Download presentation
Presentation is loading. Please wait.

1
Tumors of Intestines

2
Introduction Overall, colorectal cancer ranks second only to bronchogenic carcinoma among the cancer killers. Adenocarcinomas constitute the vast majority of colorectal cancers and represent 70% of all malignancies arising in the gastrointestinal tract.

3
Terminology •A polyp is a tumorous mass that protrudes into the lumen of the gut; traction on the mass may create a stalked or pedunculated polyp. Alternatively the polyp may be sessile, without a definable stalk. •Non-neoplastic Polyps abnormal mucosal maturation, inflammation do not have malignant potential (excl.Peutz-Jeghers) •Neoplastic Polyps: adenomatous polyps, or adenomas, precursors of carcinoma.
 •Neoplastic Polyps: adenomatous polyps, or adenomas, precursors of carcinoma.")
4
Non-neoplastic (benign) Polyps Hyperplastic polyps
Hamartomatous polyps Juvenile polyps Peutz-Jeghers polyps Inflammatory polyps Lymphoid polyps

5
Neoplastic epithelial lesions
Benign lesions: Neoplastic polyp Adenoma Malignant lesions: Adenocarcinoma Carcinoid tumor Anal zone (anorectal) carcinoma Mesenchymal lesions (benign/malignant) Lymphoma
 carcinoma. Mesenchymal lesions (benign/malignant) Lymphoma.")
6
Non-neoplastic (benign) Polyps
Common Hyperplastic polyps Adults Rectosigmoid Multiple Nipple-like, Small protrusions (5 mm) Abundant crypts. Juvenile polyps Children Rectum Single Round mass 1-3 cm Dilated cystic glands.
 Abundant crypts. Juvenile polyps. Children. Rectum. Single. Round mass. 1-3 cm. Dilated cystic glands.")
7
Hyperplastic polyp Polyps Juvenile polyp

8
Sessile Pedunculated

9
Adenomas Small-pedunculated; large-sessile Colon Malignancy:
Familial predisposition Risk of carcinoma Subtypes: Tubular Villous Tubulovillous Malignancy: Rare: tubular adenoma less than 1 cm High: sessile villous adenomas more than 4 cm Dysplasia: villous adenomas.

10
Tubulovillous adenomas:
Tubular adenomas: Colon (rectosigmoid) Small-sessile; large-pedunculated Stalk is covered by normal mucosa Tumor is composed of neoplastic epithelium Intramucosal Ca or invasive Ca. Villous adenomas: Rectum/rectosigmoid Larger than tubular Sessile Cauliflower-like Dysplasia Ca. Tubulovillous adenomas: Peduculated or sessile Mix of tubular and villous patterns Dysplasia Malignancy.
 Small-sessile; large-pedunculated. Stalk is covered by normal mucosa. Tumor is composed of neoplastic epithelium. Intramucosal Ca or invasive Ca. Villous adenomas: Rectum/rectosigmoid. Larger than tubular. Sessile. Cauliflower-like. Dysplasia Ca. Tubulovillous adenomas: Peduculated or sessile. Mix of tubular and villous patterns. Dysplasia. Malignancy.")
11
Adenoma

