Download presentation
Presentation is loading. Please wait.

1
Management of HER2 Over-Expressed Breast Cancer in the Adjuvant, Neoadjuvant, and Metastatic settings Christy A Russell, MD Keck School of Medicine University of Southern California

2
Metastatic Breast Cancer

3
Chemotherapy Plus Trastuzumab in Metastatic Disease
Slamon et al n = 469 Marty et al n = 186 Treatment Arms AC or T* vs AC or T→H† Docetaxel Docetaxel →H† Time to Disease Progression (mos) 4.6 7.4 P value 6.1 11.7 < 0.001 0.0001 Response Rate 32% 50% 34% 61% 0.0002 Median Overall Survival (mos) 20 25 0.046 23 31 0.0325 *T = paclitaxel; †H = trastuzumab. Hudis CA. N Engl J Med. 2007;357:36-51; Slamon DJ, et al. N Engl J Med. 2001;344: ; Marty M, et al. J Clin Oncol. 2005;23:
 P value < Response Rate. 32% 50% 34% 61% Median Overall Survival (mos) *T = paclitaxel; †H = trastuzumab. Hudis CA. N Engl J Med. 2007;357:36-51; Slamon DJ, et al. N Engl J Med. 2001;344: ; Marty M, et al. J Clin Oncol. 2005;23:")
4
Anti-HER2 Targeted Therapy: Pertuzumab

5
Pertuzumab-HER2 Complex Trastuzumab-HER2 Complex
Pertuzumab and Trastuzumab Bind to Distinct Extracellular HER2 Epitopes Pertuzumab-HER2 Complex Trastuzumab-HER2 Complex Pertuzumab Dimerization domain I I II II III III Trastuzumab IV IV ADCC, antibody-dependent cell-mediated cytotoxicity. Like trastuzumab, pertuzumab was among the first-line anti-HER2 antibodies tested preclinically in vitro and in vivo that showed that antibodies against the HER2 extracellular domain could growth-inhibit these tumors preclinically. Although they are both HER2-targeting agents, pertuzumab and trastuzumab have some distinct differences, listed here. The most important difference is that pertuzumab binds to a different epitope in the HER2 extracellular domain that inhibits the HER2 dimerization with other HER family receptors. In particular, pertuzumab more strongly inhibits the most effective signaling dimerization partner complex, HER2 plus HER3. Inhibits HER2 dimerization with other HER family receptors (particularly HER3) Activates ADCC Inhibits multiple HER-mediated signaling pathways Activates ADCC Inhibits HER-mediated signaling pathways Prevents HER2 domain cleavage Hubbard SR. Cancer Cell. 2005;7:
 Activates ADCC. Inhibits multiple HER-mediated signaling pathways. Activates ADCC. Inhibits HER-mediated signaling pathways. Prevents HER2 domain cleavage. Hubbard SR. Cancer Cell. 2005;7:")
6
Trastuzumab and Pertuzumab Bind to Different Regions on HER2 and May Have Synergistic Activity
Subdomain IV of HER2 Dimerization domain of HER2 Trastuzumab does not inhibit HER2 dimerization, thus blocking HER2:HER3 Trastuzumab prevents HER2 receptor shedding Trastuzumab blocks HER2 signaling and flags cells for destruction by the immune system Pertuzumab inhibits HER2 from forming dimer pairs Flags cells for destruction by the immune system Pertuzumab does not prevent HER2 receptor shedding 6

7
CLEOPATRA Study Design
Docetaxel (≥ 6 cycles recommended) Centrally confirmed HER2-positive locally recurrent, unresectable or MBC ≤ 1 hormonal regimen for MBC Prior (neo)adjuvant systemic Rx, including trastuzumab and/or taxane allowed if followed by DFS ≥ 12 mos Baseline LVEF ≥ 50%; no CHF or LVEF < 50% during or after previous trastuzumab N = 406 Trastuzumab Placebo R 1:1 Docetaxel (≥ 6 cycles recommended) Trastuzumab N = 402 Pertuzumab Primary endpoint: Independently assessed PFS Baselga J, et al. N Engl J Med. 2012;366:
 Centrally confirmed HER2-positive locally recurrent, unresectable or MBC. ≤ 1 hormonal regimen for MBC. Prior (neo)adjuvant systemic Rx, including trastuzumab and/or taxane allowed if followed by DFS ≥ 12 mos. Baseline LVEF ≥ 50%; no CHF or LVEF < 50% during or after previous trastuzumab. N = 406. Trastuzumab. Placebo. R. 1:1. Docetaxel (≥ 6 cycles recommended) Trastuzumab. N = 402. Pertuzumab. Primary endpoint: Independently assessed PFS. Baselga J, et al. N Engl J Med. 2012;366:")
8
CLEOPATRA: PFS Assessed at an IRF
100 Pertuzumab (median: 18.5 mos) Control (median: 12.4 mos) 90 80 70 60 PFS (%) 50 40 HR: 0.62 (95% CI: ; P < .001) 30 20 10 5 10 15 20 25 30 35 40 Mos Pts at Risk, n Pertuzumab Control 139 93 83 42 32 17 10 7 0 0 0 0 Baselga J, et al. N Engl J Med. 2012;366:
 Control (median: 12.4 mos) PFS (%) HR: 0.62 (95% CI: ; P < .001) Mos. Pts at Risk, n Pertuzumab Control Baselga J, et al. N Engl J Med. 2012;366:")
9
Adding Pertuzumab to Trastuzumab and Chemotherapy

