Download presentation
Presentation is loading. Please wait.

1
Programa InForMed 2006-2007 Programa de Información y Formación Médica Continuada Para el uso racional del medicamento

2
TOXICITAT CARDIACA AL TRACTAMENT DEL CÀNCER DE MAMA Jesús Alarcón Company Oncologia mèdica HUSD

3
CARDIOTOXICITAT INDUÏDA PER FÀRMACS FÀRMACEFECTE CARDIAC Antraciclines Arritmies Miocardiopatia congestiva Vessaments pleurals Ciclofosfamida Insuficiència cardiaca congestiva aguda Miocarditis hemorràgica Vessaments pleurals 5 FUIsquèmia miocàrdica Paclitaxel Arrítmies (bradicàrdia) Canvis EKG, isquèmia TrastuzumabInsuficiència cardiaca congestiva
 Canvis EKG, isquèmia TrastuzumabInsuficiència cardiaca congestiva")
5
Anthracyclines Cardiotoxic effects may manifest during early, late, or posttreatment [1] –Early toxicity uncommon Chronic, potentially irreversible doxorubicin-associated myopathy of great concern [2,3] –Cardiomyopathy risk relative to cumulative dose Damage starts with the first administration –Seldom noted at low cumulative dosages because of cardiac reserves Clinical expression low (< 5%) when dose < 400 mg/m 2 Clinical expression becomes greater as dose surpasses 450 mg/m 2 1. Bristow M, et al. Am J Med. 1978;65:823-832. 2. Lefrak E, et al. Cancer. 1973;32:302-314. 3. Minow R, et al. Cancer. 1977;39:1397-1402.
![Anthracyclines Cardiotoxic effects may manifest during early, late, or posttreatment [1] –Early toxicity uncommon Chronic, potentially irreversible doxorubicin-associated myopathy of great concern [2,3] –Cardiomyopathy risk relative to cumulative dose Damage starts with the first administration –Seldom noted at low cumulative dosages because of cardiac reserves Clinical expression low (< 5%) when dose < 400 mg/m 2 Clinical expression becomes greater as dose surpasses 450 mg/m 2 1.](http://images.slideplayer.com/1/232248/slides/slide_5.jpg "Bristow M, et al. Am J Med. 1978;65: Lefrak E, et al. Cancer. 1973;32: Minow R, et al. Cancer. 1977;39:")
6
Agents That Increase Anthracycline Cardiotoxicity Cyclophosphamide [1, 2] –Cardiotoxic at high doses –Increased cardiotoxicity when combined with doxorubicin Paclitaxel [3] May cause bradycardia, hypertension, or hypotension Increases the plasma concentration of doxorubicin Trastuzumab –Causes an inherent but largely transient contractile dysfunction –Increases expression of doxorubicin-induced cardiotoxicity as trastuzumab constitutes a sequential stress 1. Minow R, et al. Cancer. 1977;39:1397-1402. 2. Appelbaum F, et al. Lancet. 1976;1:58-62. 3. Gianni L, et al. Ann Oncol. 2001;12:1067-1073.
![Agents That Increase Anthracycline Cardiotoxicity Cyclophosphamide [1, 2] –Cardiotoxic at high doses –Increased cardiotoxicity when combined with doxorubicin Paclitaxel [3] May cause bradycardia, hypertension, or hypotension Increases the plasma concentration of doxorubicin Trastuzumab –Causes an inherent but largely transient contractile dysfunction –Increases expression of doxorubicin-induced cardiotoxicity as trastuzumab constitutes a sequential stress 1.](http://images.slideplayer.com/1/232248/slides/slide_6.jpg "Minow R, et al. Cancer. 1977;39: Appelbaum F, et al. Lancet. 1976;1: Gianni L, et al. Ann Oncol. 2001;12:")
7
NCIC CTG MA.5: LVEF Changes With Adjuvant CEF vs CMF Shepherd LE, et al. ASCO 2006. Abstract 522. Patients Experiencing Noted LVEF Decrease (%) < 10%10% to 20%> 20% 0 20 40 60 80 100 CEF (n = 139) CMF (n = 144) CEF (n = 291) CMF (n = 296) LVEF decrease: 0.7 8.5 90.8 74.9 20.1 5.0 91.0 8.3 0.7 80.7 18.6 0.7 6 Months 60 Months
 < 10%10% to 20%> 20% CEF (n = 139) CMF (n = 144) CEF (n = 291) CMF (n = 296) LVEF decrease: Months 60 Months.")
8
Anthracycline-Induced Cardiotoxicity Patients with anthracycline-induced cardiotoxicity can respond to treatment for chemotherapy- induced heart failure and other cardiac dysfunction, but the inherent damage persists [1] Cardiotoxicity that occurs early following anthracycline administration may be a predictor of later toxicity [2] –Heart failure is much more likely to be fatal if it occurs < 4 weeks from last doxorubicin dose 1. Haq M, et al. Cancer. 1985;56:1361-1365. 2. Minow R, et al. Cancer. 1977;39:1397- 1402. 3. Ali M, et al. Cancer. 1994;74:182-188.
![Anthracycline-Induced Cardiotoxicity Patients with anthracycline-induced cardiotoxicity can respond to treatment for chemotherapy- induced heart failure and other cardiac dysfunction, but the inherent damage persists [1] Cardiotoxicity that occurs early following anthracycline administration may be a predictor of later toxicity [2] –Heart failure is much more likely to be fatal if it occurs < 4 weeks from last doxorubicin dose 1.](http://images.slideplayer.com/1/232248/slides/slide_8.jpg "Haq M, et al. Cancer. 1985;56: Minow R, et al. Cancer. 1977;39: Ali M, et al. Cancer. 1994;74:")
9
Factors That Can Cause Sequential Stress Examples –Administration of different chemotherapeutics Retreatment with additional anthracyclines Trastuzumab following anthracyclines Other potentially cardiotoxic treatment modalities –Viral infections –Pregnancy Presentation will depend on extent of initial damage –Small sequential stress can be devastating to hearts that have sustained severe previous damage