12
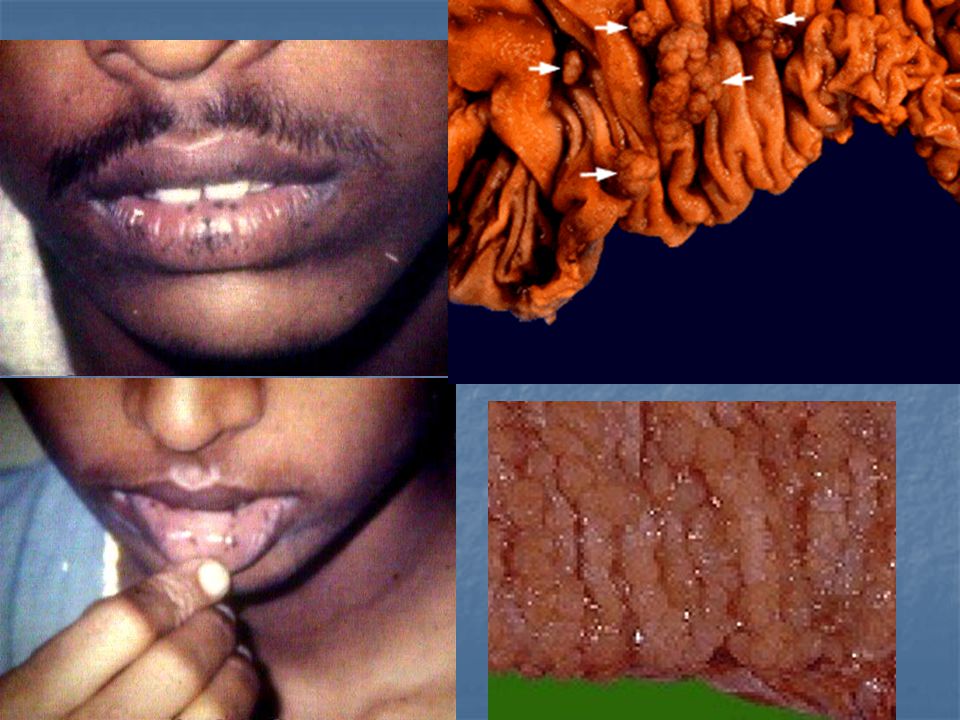
Familial polyposis syndromes
Peutz-Jeghers Syndrome Multiple polyps (polyposis coli) large, firm polyps with a tree-like structure distinctive freckles on the lips, palms, and genitals risk for colon cancer. Turcot's syndrome Multiple polyps brain tumors. Gardner's syndrome Multiple polyps minor birth defects risk for other tumors (notably mesenchymal). Cowden's syndrome Risk of tumors of: Thyroid Breast Uterus Skin.
 large, firm polyps with a tree-like structure. distinctive freckles on the lips, palms, and genitals. risk for colon cancer. Turcot s syndrome. Multiple polyps. brain tumors. Gardner s syndrome. Multiple polyps. minor birth defects. risk for other tumors (notably mesenchymal). Cowden s syndrome. Risk of tumors of: Thyroid. Breast. Uterus. Skin.")
14
Part One Tumors of Small Intestine

15
Small Intestine tumors:
Small intestine -75% but tumors – 3-6% Benign tumors (common) Adenoma(25%), lipoma & leiomyoma. Malignant tumors (rare; <1%) Adenocarcinoma of Duodenum or Jejunum, Carcinoid, Lymphoma, Sarcoma Present at late stage, 70% 5 year survival.
 Adenoma(25%), lipoma & leiomyoma. Malignant tumors (rare; <1%) Adenocarcinoma of Duodenum or Jejunum, Carcinoid, Lymphoma, Sarcoma. Present at late stage, 70% 5 year survival.")
16
Classification Non neoplastic polyps Neoplastic – epithelial
Hyperplastic, lymphoid & hamartomatous Inflammatory Neoplastic – epithelial Benign – Adenoma (ampulla of Vater) Malignant – Adenocarcinoma, carcinoid Neoplastic – Mesenchymal Benign - Lipoma, leiomyoma, neuroma, angioma Malignant – Leiomyosarcoma, liposarcoma. Lymphoma
 Malignant – Adenocarcinoma, carcinoid. Neoplastic – Mesenchymal. Benign - Lipoma, leiomyoma, neuroma, angioma. Malignant – Leiomyosarcoma, liposarcoma. Lymphoma.")
17
Benign tumors: Lipoma Most common Mature adipose tissue

18
Adenocarcinoma Napkin-ring or polypoid Duodenum (ampulla of Vater’s)
Spreading: Regional lymph nodes Liver Obstructive jaundice.

