Download presentation
Presentation is loading. Please wait.

1
Asymptomatic carotid stenosis Identification of the high-risk patient Richard Bulbulia Consultant Vascular Surgeon CTSU, University of Oxford And Cheltenham General Hospital

3
Projected Rise in Stroke Mortality Worldwide to 2030

4
Average annual risk rates of Ipsilateral stroke in patients with at least 50% asymptomatic carotid stenosis OXVASC study, Stroke 2010;41:e11-e17.

5
Residual Risk

6
Despite intensive statin therapy residual cardiovascular risk remains high SEARCH trial: a trial comparing intensive vs. moderate LDL- lowering (80 mg simvastatin vs. 20 mg) 6031 post-MI patients allocated simvastatin 80mg daily for 7 years Annual vascular death rate: 1.4% Annual major vascular event rate:3.6% 10-year risk of major vascular event over 30% and risk of death almost 15%
 6031 post-MI patients allocated simvastatin 80mg daily for 7 years Annual vascular death rate: 1.4% Annual major vascular event rate:3.6% 10-year risk of major vascular event over 30% and risk of death almost 15%.")
7
Residual Stroke Risk 1.0% yearly post-procedural stroke risk in ACST 10 year follow-up amongst those allocated immediate CEA Stroke rates of 1.0% per year seen in the long- term follow-up of HPS (17,000 high-risk patients receiving good LDL-lowering therapy)
")
8
What is the net benefit of carotid intervention? Procedural risk Long-term efficacy Natural history of asymptomatic stenosis

10
ACST-1, Lancet 2010

11
Determinants of stroke risk

12
Degree of stenosis and stroke risk % StenosisImmediate CEADeferral <701.3% (13/976)2.3% (23/989) 70-790.9% (28/3091)2.0% (59/3023) 80-891.0% (25/2522)2.1% (58/2754) 90-991.1% (33/2993)1.7% (48/2789) ACST 10-year Results: First non-perioperative stroke by % ipsilateral stenosis
2.3% (23/989) % (28/3091)2.0% (59/3023) % (25/2522)2.1% (58/2754) % (33/2993)1.7% (48/2789) ACST 10-year Results: First non-perioperative stroke by % ipsilateral stenosis")
13
Contralateral occlusion and stroke risk Contralateral statusImmediate CEADeferral Patent0.9% (56/6452)1.6% (109/6690) Occluded1.2% (10/846)2.4% (18/736) ACST 10-year Results: First non-perioperative stroke by contralateteral status
1.6% (109/6690) Occluded1.2% (10/846)2.4% (18/736) ACST 10-year Results: First non-perioperative stroke by contralateteral status")
14
TCD micro-emboli and stroke risk Source: The Lancet Neurology 2010; 9:663-671 (DOI:10.1016/S1474-4422(10)70120-4)The Lancet Neurology 2010; 9:663-671
 )The Lancet Neurology 2010; 9:")
15
Jonathan Y. Streifler MD, Anne G. den Hartog MD, Samuel Pan, Hongchao Pan PhD, Richard Bulbulia MD, Dafydd J. Thomas MD, Alison Halliday MD on behalf of the ACST-1 trial collaborators ISC Hawaii Disclosure: None

16
Silent brain infarcts MRI-defined silent brain infarcts (SBI’s) are detected in 20% of healthy elderly people SBI’s are detected in up to 50% of patients in selected series. Although silent infarcts, by definition, lack clinically overt stroke-like symptoms, they are associated with subtle deficits in physical and cognitive function that commonly go unnoticed. Vermeer SE et al, Silent brain infarcts: a systematic review. Lancet Neurol 2007;6:611

17
SBI’s in patients undergoing CEA for asymptomatic carotid stenosis. Cao P. et al. J Vasc Surg. 1999;29:995 Conclusion: In our experience, preoperative SBI did not occur more frequently in the hemisphere ipsilateral to asymptomatic severe carotid stenosis. Although our study lacks a medically treated control group, our data show that SBI is predictive of poor neurologic outcome in asymptomatic patients undergoing CEA. We conclude that CT before CEA, selectively applied, provides information on long-term neurologic prognosis and that a less aggressive attitude towards CEA in asymptomatic patients with SBI may be justified

18
Stroke-free rate in 462 patients with 60% to 99% carotid artery stenosis in relation to “embolic” infarction on CT brain scans. Kakkos SK et al. ACSRS Study Group, J Vasc Surg, 2009,:49:902–90