14
Reducing Anthracycline Cardiotoxicity Limit cumulative dose [1] –Expression of cardiotoxicity unusual at cumulative doses < 300 mg/m 2 and 5% at 400 mg/m [2] Liposomal delivery systems [2-4] –Phase II trial suggested liposome-encapsulated doxorubicin combination therapy highly active against metastatic breast cancer with reduced cardiotoxicity 1. Ewer MS, et al. J Clin Oncol. 1984;2:112-117. 2. Valero V, et al. J Clin Oncol. 1999;17:1425-1434. 3. Harris L, et al. Cancer. 2002;94:25-36. 4. Batist G, et al. J Clin Oncol. 2001;19:1444-1454.
![Reducing Anthracycline Cardiotoxicity Limit cumulative dose [1] –Expression of cardiotoxicity unusual at cumulative doses < 300 mg/m 2 and 5% at 400 mg/m [2] Liposomal delivery systems [2-4] –Phase II trial suggested liposome-encapsulated doxorubicin combination therapy highly active against metastatic breast cancer with reduced cardiotoxicity 1.](http://images.slideplayer.com/1/232248/slides/slide_14.jpg "Ewer MS, et al. J Clin Oncol. 1984;2: Valero V, et al. J Clin Oncol. 1999;17: Harris L, et al. Cancer. 2002;94: Batist G, et al. J Clin Oncol. 2001;19:")
15
Reducing Anthracycline Cardiotoxicity Modification of dose schedule [1-3] –Weekly administration decreases cardiotoxicity and allows approximately 200 mg/m 2 more doxorubicin to be given than by standard schedule –Data implies doxorubicin cardiotoxicity relates to peak plasma levels Use continuous rather than rapid infusion [4] –Higher dose can be administered with less cardiotoxicity 1. Von Hoff D, et al. Am J Med. 1977;62:200-208. 2. Von Hoff D, et al. Ann Intern Med. 1979;91:710-717. 3. Chlebowski R, et al. Cancer Treat Rep. 1980;64:47-51. 4. Legha SS, et al. Ann Intern Med. 1979;91:847-852.
![Reducing Anthracycline Cardiotoxicity Modification of dose schedule [1-3] –Weekly administration decreases cardiotoxicity and allows approximately 200 mg/m 2 more doxorubicin to be given than by standard schedule –Data implies doxorubicin cardiotoxicity relates to peak plasma levels Use continuous rather than rapid infusion [4] –Higher dose can be administered with less cardiotoxicity 1.](http://images.slideplayer.com/1/232248/slides/slide_15.jpg "Von Hoff D, et al. Am J Med. 1977;62: Von Hoff D, et al. Ann Intern Med. 1979;91: Chlebowski R, et al. Cancer Treat Rep. 1980;64: Legha SS, et al. Ann Intern Med. 1979;91:")
16
1.Dexrazoxane may decrease cardiotoxicity when used at the initiation of doxorubicin-based chemotherapy in breast cancer 2.Beneficial effects are also seen when the initiation of dexrazoxane is delayed until a cumulative dose of 300 mg/m2 is reached. 3.Recommend against the routine use of dexrazoxane at the initiation of doxorubicin-based chemotherapy in patients with metastatic breast cancer. 4.It is suggested that the use of dexrazoxane be considered for patients with metastatic breast cancer who have received more than 300 mg/m2 of doxorubicin in the metastatic setting and who may benefit from continued doxorubicin- containing therapy. ASCO guidelines 2002