10
Trastuzumab + Docetaxel + Pertuzumab Trastuzumab + Docetaxel + Placebo
CLEOPATRA: Safety Adverse Events, % Trastuzumab + Docetaxel + Pertuzumab (n = 407) Trastuzumab + Docetaxel + Placebo (n = 397) All Grades Grade 3/4 Diarrhea 66.8 7.9 46.3 5.0 Alopecia 60.9 NR 60.5 Neutropenia 52.8 48.9 49.6 45.8 Nausea 42.3 41.6 Fatigue 37.6 2.2 36.8 3.3 Rash 33.7 24.2 Decreased appetite 29.2 26.4 Mucosal inflammation 27.8 19.9 Asthenia 26.0 2.5 30.2 1.5 Peripheral edema 23.1 30.0 Constipation 15.0 24.9 Febrile neutropenia 13.8 7.6 Dry skin 10.6 4.3 Leukopenia 12.3 14.6 Baselga J, et al. N Engl J Med. 2012;366:
 Trastuzumab + Docetaxel + Placebo. (n = 397) All Grades. Grade 3/4. Diarrhea Alopecia NR Neutropenia Nausea Fatigue Rash Decreased appetite Mucosal inflammation Asthenia Peripheral edema Constipation Febrile neutropenia Dry skin Leukopenia Baselga J, et al. N Engl J Med. 2012;366:")
11
NCCN: First-line Treatment of HER2+ MBC With No Previous Trastuzumab Exposure
Preferred regimens Docetaxel + trastuzumab + pertuzumab (category 1) Paclitaxel + trastuzumab + pertuzumab Other regimens Trastuzumab with: Paclitaxel ± carboplatin Docetaxel Vinorelbine Capecitabine NCCN. Clinical practice guidelines in oncology: breast cancer. V
 Paclitaxel + trastuzumab + pertuzumab. Other regimens. Trastuzumab with: Paclitaxel ± carboplatin. Docetaxel. Vinorelbine. Capecitabine. NCCN. Clinical practice guidelines in oncology: breast cancer. V")
12
NCCN: Treatment of HER2+ MBC Beyond First Line With Previous Trastuzumab Exposure
Preferred agents Ado-trastuzumab emtansine (T-DM1) Other agents Lapatinib + capecitabine Trastuzumab + capecitabine Trastuzumab + lapatinib (without cytotoxic therapy) Trastuzumab + other agents NCCN. Clinical practice guidelines in oncology: breast cancer. V
 Other agents. Lapatinib + capecitabine. Trastuzumab + capecitabine. Trastuzumab + lapatinib (without cytotoxic therapy) Trastuzumab + other agents. NCCN. Clinical practice guidelines in oncology: breast cancer. V")
13
Second-line and Further Therapy TDM-1