19
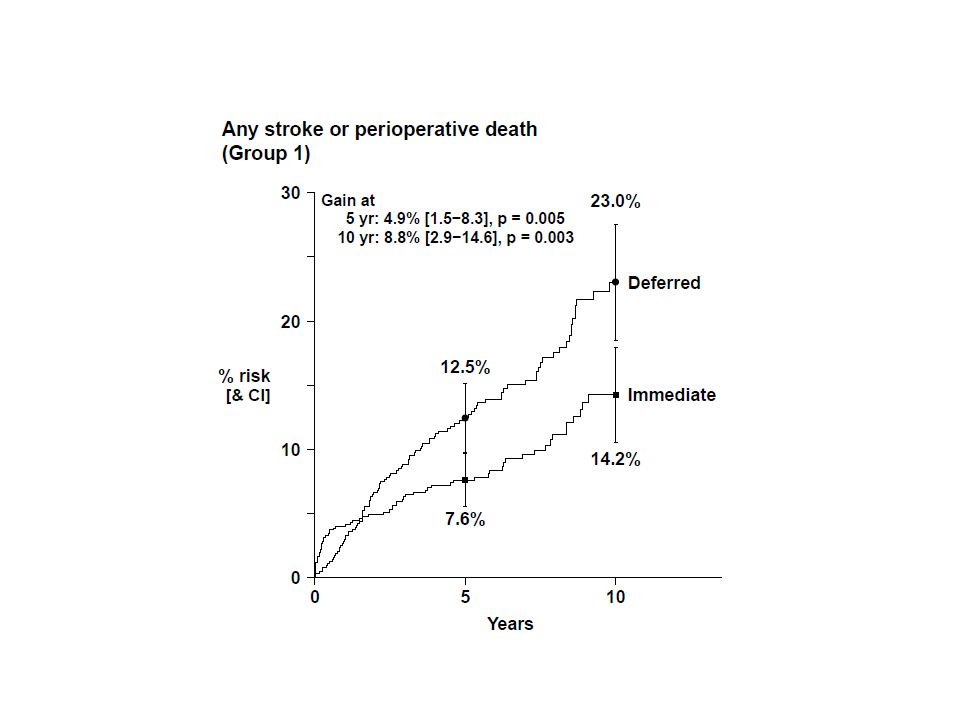
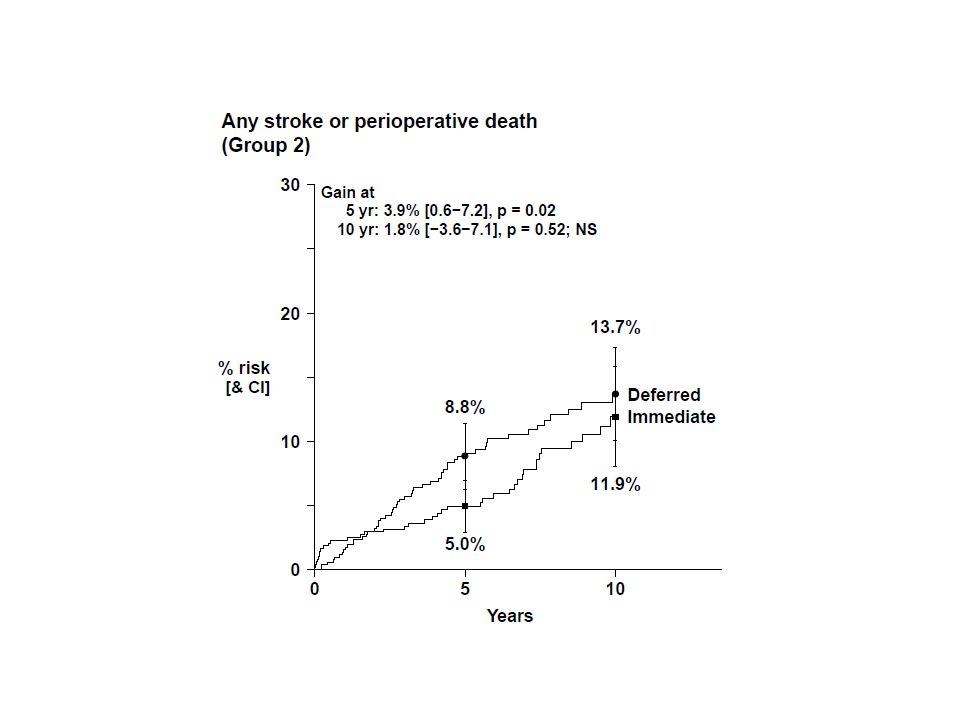
Methods ACST-1 included 3120 patients Baseline brain imaging was identified in 2333 patients and these were divided into 2 groups: 1. Group 1: 1331 patients with prior brain infarcts (i.e. radiological evidence of an asymptomatic infarct or prior ischemic symptoms >6 months prior to randomization). Only 31 had normal brain imaging. 2. Group 2: 1002 patients with normal imaging and no prior symptoms. All participants were randomly allocated either immediate or deferred CEA.
. Only 31 had normal brain imaging. 2. Group 2: 1002 patients with normal imaging and no prior symptoms. All participants were randomly allocated either immediate or deferred CEA..")
20
Category Group 1 (1331) Group 2 (1002) P-value n%n% Sex0.002 Men922(69.3)632(63.1) Women409(30.7)370(36.9) Age at entry (years)0.2 < 65407(30.6)272(27.2) 65-74651(48.9)513(51.2) ≥ 75273(20.5)217(21.7) mean ± SD68.5 ± 7.668.8 ± 7.6 0.2 Ipsilateral carotid diameter reduction (% by ultrasound)0.02 < 80569(42.8)373(37.2) 80-89355(26.7)282(28.1) ≥ 90407(30.6)347(34.6) Ispsilateral stenosis 79.0 ± 11.780.2 ± 11.0 0.01 Contralateral stenosis >50% (incl occlusion) ?0.6 Yes372(28.0)269(26.9) No959(72.1)733(73.2) Baseline characteristics of groups 1 vs. 2