17
5.More than 300 mg/m2 in the adjuvant setting and initiating doxorubicin based chemotherapy in the metastatic setting: individualized. 6.Dexrazoxane in the adjuvant setting is not suggested outside of a clinical trial 7.Dexrazoxane at a ratio of 10:1 with the doxorubicin dose, given by slow IV push or short IV infusion, 15 to 30 minutes before doxorubicin or epirubicin administration. 8.A ratio of 10:1 with the epirubicin dose may be reasonable. However, it should be noted that the optimal dose ratio has not been determined. 9.Dexrazoxane in patients with cardiac risk factors or underlying cardiac disease: insufficient evidence ASCO guidelines 2002

18
These anthracycline-associated abnormalities and their related cardiac dysfunction constitute an entity that should now be considered type I CRC (Chemotherapy Related Cardiac damage). The differences between trastuzumab and anthracycline CRCD are now sufficiently clear to identify a variant form of myocardial dysfunction, type II CRCD, exemplified by trastuzumab cardiac effects. Ewer MS, Lippman SM; JCO 2005, 23 (13); 2900-2902
;")
21
Increasing evidence for the relative safety of rechallenge; additional data needed

25
Trastuzumab in Combination With Chemotherapy in MBC Patients Survival Time Overall trastuzumab impact on survival uncertain –Limited duration of follow-up ( 12 months) –Patients on CT alone allowed to enter trastuzumab extension protocol Preliminary analysisimproved 1-year survival –H + CT = 78% alive –CT alone = 67% alive Slamon DJ, et al. N Engl J Med. 2001;344:783-792.