14
Trastuzumab/Emtansine: Novel Antibody–Drug Conjugate
Monoclonal antibody: trastuzumab Target expression: HER2 Trastuzumab Highly potent cytotoxic agent Cytotoxic agent: emtansine (DM1) MCC DM1 Systemically stable Linker: SMCC T-DM1 Average drug:antibody ratio ≅ 3.5:1
 MCC. DM1. Systemically stable. Linker: SMCC. T-DM1 Average drug:antibody ratio ≅ 3.5:1.")
15
EMILIA Phase III Study: T-DM1 vs Lapatinib/Capecitabine in HER2+ MBC
Stratified by world region, number of previous chemotherapy regimens for MBC or unresectable locally advanced breast cancer, presence of visceral disease T-DM1 3.6 mg/kg by IV every 3 wks (n = 495) Patients with HER2-positive locally advanced or MBC* (N = 980) PD Capecitabine 1000 mg/m2 orally twice daily on Days 1-14, every 3 wks + Lapatinib 1250 mg/day orally continuously (n = 496) *All pts received previous taxane and trastuzumab Primary endpoint: PFS by IRF, OS, safety Secondary endpoints: QoL (FACT B), DOR, PFS by investigator assessment Verma S, et al. NEJM 2012;367:
 Patients with HER2-positive locally advanced or MBC* (N = 980) PD. Capecitabine 1000 mg/m2 orally twice daily on Days 1-14, every 3 wks + Lapatinib 1250 mg/day orally continuously (n = 496) *All pts received previous. taxane and trastuzumab. Primary endpoint: PFS by IRF, OS, safety. Secondary endpoints: QoL (FACT B), DOR, PFS by investigator assessment. Verma S, et al. NEJM 2012;367:")
16
T-DM1 vs Lapatinib/Capecitabine in HER2+ MBC (EMILIA): PFS
Median, Mos Events, n 1.0 Capecitabine/lapatinib T-DM1 304 265 0.8 Stratified HR: (95% CI: ; P < .0001) 0.6 Proportion Progression Free 0.4 T-DM1 Capecitabine/ lapatinib 0.2 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 Mos Verma S, et al. NEJM 2012;367:
 0.6. Proportion Progression Free T-DM1. Capecitabine/ lapatinib Mos. Verma S, et al. NEJM 2012;367:")
17
OS: Second Interim Analysis
Median No. of Mos No. of Events 100 85.2% (95% CI: ) Lapatinib-capecitabine T-DM1 Stratified HR: 0.68 (95% CI: ; P < .001) 80 64.7% (95% CI: ) Efficacy stopping boundary P = or HR: 0.73 60 78.4% (95% CI: ) T-DM1 OS (%) 40 51.8% (95% CI: ) Lapatinib-capecitabine 20 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36 Pts at Risk, n Lapatinib- capecitabine T-DM1 Mos 63 86 45 62 27 38 17 28 7 13 4 5 Data cutoff July 31, 2012; median follow-up: 18.6 mos. Verma S, et al. N Engl J Med. 2012;367:
 Lapatinib-capecitabine T-DM1. Stratified HR: 0.68 (95% CI: ; P < .001) % (95% CI: ) Efficacy stopping boundary P = or HR: % (95% CI: ) T-DM1. OS (%) % (95% CI: ) Lapatinib-capecitabine Pts at Risk, n Lapatinib- capecitabine T-DM1. Mos Data cutoff July 31, 2012; median follow-up: 18.6 mos. Verma S, et al. N Engl J Med. 2012;367:")
18
T-DM1 vs Lapatinib/Capecitabine in HER2+ MBC (EMILIA): Adverse Events
Capecitabine + Lapatinib (n = 488) All Grades Grades ≥ 3 Nonhematologic Diarrhea 23.3 1.6 79.7 20.7 Hand-foot syndrome 1.2 58.0 16.4 Vomiting 19.0 0.8 29.3 4.5 Hypokalemia 8.6 2.2 4.1 Fatigue 35.1 2.4 27.9 3.5 Nausea 39.2 44.7 2.5 Mucosal inflammation 6.7 0.2 19.1 2.3 Increased AST 22.4 4.3 9.4 Increased ALT 16.9 2.9 8.8 1.4 Hematologic Neutropenia 5.9 2.0 Febrile neutropenia 1.0 Anemia 10.4 2.7 8.0 Thrombocytopenia 28.0 12.8 Verma S, et al. NEJM 2012;367:
 All Grades. Grades ≥ 3. Nonhematologic. Diarrhea Hand-foot syndrome Vomiting Hypokalemia Fatigue Nausea Mucosal inflammation Increased AST Increased ALT Hematologic. Neutropenia Febrile neutropenia Anemia Thrombocytopenia Verma S, et al. NEJM 2012;367:")
19
Ongoing Clinical Trials for Metastatic Breast Cancer