21
Diabetes?1.0 Yes267(20.1)202(20.2) No1064(79.9)800(79.8) Cardiac disease?0.9 Yes429(32.2)320(31.9) No902(67.8)682(68.1) Hyperlipidemia?0.6 Yes1033(77.6)787(78.5) No298(22.4)215(21.5) Hypertension?0.01 Yes1138(85.5)818(81.6) No193(14.5)184(18.4) Immediate CEA?0.3 Yes677(50.9)486(48.5) No654(49.1)516(51.5) Category Group 1 (1331) Group 2 (1002) P-value n%n% Baseline characteristics of groups 1 vs. 2 (continued)
.")
22
PBI No PBI

23
Stroke type Both groups (N=2333) n (%) Group 1 (N=1331) n (%) Group 2 (N=1002) n (%) p-value* Territory (regardless of side) Carotid222 (9.5)138 (10.5)84 (8.4)0.03 VB23 (1.0)18 (1.4)5 (0.5)0.03 Unknown14 (0.6)11 (0.8)3 (0.3)0.06 Nature Ischaemic166 (7.1)110 (8.3)56 (5.6)0.005 Hemorrhagic22 (0.9)12 (0.9)10 (1.0)1.0 Unknown71 (3.0)45 (3.4)26 (2.6)0.1 Lacunar25 (1.1)17 (1.3)8 (0.8)0.3 Arterial147 (6.3)100 (7.5)47 (4.7)0.003 Cardio-embolic33 (1.4)21 (1.6)12 (1.2)0.2 Disabling77 (3.3)53 (4.0)24 (2.4)0.03 Non-disabling109 (4.7)67 (5.0)42 (4.2)0.2 Any259 (11.1)167 (12.5)92 (9.2)0.002 Number of the first episode of stroke events observed in group 1 and 2 * From Cox proportional hazards model, adjusting all other baseline variables listed in table 1
 n (%) Group 1 (N=1331) n (%) Group 2 (N=1002) n (%) p-value* Territory (regardless of side) Carotid222 (9.5)138 (10.5)84 (8.4)0.03 VB23 (1.0)18 (1.4)5 (0.5)0.03 Unknown14 (0.6)11 (0.8)3 (0.3)0.06 Nature Ischaemic166 (7.1)110 (8.3)56 (5.6)0.005 Hemorrhagic22 (0.9)12 (0.9)10 (1.0)1.0 Unknown71 (3.0)45 (3.4)26 (2.6)0.1 Lacunar25 (1.1)17 (1.3)8 (0.8)0.3 Arterial147 (6.3)100 (7.5)47 (4.7)0.003 Cardio-embolic33 (1.4)21 (1.6)12 (1.2)0.2 Disabling77 (3.3)53 (4.0)24 (2.4)0.03 Non-disabling109 (4.7)67 (5.0)42 (4.2)0.2 Any259 (11.1)167 (12.5)92 (9.2)0.002 Number of the first episode of stroke events observed in group 1 and 2 * From Cox proportional hazards model, adjusting all other baseline variables listed in table 1")
24
Univariate analysisMultivariate analysis CategoryHR95% CIΧ21Χ21 p-valueHR95% CIΧ21Χ21 p-value Group 1 vs 21.501.16-1.939.70.0021.511.17-1.959.80.002 Men vs Women1.100.85-1.420.5 1.060.82-1.390.20.6 Age (per 10 years increase)1.181.00-1.393.70.051.231.03-1.465.20.02 Ipsilateral stenosis (per 10% ↑)0.970.87-1.070.40.50.940.85-1.051.30.3 Contralateral stenosis vs no1.110.85-1.460.60.41.140.87-1.490.80.4 Diabetes vs no1.601.21-2.1210.90.0011.641.23-2.1711.70.0006 Cardiac disease vs no1.170.90-1.511.40.21.090.84-1.410.40.5 Hyperlipidemia vs no0.970.72-1.300.050.81.030.76-1.390.030.9 Hypertension vs no1.260.89-1.791.70.21.160.82-1.660.70.4 Immediate CEA vs Deferral0.670.52-0.8610.00.0020.660.52-0.8510.50.001 Hazard ratio (HR) of stroke, by baseline characteristics ↑ = increase