26
1.Longer time to disease progression (median, 7.4 vs. 4.6 months; P<0.001) 2.Objective response (50 percent vs. 32 percent, P<0.001) 3.Longer duration of response (median, 9.1 vs. 6.1 months; P<0.001) 4.Lower rate of death at 1 year (22 percent vs. 33 percent, P=0.008) 5.Longer survival (median survival, 25.1 vs. 20.3 months; P=0.046) 6. 20 % risk of death Anthracycline + cyclophosphamide + trastuzumab 27 % Anthracycline+cyclophosphamide 8 % Paclitaxel+trastuzumab 13 % paclitaxel alone 1 % Slamon et al. N Engl J Med. 2001;344:783-792. Cardiac dysfunction
 2.Objective response (50 percent vs. 32 percent, P<0.001) 3.Longer duration of response (median, 9.1 vs. 6.1 months; P<0.001) 4.Lower rate of death at 1 year (22 percent vs. 33 percent, P=0.008) 5.Longer survival (median survival, 25.1 vs months; P=0.046) % risk of death Anthracycline + cyclophosphamide + trastuzumab 27 % Anthracycline+cyclophosphamide 8 % Paclitaxel+trastuzumab 13 % paclitaxel alone 1 % Slamon et al. N Engl J Med. 2001;344: Cardiac dysfunction.")
27
Slamon et al. N Engl J Med. 2001;344:783-792. Enrolled Response Rate (Improvement%) Response Duration (months, Improvement %) Time to Progression (months, Improvement %) H + CT23549 (-53%)9.3 (-58%)7.6 (-65%) CT234325.94.6 H + AC13852 (-20%)9.1 (-40%)8.1 (-33%) AC145436.56.1 H + T9242 (-163%)11.0 (-150%)6.9 (-130%) T96164.43.0 Comparison of Best Available w/Same Chemotherapy + Trastuzumab in MBC
 Response Duration (months, Improvement %) Time to Progression (months, Improvement %) H + CT23549 (-53%)9.3 (-58%)7.6 (-65%) CT H + AC13852 (-20%)9.1 (-40%)8.1 (-33%) AC H + T9242 (-163%)11.0 (-150%)6.9 (-130%) T Comparison of Best Available w/Same Chemotherapy + Trastuzumab in MBC.")
28
Trastuzumab in Combination With Chemotherapy in MBC Patients Cardiac Dysfunction Outcomes (CREC) H + ACACH + TT Cardiac dysfunction events, n (%) 39 (27)9 (7) 11 (12) 2 (1) Trastuzumab posttreatment events, n 145*61* Deaths, n4112 MBC4002 Cardiac0100 Pneumonia0010
 H + ACACH + TT Cardiac dysfunction events, n (%) 39 (27)9 (7) 11 (12) 2 (1) Trastuzumab posttreatment events, n 145*61* Deaths, n4112 MBC4002 Cardiac0100 Pneumonia0010")
29
Clinical Safety of Trastuzumab in MBC Patients Trastuzumab is generally well tolerated –Single agent –Combined with chemotherapy Most adverse events mild to moderate in severity –Infusion-associated symptoms, including fever and chills, primarily with first dose Serious adverse events infrequent Increased incidence of cardiac dysfunction, particularly when administered with anthracycline-based therapy Slamon DJ, et al. N Engl J Med. 2001;344:783-792.

30
Concomitant trastuzumab+anthracycline+cyclophosphamide 27% Paclitaxel and trastuzumab 13% Trastuzumab alone 3% to 7% Anthracycline plus cyclophosphamide 8% Paclitaxel alone 1% Seidman A et al J Clin Oncol 20:1215-1221. Trastuzumab is associated with an increased risk of CD, which is greatest in patients receiving concurrent anthracyclines Conclusion:

31
Product-limit estimates of cumulative doxorubicin dose to CD onset. CREC-diagnosed CD Seidman A et al J Clin Oncol 20:1215-1221.