19
Tumors of Colon & Rectum

20
Colorectal carcinoma Adenocarcinomas (98%)
often arises in one of the benign neoplastic colonic polyp risk factors (1) mild hereditary defects in anti-oncogenes lost in colon cancer, (2) years of eating the typical western diet. Low content of vegetables High content of refined carbohydrates High content of fat (animal) Low content of micronutrients (vitamins A, C, E).
 mild hereditary defects in anti-oncogenes lost in colon cancer, (2) years of eating the typical western diet. Low content of vegetables. High content of refined carbohydrates. High content of fat (animal) Low content of micronutrients (vitamins A, C, E).")
21
Morphology Proximal colon tumors: polypoid
Cecum and ascending colon: exophytic Distal colon: napkin-ring Progression: slow (years) Types: Gut: Adenocarcinoma Mucin production Anal zone: Squamous cell carcinoma Spreading: Regional lymph nodes Liver
 Types: Gut: Adenocarcinoma. Mucin production. Anal zone: Squamous cell carcinoma. Spreading: Regional lymph nodes. Liver.")
23
Carcinoid Tumors 2% of colorectal malignancies. Origin: Neuroendocrine cells (paracrine, Kulchitsky, enterochromaffin, neurosecretory, chromaffin) Location: gut (common in appendix) pancreas or peripancreatic tissue, lungs, biliary tree liver. Rectal and appendiceal carcinoids almost never metastasize The classic carcinoid syndrome (serotonin) (1) wheezing (asthmatic); (2) flushing (vasomotor); (3) fibrosis (cardiac, pulmonic, pleural, pelvic); (4) intestinal hypermotility.
 pancreas or peripancreatic tissue, lungs, biliary tree. liver. Rectal and appendiceal carcinoids almost never metastasize. The classic carcinoid syndrome (serotonin) (1) wheezing (asthmatic); (2) flushing (vasomotor); (3) fibrosis (cardiac, pulmonic, pleural, pelvic); (4) intestinal hypermotility.")
24
Midgut carcinoids: Foregut carcinoids: small intestinal, appendiceal,
most colonic carcinoids. These are usually argyrophil (hormonally active). Foregut carcinoids: lung, duodenal, biliary carcinoids. These are almost never argyrophil (hormonally inactive).
. Foregut carcinoids: lung, duodenal, biliary carcinoids. These are almost never argyrophil (hormonally inactive).")
26
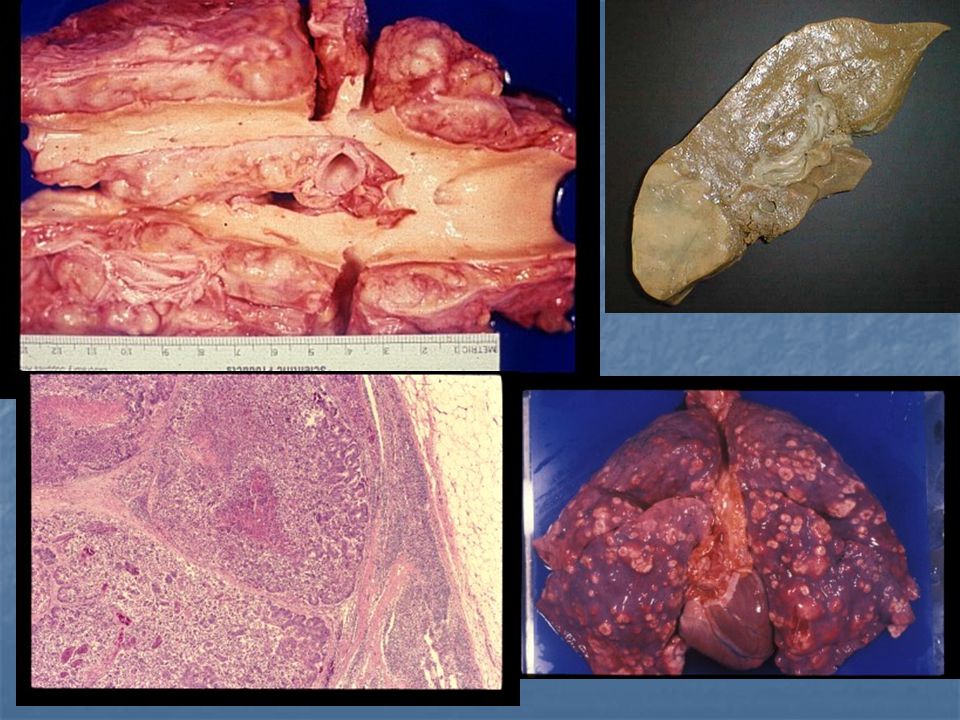
Gastrointestinal lymphoma
Less common than carcinomas Western lymphomas are usually familiar B-cell lymphomas Mediterranean lymphomas usually feature plasmacytoid differentiation (a subset is alpha-heavy chain disease). Sprue-associated lymphoma exhibits T-cell markers
. Sprue-associated lymphoma exhibits T-cell markers.")
27
Lymphoma

28
THANK YOU

Similar presentations









 have two basic components. Proliferating neoplastic cells that constitute.>")










>")