbamazepine, lamotrigine. However response haven’t been satisfactory and patients need lots of psychological support.")
36
Neuropathic treatment ctd
Other measures include, opiates,mexiletine,Topical capsaicin, lipoic acid, transdermal lidocaine patches TENS(transcutaneous electrical nerve stimulation) Use of custom shoes for neuropathic foot deformities Occupational therapy
 Use of custom shoes for neuropathic foot deformities. Occupational therapy.")
37
Autonomic neuropathy-GIT
Gastroparesis Improve glycaemic control Frequent small easier to digest meals Prokinetic drugs Metoclopramide, domperidone, cisapride, erythromycin (250 mg tds) Jejunostomy Diarrhoea Codeine/loperamide/diphenoxylate Treat bacterial overgrowth (oxytet/erythromycin) if suspected/present Constipation; laxatives e.g senna
 Jejunostomy. Diarrhoea. Codeine/loperamide/diphenoxylate. Treat bacterial overgrowth (oxytet/erythromycin) if suspected/present. Constipation; laxatives e.g senna.")
38
Autonomic neuropathy-CVS
Orthostatic hypotension; Increase dietary fluid and salt intake Avoid dehydration Compression stockings Fludrocortisone, midodrine, clonidine

39
Autonomic neuropathy-UGS
Bladder and voiding problems Intermittent or permanent self catheterization Prophylactic antibiotics ED: phosphodiesterase type 5 inhibitors, apomorphone, intracarvenosal or intraurethral prostaglandins, vacuum devices, or penile prosthesis, psychotherapy

40
Further measures Management and avoidance of other risk factors;
Treat hypertension and dyslipidemia Avoid alcohol and smoking Folate and B12 supplementation Follow up; Examine feet Use monofilament and tuning fork Glycaemic assessment (HBA1c)
")
41
Counselling for patients with neuropathic foot
Do check your feet each day for blisters, cuts, scratches, reddened areas. Use a mirror or ask someone else to help look at the soles. Do wash your feet each day. Dry them carefully especially between the toes. Do avoid extremely hot or cold water. Test them with your hand or elbow before use. Do apply a very thin coat of lubricating oil or cream on the skin after bathing if your skin is dry but not between the toes

42
Counseling ctd Do ask about therapeutic shoes if you have a foot deformity, such as bunions or claw toes or previous ulcer Do see your care provider for regular foot examination. Always protect your feet. Wear shoes both in and outside the house to avoid injury

43
Counseling ctd Don’t walk barefoot.
Don’t walk on hot surfaces, such as sandy beaches or the cement, roads etc. Don’t put hot water bottles, electric blanket or heating pad on your feet. Don't cut corns, calluses or use chemical agents, corn plasters, strong antiseptics on your feet. Don’t soak your feet unless professionally advised. Don’t wear shoes without stockings. Don’t wear sandals with thongs between the toes. Avoid pointy-toe shoes, high heels, stilettos, strapless and backless shoes Don’t smoke Don’t put jewellery on your feet

44
Prognosis Repetitive trauma to a neuropathic area may cause ulceration and infection and amputations Neuropathic foot ulceration and amputation is the commonest cause of admission of DM patients Mortality is mainly from cardiac autonomic neuropathy. Such patients are at risk of sudden death

45
conclusion DM neuropathy is the commonest chronic complication in diabetics Poor glycaemic control and prolonged duration of DM are the greatest risk factors Major cause of non traumatic lower limb amputations as well as sudden deaths Strict blood glucose control is advised to prevent or delay it’s progression

46
Thank you for listening

Similar presentations











 affect your feet? How to take care of your feet What shoes.>")