36
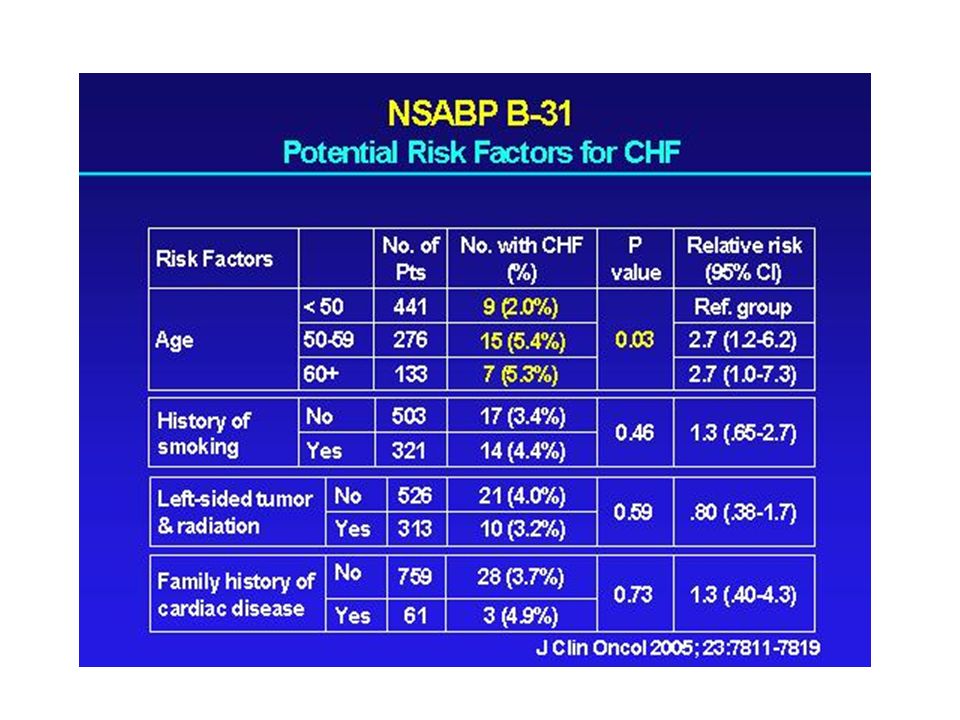
3,3% RISC RELATIU = 5,9 (95% CI 2,3-15,3; p<0,0001)
")
40
Three-Year Cumulative Incidence of CHF As a Function of Post-AC LVEF and Age in Evaluable B-31 Patients Receiving AC Followed by Paclitaxel Plus Trastuzumab

