Download presentation
Presentation is loading. Please wait.

1
Spa vid dagkirurgi ”nedan naveln” en alternativ anestesiteknik
Walking Spinal – selektiv unilateral spinal – Mini dos spinal Jan Jakobsson Anestesi & Intensivvård Institutionen för Fysiologi & Farmakologi Karolinska Institutet

2
Ambulatory anaesthesia
Fentanyl Alfentanil Remifentanil

3
Anestesi för nedre extrimitetens ortopediska kirurgi
Höftproteskirurgi – Spa + LIA Knäproteskirurgi – Spa + LIA Akillessena - Spa? Korsband – Spa? Fotledskirurgi - Spa Mellanfot - ? Framfot - ??

4
Lokalbedövning Marcain tung Marcain spinal Chirocaine 5 mg/ml
Narop 5 mg/ml

5
Spinalbedövning Marcain tung 5 mg/ml Indikationer
Spinalanestesi vid kirurgiska ingrepp, till exempel urologiska operationer och operationer i nedre extremiteterna som varar 2–3 timmar samt operationer i buken som varar 45–60 minuter. Indikation Dos ml mg Tillslagstid minuter (ca) Duration timmar (ca) Urologisk kirurgi 1,5-3 ml 7,5-15 mg 5-8 min 2-3 timmar Ingrepp i nedre extremiteter, inklusive höftkirurgi 2-4 ml 10-20 mg Bukkirurgi (inklusive kejsarsnitt) 45-60 min
 Duration. timmar (ca) Urologisk kirurgi. 1,5-3 ml. 7,5-15 mg. 5-8 min. 2-3 timmar. Ingrepp i nedre extremiteter, inklusive höftkirurgi. 2-4 ml mg. Bukkirurgi (inklusive kejsarsnitt) min.")
6
Spinalbedövning Marcain spinal 5 mg/ml Indikationer
Spinalanestesi vid kirurgiska ingrepp i nedre extremiteter, inklusive höftkirurgi, som varar 3–4 timmar och där en uttalad motorblockad behövs. Indikation Dos ml mg Tillslagstid minuter (ca) Duration timmar (ca) Ingrepp i Nedre Extremiteter Inklusive höftkirurgi 2-4 ml 10-20 mg 5-8 min 1,5-4 timmar
 Duration. timmar (ca) Ingrepp i. Nedre. Extremiteter. Inklusive. höftkirurgi. 2-4 ml mg. 5-8 min. 1,5-4 timmar.")
7
Spinalbedövning Narop 5 mg/ml Indikationer
Kirurgisk anestesi: spinalanestesi Indikation Styrka mg/ml Volym ml Dos mg Tillslag minuter Duration timmar Spinal administrering för kirurgi 5 mg/ml 3-4 ml 15-20 mg 1-5 min 2-6 tim

8
Spinalbedövning Chirocaine 5 mg/ml Indikationer Kirurgisk anestesi:
intratekal DOSERINGSTABELL Koncentration mg/ml1 Dos Motorblockad Kirurgisk anestesi: Intratekal 5,0 3 ml (15 mg) Måttlig till fullständig
 Måttlig till fullständig.")
9
Vilket medel är bäst? Ropivacaine, the S-isomer of the propyl homologue of bupivacaine (Whiteside et al. 2001) has approximately 50% of the potency of bupivacaine at equal doses, when administered i.t. (Gautier et al. 1999; McDonald et al. 1999). Levobupivacaine is the S-enantiomer of bupivacaine with a lower degree of cardiotoxicity compared to racemic bupivacaine (Whiteside and Wildsmith 2001). Cardiotoxicity is not relevant with the bupivacaine doses (up to 20 mg) used in spinal anaesthesia. No difference was found between the spinal block after i.t. bupivacaine or levobupivacaine (Alley et al. 2002).
 has approximately 50% of the potency of bupivacaine at equal doses, when administered i.t. (Gautier et al. 1999; McDonald et al. 1999). Levobupivacaine is the S-enantiomer of bupivacaine with a lower degree of cardiotoxicity compared to racemic bupivacaine (Whiteside and Wildsmith 2001). Cardiotoxicity is not relevant with the bupivacaine doses (up to 20 mg) used in spinal anaesthesia. No difference was found between the spinal block after i.t. bupivacaine or levobupivacaine (Alley et al. 2002).")
10
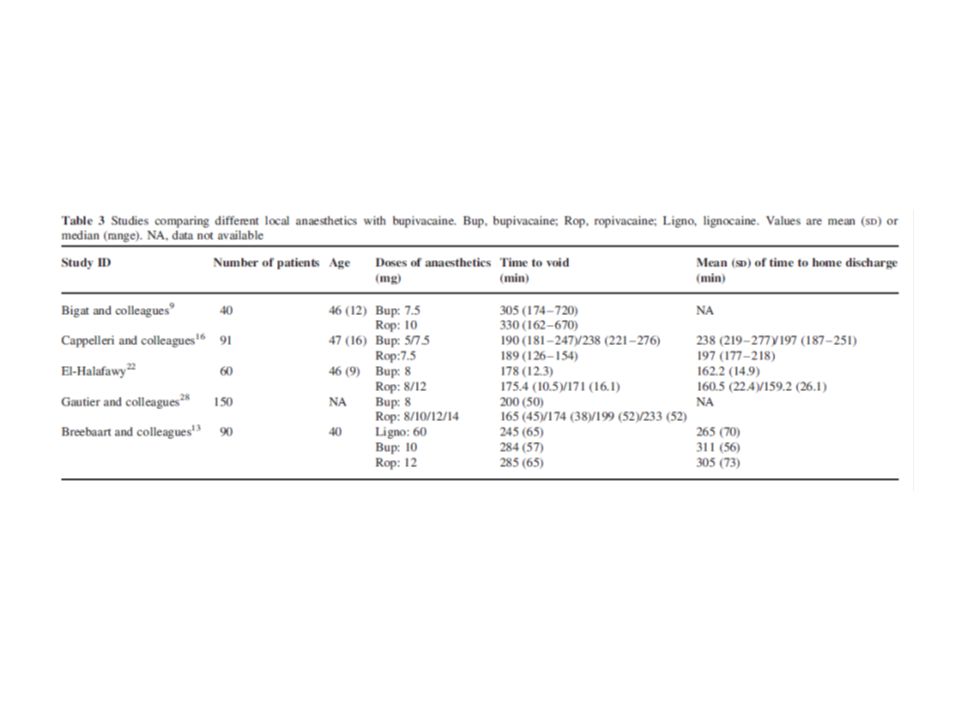
Dos och tid till utskrivning
In a dose-response study of hyperbaric bupivacaine (3.75 – mg) in volunteers, each additional mg of bupivacaine increased the time to home readiness by 21 min (Liu et al. 1996).
 in volunteers, each additional mg of bupivacaine increased the time to home readiness by 21 min (Liu et al. 1996).")
11
Kontraindikation?