20
Phase III MARIANNE Study: T-DM1 ± Pertuzumab in HER2+ MBC
PD Trastuzumab + Taxane (n = 364) Patients with HER2+, previously untreated MBC (N = 1092) T-DM1 + Pertuzumab (n = 364) T-DM1 + Placebo (n = 364) Primary endpoints: PFS as assessed by IRF, AEs Superiority design with a noninferiority analyses Interim futility analysis: option to drop experimental arm Secondary endpoints: OS, TTF by IRF, ORR, CBR, DOR ClinicalTrials.gov. NCT 20
 Patients with HER2+, previously untreated MBC. (N = 1092) T-DM1 + Pertuzumab. (n = 364) T-DM1 + Placebo. (n = 364) Primary endpoints: PFS as assessed by IRF, AEs. Superiority design with a noninferiority analyses. Interim futility analysis: option to drop experimental arm. Secondary endpoints: OS, TTF by IRF, ORR, CBR, DOR. ClinicalTrials.gov. NCT")
21
Phase III Trial of Everolimus in Combination With Trastuzumab and Paclitaxel as Frontline Therapy for HER2+ MBC (BOLERO-1) RANDOMIZATION HER+ MBC No prior anthracycline/taxane-based chemotherapy in the metastatic setting (N = 719) Everolim us 10 mg PO + Paclitaxel 80 mg/m2 qwk d 1, 8, 15 + Trastuzu mab 2 mg/kg d 1, 8, 15, 22 Placebo + Primary Endpoint: PFS Available at:
 Everolim us 10 mg PO + Paclitaxel 80 mg/m2 qwk d 1, 8, Trastuzu mab 2 mg/kg d 1, 8, 15, 22. Placebo + Primary Endpoint: PFS. Available at:")
22
Other Trials With Completed or Ongoing Accrual in MBC
T-DM1 vs investigator’s choice (TH3RESA) Addition of pertuzumab to vinorelbine and trastuzumab (VELVET)
 Addition of pertuzumab to vinorelbine and trastuzumab (VELVET)")
23
Neoadjuvant Therapy

24
Trastuzumab + Lapatinib Trials

25
pCR Rates (breast and LN) with Trastuzumab (H) and/or Lapatinib (L)
Study/Neoadjuvant Regimen Total pCR Trastuzumab Lapatinib H + L NeoALTTO1 (6 week H and/or L (WP) x 12 plus H and/or L) N=455 27.6% 20.0% 46.8% NSABP B-412 (AC x 4 WP x 12 plus H and/or L) N=519 49.4% 47.4% 60.2% CALGB (WP x 16 plus H and/or L) N=299 43% 29% 52% CHER-LOB4 (WP x 12 FEC x 4 plus H and or L throughout N=121 25% 26.3% 46.7% WP=weekly paclitaxel; AC=doxorubicin/cyclophosphamide; FEC=5-FU, epirubicin, cyclophosphamide Baselga J, et al. Lancet 2012;18: Robidoux, et al Lancet Oncol; pub online Oct 4, 2013 3. Carey, et al. ASCO 2013, abst Guarneri, et al. JCO 2012;31.
 x 12 plus H and/or L) N= % 20.0% 46.8% NSABP B-412. (AC x 4 WP x 12 plus H and/or L) N= % 47.4% 60.2% CALGB (WP x 16 plus H and/or L) N= % 29% 52% CHER-LOB4. (WP x 12 FEC x 4 plus H and or L throughout. N= % 26.3% 46.7% WP=weekly paclitaxel; AC=doxorubicin/cyclophosphamide; FEC=5-FU, epirubicin, cyclophosphamide. Baselga J, et al. Lancet 2012;18: Robidoux, et al Lancet Oncol; pub online Oct 4, Carey, et al. ASCO 2013, abst Guarneri, et al. JCO 2012;31.")
32
CALGB Schema Carey L, et al ASCO 2013 Abstr # 500

33
Breast pCR Rate by HR Status
HR+ (N=173) HR- (N=123) Carey L, et al ASCO 2013 Abstr # 500
 HR- (N=123) Carey L, et al ASCO 2013 Abstr # 500.")
34
pCR Rate by Arm and Subtype
Basal-like (N=11) HER2-E (N=52) Lum-A (N=51) Lum-B (N=35) Carey L, et al ASCO 2013 Abstr # 500
 HER2-E. (N=52) Lum-A. (N=51) Lum-B. (N=35) Carey L, et al ASCO 2013 Abstr # 500.")
35
Neoadjuvant Trastuzumab + Pertuzumab Trials