55
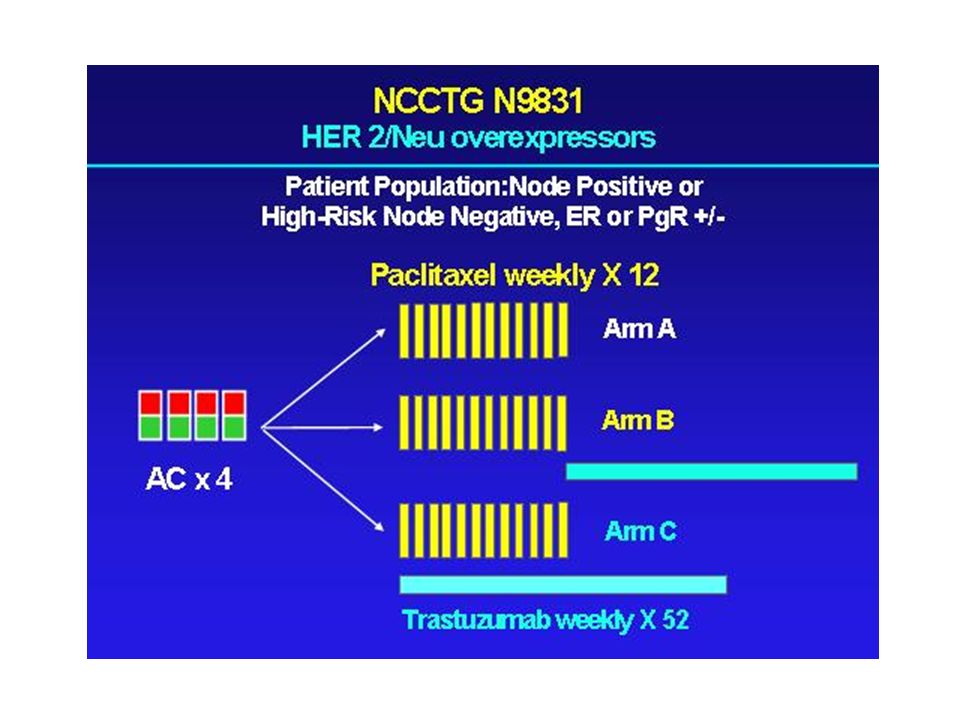
nine weekly trastuzumab infusions

56
Joensuu et al, NEJM 354; 2006

57
One patient had cardiac infarction and 3 had cardiac failure; none had received trastuzumab. LVEF were preserved in women who received trastuzumab: At least 1 measurements of ejection fraction 15% less than pretreatment –4 women treated with trastuzumab (3.5 percent) –7 who were not (6.0 percent) >10 %, resulting in an LVEF < 50 %, in 3 patients (none had received trastuzumab). Joensuu et al, NEJM 354; 2006
 –7 who were not (6.0 percent) >10 %, resulting in an LVEF < 50 %, in 3 patients (none had received trastuzumab). Joensuu et al, NEJM 354;")
58
None of the women treated with trastuzumab had cardiac failure, and unexpectedly, these women had slightly better maintenance of left ventricular ejection fraction than did those who did not receive the antibody. Administration of trastuzumab before FEC and radiotherapy as well as the small cumulative dose of epirubicin given may have contributed to the preservation of cardiac function. Joensuu et al, NEJM 354; 2006

59
LVEF are more sustained with AC T and AC TH (> 550 days at last follow-up) than was previously thought Coamplification of the topoisomerase II alpha gene –Occurs in ~ 35% of HER2-positive patients and may confer a therapeutic advantage to anthracycline-based trastuzumab combination regimens Not coamplified for topoisomerase II alpha –Approximately ~ 65% of HER2-positive patients do not appear to have this same benefit and may be ideal candidates for efficacious, nonanthracycline-based regimens, thus avoiding potential cardiac toxicity Slamon D. SABCS 2005. Observacions