 Ipsilateral stenosis (per 10% ↑) Contralateral stenosis vs no Diabetes vs no Cardiac disease vs no Hyperlipidemia vs no Hypertension vs no Immediate CEA vs Deferral Hazard ratio (HR) of stroke, by baseline characteristics ↑ = increase")
25
Cause of death Both groups (N=2333) n (%) Group 1 (N=1331) n (%) Group 2 (N=1002) n (%) p-value* Stroke90 (3.9)61 (4.6)29 (2.9)0.009 Other vascular or cardiac433 (18.6)256 (19.2)177 (17.7)0.06 Cancer165 (7.1)102 (7.7)63 (6.3)0.09 Other known cause120 (5.1)76 (5.7)44 (4.4)0.03 Unknown cause86 (3.7)46 (3.5)40 (4.0)0.9 Any894 (38.3)541 (40.6)353 (35.2)0.0003 Cause-specific numbers of deaths, separated for group 1 and group 2 * From Cox proportional hazards model, adjusting all other baseline variables listed in table 1
 n (%) Group 1 (N=1331) n (%) Group 2 (N=1002) n (%) p-value* Stroke90 (3.9)61 (4.6)29 (2.9)0.009 Other vascular or cardiac433 (18.6)256 (19.2)177 (17.7)0.06 Cancer165 (7.1)102 (7.7)63 (6.3)0.09 Other known cause120 (5.1)76 (5.7)44 (4.4)0.03 Unknown cause86 (3.7)46 (3.5)40 (4.0)0.9 Any894 (38.3)541 (40.6)353 (35.2) Cause-specific numbers of deaths, separated for group 1 and group 2 * From Cox proportional hazards model, adjusting all other baseline variables listed in table 1")
27
Univariate analysisMultivariate analysis CategoryHR95% CIΧ21Χ21 p-valueHR95% CIΧ21Χ21 p-value Group 1 vs 21.301.12-1.5211.10.00091.301.11-1.5210.70.001 Men vs Women1.291.09-1.539.10.0031.251.05-1.486.40.01 Age (per 10 yrs. increase)1.371.23-1.5333.4<0.00011.431.27-1.6037.8<0.0001 Ipsilateral stenosis (per 10% ↑)1.040.98-1.121.60.20.990.93-1.060.050.8 Contralateral stenosis vs no1.251.06-1.487.20.0071.271.08-1.508.00.005 Diabetes vs no1.721.45-2.0538.0<0.00011.721.45-2.0537.5<0.0001 Cardiac disease vs no1.631.39-1.9037.8<0.00011.481.26-1.7323.6<0.0001 Hyperlipidemia vs no0.930.78-1.120.60.51.010.84-1.210.0031.0 Hypertension vs no1.150.93-1.421.70.21.020.82-1.260.030.9 Immediate CEA vs Deferral0.940.80-1.090.70.40.930.80-1.090.80.4 Hazard ratio (HR) of stroke or vascular death, by baseline characteristics ↑ = increase
 < < Ipsilateral stenosis (per 10% ↑) Contralateral stenosis vs no Diabetes vs no < < Cardiac disease vs no < < Hyperlipidemia vs no Hypertension vs no Immediate CEA vs Deferral Hazard ratio (HR) of stroke or vascular death, by baseline characteristics ↑ = increase.")
32
In ACST 1… 1. Prior brain infarcts were common (>1/3 rd ) 2. Associated with increased risk of carotid territory stroke 3. May help identify a population in whom carotid intervention is particularly worthwhile

Similar presentations