36
NeoSphere: study design
TH (n=107) docetaxel + trastuzumab S U R G E Y FEC q3w x 3 trastuzumab q3w cycles 5–17 trastuzumab q3w cycles 5–21 Patients with operable or locally advanced /inflammatory* HER2-positive BC Chemo-naïve & primary tumors >2cm (N=417) THP (n=107) docetaxel + trastuzumab + pertuzumab HP (n=107) trastuzumab + pertuzumab docetaxel q3w x 4→FEC q3w x 3 trastuzumab q3w cycles 5–17 TP (n=96) docetaxel + pertuzumab Study dosing: q3w x 4 BC, breast cancer; FEC, 5-fluorouracil, epirubicin and cyclophosphamide *Locally advanced=T2–3, N2–3, M0 or T4a–c, any N, M0; operable=T2–3, N0–1, M0; inflammatory = T4d, any N, M0 H, trastuzumab; P, pertuzumab; T, docetaxel 3
 docetaxel + trastuzumab. S. U. R. G. E. Y. FEC q3w x 3. trastuzumab q3w cycles 5–17. trastuzumab q3w cycles 5–21. Patients with operable or locally advanced /inflammatory* HER2-positive BC. Chemo-naïve & primary tumors >2cm (N=417) THP (n=107) docetaxel + trastuzumab + pertuzumab. HP (n=107) trastuzumab + pertuzumab. docetaxel q3w x 4→FEC q3w x 3. trastuzumab q3w cycles 5–17. TP (n=96) docetaxel + pertuzumab. Study dosing: q3w x 4. BC, breast cancer; FEC, 5-fluorouracil, epirubicin and cyclophosphamide *Locally advanced=T2–3, N2–3, M0 or T4a–c, any N, M0; operable=T2–3, N0–1, M0; inflammatory = T4d, any N, M0 H, trastuzumab; P, pertuzumab; T, docetaxel. 3.")
37
NeoSphere pCR rates: ITT population summary
50 p = 0.003 40 pCR, % 95% CI 45.8 30 20 29.0 24.0 10 16.8 H, trastuzumab; P, pertuzumab; T, docetaxel TH THP HP TP

38
NeoSphere: pCR and Hormone Receptors Status
Gianni L, et al. Cancer Res. 2010;70 (24 Suppl): Abstract [S3-2].
: Abstract [S3-2].")
39
NeoSphere Trial: pCR in Breast and Nodes
HR+ HR- n %pCR Trastuzumab + docetaxel 50 12% 57 29.8% Trastuzumab + docetaxel + pertuzumab 22% 54.4% Trastuzumab + pertuzumab 51 2% 55 20% Docetaxel + pertuzumab 46 8.7% 26%

40
TRYPHAENA Study: TCH + pertuzumab
225 patients with locally advanced, operable, or inflammatory breast cancer (T2-T4d) Trial was designed to assess cardiac safety Schneeweiss, et al. Ann Oncol 2013;24
 Trial was designed to assess cardiac safety. Schneeweiss, et al. Ann Oncol 2013;24.")
41
TRYPHAENA pCR Neoadjuvant Regimen HR+ HR- %pCR TCH + Pertuzumab (76)
47.5% 81.1% FEC (75) P + T + Docetaxel 45.7% 62.5% Pertuzumab + Trastuzumab 41.0% 73.5% FEC (72) Docetaxel Schneeweiss, et al. Ann Oncol 2013;24
 P + T + Docetaxel. 45.7% 62.5% Pertuzumab + Trastuzumab. 41.0% 73.5% FEC (72) Docetaxel. Schneeweiss, et al. Ann Oncol 2013;24.")
42
FDA Approval in Neoadjuvant Setting
Pertuzumab is indicated for use in combination with trastuzumab and docetaxel for the neoadjuvant treatment of patients with HER2+, locally advanced, inflammatory, or early stage breast cancer (either >2 cm or node positive) as part of a complete treatment regimen for early breast cancer. This indication is based on demonstration of an improvement in pCR rate. No data are available demonstrating improvement in EFS or OS. Limitations of Use: The safety of pertuzumab as part of a doxorubicin-containing regimen has not been established. The safety of pertuzumab administered for > 6 cycles for early breast cancer has not been established.
 as part of a complete treatment regimen for early breast cancer. This indication is based on demonstration of an improvement in pCR rate. No data are available demonstrating improvement in EFS or OS. Limitations of Use: The safety of pertuzumab as part of a doxorubicin-containing regimen has not been established. The safety of pertuzumab administered for > 6 cycles for early breast cancer has not been established.")
43
Adjuvant HER-2 Targeted Therapy