60
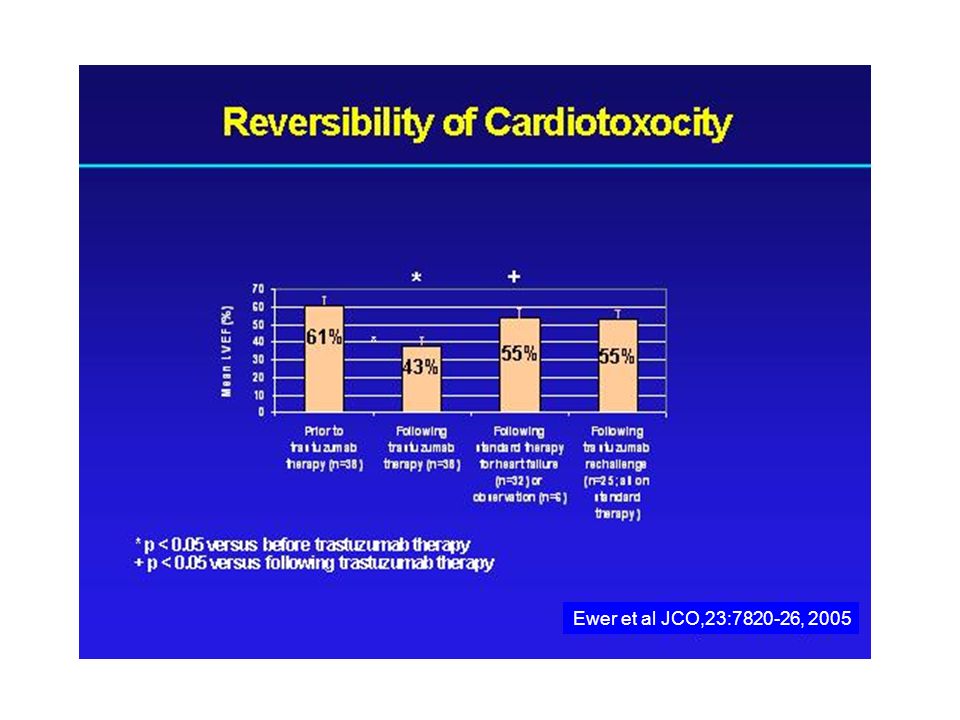
LVEF decreased to 0.43 after trastuzumab (P.0001). After withdrawal of trastuzumab, the LVEF increased to 0.56 Mean time to recovery of LVEF =1.5 months with medical treatment in 32 (84%) without treatment in six patients (16%). Conclusion Reintroducing trastuzumab may be appropriate for some individuals who previously have experienced trastuzumab- related cardiac dysfunction. Patients who develop cardiotoxicity while receiving trastuzumab therapy generally improve on removal of the agent. 22 patients (88%) did not. 25 re-treated 3 (12%) left ventricular dysfunction Ewer et al JCO,23:7820-26, 2005
 without treatment in six patients (16%). Conclusion Reintroducing trastuzumab may be appropriate for some individuals who previously have experienced trastuzumab- related cardiac dysfunction. Patients who develop cardiotoxicity while receiving trastuzumab therapy generally improve on removal of the agent. 22 patients (88%) did not. 25 re-treated 3 (12%) left ventricular dysfunction Ewer et al JCO,23: ,")
62
LVEF Improves With Therapy for Heart Failure Durand JB, et al. J Clin Oncol. 2005;23:7820-7826. 90 80 70 60 50 40 30 20 10 0 Mean LVEF (%) Following Trastuzumab Therapy (n = 35) Prior to Trastuzumab Therapy (n = 35) Following Standard Therapy for Heart Failure (n = 33) Following Trastuzumab Rechallenge (n = 25)
 Following Trastuzumab Therapy (n = 35) Prior to Trastuzumab Therapy (n = 35) Following Standard Therapy for Heart Failure (n = 33) Following Trastuzumab Rechallenge (n = 25).")
65
Strategies to Reduce Cardiovascular Toxicity and Manage Complications Trastuzumab-related cardiomyopathy seems to be largely reversible [1] –Cease drug administration –Treat cardiac risk factors –Administer appropriate therapy for LV dysfunction ACE inhibitors and beta-blockers should be aggressively administered The role of ongoing treatment of trastuzumab- associated cardiotoxicity is uncertain 1. Ewer MS, et al. J Clin Oncol. 2005;23:7820-7826.
![Strategies to Reduce Cardiovascular Toxicity and Manage Complications Trastuzumab-related cardiomyopathy seems to be largely reversible [1] –Cease drug administration –Treat cardiac risk factors –Administer appropriate therapy for LV dysfunction ACE inhibitors and beta-blockers should be aggressively administered The role of ongoing treatment of trastuzumab- associated cardiotoxicity is uncertain 1.](http://images.slideplayer.com/1/232248/slides/slide_65.jpg "Ewer MS, et al. J Clin Oncol. 2005;23:")
78
NCI Guidelines: Common Toxicity Criteria, 2001, 1-12 GRADE 12345 LV Systolic Dysfunct ion Asympto maticLVE F 50% to 60%; SF < 24% to 30% Asympto maticLVE F 40-50%: SF < 15% to 24% Symptomati c CHF responsive to intervention; EF < 20% to 40% SF < 15% Refractory CHF or LVEF < 20%: interventio n such as VAD, ventricular reduction surgery, or heart transplant indicated Deat h NCI Guidelines: Common Toxicity Criteria. 2001; 1-12.

79
Cancer vs Heart Failure CANCER Bad outcome Bad way to die HEART FAILURE Bad outcome –Median survival class IV heart failure: 1.0-1.5 yrs Bad way to die –80% of HF deaths accompanied by severe symptoms –Pain, anorexia, constipation common –Anxiety and insomnia may be aggravated by high central dopamine levels

Similar presentations












































 patients Policy.>")







 Chemoimmunotherapy and Maintenance Lenalidomide in Relapsed/Refractory (R/R) Chronic Lymphocytic Leukemia (CLL) and Small.>")