44
NCCTG N9831 Trial Incorporating Trastuzumab in Adjuvant Therapy
Group A AC T R A N D O M I Z E Group B HER2 positive (FISH+ or IHC 3+) AC T H Group C n=3,505 AC T H = AC (doxorubicin/cyclophosphamide 60/600 mg/m2 q3w × 4) = T (paclitaxel 80 mg/m2/wk × 12) = H (trastuzumab 4 mg/kg loading dose + 2 mg/kg/wk × 51)
 AC. T. H. Group C. n=3,505. AC. T. H. = AC (doxorubicin/cyclophosphamide 60/600 mg/m2 q3w × 4) = T (paclitaxel 80 mg/m2/wk × 12) = H (trastuzumab 4 mg/kg loading dose + 2 mg/kg/wk × 51)")
45
NSABP B-31 Trial Incorporating Trastuzumab in Adjuvant Therapy
Group 1 AC T R A N D O M I Z E Node positive HER2 positive (FISH+ or IHC 3+) Group 2 N=2,006 AC T H = AC (doxorubicin/cyclophosphamide 60/600 mg/m2 q3w × 4) = T (paclitaxel 175 mg/m2 q3w × 4 or 80 mg/m2/wk × 12) = H (trastuzumab 4 mg/kg loading dose + 2 mg/kg/wk × 51)
 Group 2. N=2,006. AC. T. H. = AC (doxorubicin/cyclophosphamide 60/600 mg/m2 q3w × 4) = T (paclitaxel 175 mg/m2 q3w × 4 or 80 mg/m2/wk × 12) = H (trastuzumab 4 mg/kg loading dose + 2 mg/kg/wk × 51)")
46
Joint Analysis of HER2+ Adjuvant Trials 2 Arms of N9831 + B-31
Control Group (n=1,979): AC T AC T N9831 Group A AC T B-31 Group 1 Trastuzumab Group (n=1,989): AC T+H AC T N9831 Group C H AC T B-31 Group 2 H = AC (doxorubicin/cyclophosphamide 60/600 mg/m2 q3w × 4) = T (paclitaxel 80 mg/m2/wk × 12) = T (paclitaxel 175 mg/m2 q3w × 4 or 80 mg/m2/wk × 12) = H (trastuzumab 4 mg/kg loading dose + 2 mg/kg/wk × 51)
: AC T. AC. T. N9831 Group A. AC. T. B-31 Group 1. Trastuzumab Group (n=1,989): AC T+H. AC. T. N9831 Group C. H. AC. T. B-31 Group 2. H. = AC (doxorubicin/cyclophosphamide 60/600 mg/m2 q3w × 4) = T (paclitaxel 80 mg/m2/wk × 12) = T (paclitaxel 175 mg/m2 q3w × 4 or 80 mg/m2/wk × 12) = H (trastuzumab 4 mg/kg loading dose + 2 mg/kg/wk × 51)")
47
Kaplan-Meier estimates of (A) event-free survival and (B) overall survival.
HR 0.52 P < .001 HR 0.61 Perez E A et al. JCO 2011;29: ©2011 by American Society of Clinical Oncology

48
Events Per Year From Randomization
Perez E A et al. JCO 2011;29: ©2011 by American Society of Clinical Oncology

49
Breast Cancer International Research Group (BCIRG) 006 Trial: Treatment Schema
D O M I Z E AC T (n=1073) SURGERY HER2-positive tumor (FISH+); node-positive or high-risk node-negative disease AC TH (n=1074) 52 weeks TCH (n=1075) 52 weeks Endpoints 1°: Disease-free survival (DFS) 2°: Overall survival, toxicity, pathologic and molecular markers = H = Trastuzumab 4 mg/kg loading dose = H = Trastuzumab 2 mg/kg qw = H = Trastuzumab 6 mg/kg q3w = AC = doxorubicin/cyclophosphamide 60/600 mg/m2 q3w = T = docetaxel 100 mg/m2 q3w = TC = docetaxel 75 mg/m2/carboplatin target AUC 6 mg/mL· min Radiation therapy and/or hormonal therapy may be given after completion of chemotherapy if indicated Slamon et al. NEJM 2011;365. Herceptin® (trastuzumab) PI. March 2009.
 SURGERY. HER2-positive tumor (FISH+); node-positive or high-risk node-negative disease. AC TH (n=1074) 52 weeks. TCH (n=1075) 52 weeks. Endpoints. 1°: Disease-free survival (DFS) 2°: Overall survival, toxicity, pathologic and molecular markers. = H = Trastuzumab 4 mg/kg loading dose. = H = Trastuzumab 2 mg/kg qw. = H = Trastuzumab 6 mg/kg q3w. = AC = doxorubicin/cyclophosphamide 60/600 mg/m2 q3w. = T = docetaxel 100 mg/m2 q3w. = TC = docetaxel 75 mg/m2/carboplatin target AUC 6 mg/mL· min. Radiation therapy and/or hormonal therapy may be given after completion of chemotherapy if indicated. Slamon et al. NEJM 2011;365. Herceptin® (trastuzumab) PI. March")
50
Disease-Free Survival Among all Study Patients
DFS AC-TH vs AC-T HR .64 p<0.001 TCH vs AC-T HR .75 p=0.04 OS AC-TH vs AC-T HR .63 p<0.001 TCH vs AC-T HR .77 p=0.04

51
Overall Survival Overall Survival

52
Trials to be Reported

53
ALTTO Trial Design Trastuzumab 8 mg/kg IV (loading dose)* 6 mg/kg every 3 wks for 1 yr Paclitaxel 80 mg/m2 IV once wkly x 12 Women with centrally determined HER2-positive invasive breast cancer (N = 8381 accrued) Surgery, adjuvant anthracycline-based therapy for 4 cycles; LVEF ≥ 50 6-week wash-out Trastuzumab 4 mg/kg IV (loading dose) 2 mg/kg once wkly x 11 Paclitaxel 80 mg/m2 IV once wkly x 12 Lapatinib 1500 mg orally once daily x 34 wks Lapatinib 1500 mg/kg orally once daily x 51 wks Paclitaxel 80 mg/m2 IV once wkly x 12 (This arm closed in 9/2011 due to inferiority) *For concomitant dosing with paclitaxel, trastuzumab will be given on a weekly schedule (4 mg/kg IV loading dose followed by 2 mg/kg IV weekly). Trastuzumab will revert to the 3-weekly schedule (6 mg/kg without loading dose). Trastuzumab 8 mg/kg (loading dose) 6 mg/kg every 3 wks for 1 yr Lapatinib 1000 mg orally once daily x 51 wks Paclitaxel 80 mg/m2 IV once wkly x 12
 Surgery, adjuvant anthracycline-based therapy for 4 cycles; LVEF ≥ week wash-out. Trastuzumab 4 mg/kg IV (loading dose) 2 mg/kg once wkly x 11 Paclitaxel 80 mg/m2 IV once wkly x 12. Lapatinib mg orally once daily x 34 wks. Lapatinib 1500 mg/kg orally once daily x 51 wks Paclitaxel 80 mg/m2 IV once wkly x 12. (This arm closed in 9/2011 due to inferiority) *For concomitant dosing with paclitaxel, trastuzumab will be given on a weekly schedule (4 mg/kg IV loading dose followed by 2 mg/kg IV weekly). Trastuzumab will revert to the 3-weekly schedule (6 mg/kg without loading dose). Trastuzumab 8 mg/kg (loading dose) 6 mg/kg every 3 wks for 1 yr. Lapatinib 1000 mg orally once daily x 51 wks Paclitaxel 80 mg/m2 IV once wkly x 12.")
54
APHINITY Chemotherapy + trastuzumab and pertuzumab
S U R G E R Y R A N D O M I Z T F O L W U P 10 Y R S Chemotherapy + trastuzumab and pertuzumab Anthracycline or non-anthracycline–based chemotherapy allowed N = 3806 N = 3806 Central confirmation of HER2 status Chemotherapy + trastuzumab and placebo Anthracycline or non-anthracycline–based chemotherapy allowed Randomization within 7 wks of surgery Start treatment within 1 wk Anti-HER2 therapy for a total of 1 yr (52 wks) Radiotherapy and/or endocrine therapy may be started at the end of adjuvant chemotherapy ClinicalTrials.gov Identifier: NCT
 Radiotherapy and/or endocrine therapy may be started at the end of adjuvant chemotherapy. ClinicalTrials.gov Identifier: NCT")
55
Conclusions Trastuzumab in addition to chemotherapy remains the standard for all “high-risk” HER-2+ early breast cancer. Controversies exist regarding the following: Use of anthracyclines Definition of “high-risk” Role of additional biologic agents to trastuzumab

56
“Low-Risk” HER2+ Breast Cancer

57
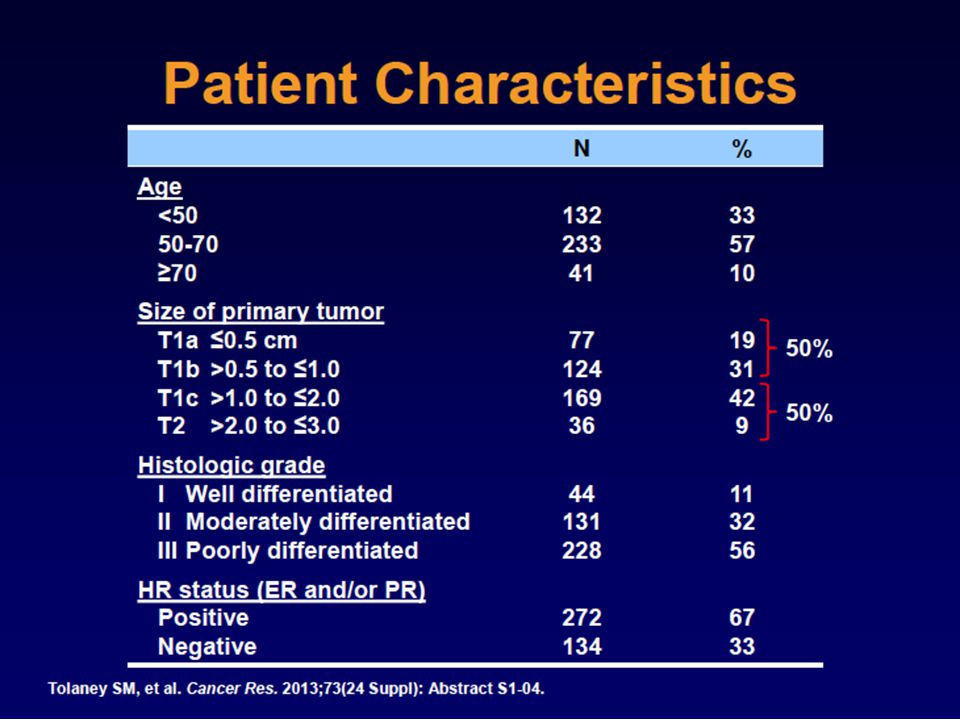
Background The three randomized adjuvant trials of HER2+ early breast cancer included limited patients with stage I disease, and virtually no patients with tumors < 1 cm. Many patients with stage I, HER2+ EBC will have a sufficiently high risk of recurrence to justify administration of adjuvant therapy, but they will likely derive a smaller absolute benefit. The development of regimens with lower degrees of toxicity is important for this population. Tolaney SM, et al. Cancer Res 2013;73:Abst S1-04.

58
[TITLE] Presented By Ines Maria Vaz Duarte Luis, MD at 2013 ASCO Annual Meeting
![[TITLE] Presented By Ines Maria Vaz Duarte Luis, MD at 2013 ASCO Annual Meeting](http://slideplayer.com/slide/1398987/3/images/58/%5BTITLE%5D+Presented+By+Ines+Maria+Vaz+Duarte+Luis%2C+MD+at+2013+ASCO+Annual+Meeting.jpg "[TITLE] Presented By Ines Maria Vaz Duarte Luis, MD at 2013 ASCO Annual Meeting")
59
[TITLE] Presented By Ines Maria Vaz Duarte Luis, MD at 2013 ASCO Annual Meeting
![[TITLE] Presented By Ines Maria Vaz Duarte Luis, MD at 2013 ASCO Annual Meeting](http://slideplayer.com/slide/1398987/3/images/59/%5BTITLE%5D+Presented+By+Ines+Maria+Vaz+Duarte+Luis%2C+MD+at+2013+ASCO+Annual+Meeting.jpg "[TITLE] Presented By Ines Maria Vaz Duarte Luis, MD at 2013 ASCO Annual Meeting")
60
Treatment of T1a/b N0 Tumors: NCCN
Luis IV, et al ASCO 2013 Abstr # 1006

61
[TITLE] Presented By Ines Maria Vaz Duarte Luis, MD at 2013 ASCO Annual Meeting
![[TITLE] Presented By Ines Maria Vaz Duarte Luis, MD at 2013 ASCO Annual Meeting](http://slideplayer.com/slide/1398987/3/images/61/%5BTITLE%5D+Presented+By+Ines+Maria+Vaz+Duarte+Luis%2C+MD+at+2013+ASCO+Annual+Meeting.jpg "[TITLE] Presented By Ines Maria Vaz Duarte Luis, MD at 2013 ASCO Annual Meeting")
62
APT Trial Tolaney SM, et. Cancer Res 2013;73:Abst S1-04.

68
Conclusions Metastatic breast cancer: The landscape of drug choices has changed with the addition of pertuzumab in the front-line and TDM-1 in the second-line. Neoadjuvant therapy: The landscape has changed with the approval of pertuzumab in the neoadjuvant setting. Adjuvant therapy: We await adjuvant trial data on anti-HER2 doublets Identify “low-risk” patients for alternative trastuzumab + chemotherapy regimens.

Similar presentations















>")