12
Allergi?

13
Systemtoxiska effekter

14
Complications in regional anaesthesia
Moen V, Dahlgren N, Irestedt L. Anesthesiology Oct;101(4):950-9.
:")
15
Spinal cord CNS Central Nervous System

16
Spinalkanalen Epiduralt Intratekalt

17
Kroppsläge Sittande Liggande Horisontalt

18
Punktionsnivå L3-L4 L2-L3

19
Vad påverkar hur spinalen sprider sig?
Greene reported 25 factors that could affect the distribution of the local anaesthetic in the cerebrospinal fluid (Greene 1985), but not all of them have clinical relevance. These factors can be classified into 4 subgroups: characteristics of the patient and of the CSF, characteristics of the local anaesthetic agent, and the injection technique used (Table 2). Besides the drug dosage, the position of the patient at the time of injection and thereafter, together with the baricity of the anaesthetic, are the most important factors affecting the level of spinal anaesthesia (Stienstra and Greene 1991; Connolly and Wildsmith 1998; Enk 1998).
, but not all of them have clinical relevance. These factors can be classified into 4 subgroups: characteristics of the patient and of the CSF, characteristics of the local anaesthetic agent, and the injection technique used (Table 2). Besides the drug dosage, the position of the patient at the time of injection and thereafter, together with the baricity of the anaesthetic, are the most important factors affecting the level of spinal anaesthesia (Stienstra and Greene 1991; Connolly and Wildsmith 1998; Enk 1998).")
20
Lite kring faktorerna som påverkar utbredning och återhämtning

21
Selektiv unilateral spinal
The advantages of unilateral or selective versus conventional SA are: better haemodynamic stability (Tanasichuk et al. 1961; Pittoni et al. 1995; Vaghadia et, al. 1997; Fanelli et al. 2000), faster motor and sensory recovery (Vaghadia et al. 1997; Vaghadia 1998; Fanelli et al. 2000) decreased risk of urinary retention (Ben-David et al. 1996; Ben-David et al. 1997; Ben-David et al. 2000; Kuusniemi et al. 2000a; Mulroy et al. 2002). The patients’ satisfaction with the unilateral techniques has been high, too (Pittoni et al. 1995; Kuusniemi et al. 1997; Kuusniemi et al. 2000a).
, faster motor and sensory recovery (Vaghadia et al. 1997; Vaghadia 1998; Fanelli et al. 2000) decreased risk of urinary retention (Ben-David et al. 1996; Ben-David et al. 1997; Ben-David et al. 2000; Kuusniemi et al. 2000a; Mulroy et al. 2002). The patients’ satisfaction with the unilateral techniques has been high, too (Pittoni et al. 1995; Kuusniemi et al. 1997; Kuusniemi et al. 2000a).")
22
SSA

23
SSA Administration

24
SSA Sakralt Horisontalt Kranialt

25
SSA Sakralt Kranialt

26
Spinalanestesi mix ”singel shot” Adrenalin Opioid Sufenta fentanyl
Morfin kombinationer Alfa-2agonister Clonidin kateter

27
Olika blandningar, inte helt lätt

28
Men vad är bäst? Recently several studies with low-dose bupivacaine for ambulatory knee arthroscopy have been conducted with varying failure rates and time to home-readiness. Många olika tekniker inte helt lätttolkade resultat

29
Unilateral bupivacaine spinal anesthesia for outpatient knee arthroscopy. Italian Study Group on Unilateral Spinal Anesthesia. Fanelli G, Borghi B, Casati A, Bertini L, Montebugnoli M, Torri G. Can J Anaesth Aug;47(8): METHODS: One hundred healthy, premedicated patients randomly received conventional bilateral (n = 50) or unilateral (n = 50) spinal anesthesia with 8 mg hyperbaric bupivacaine 0.5%.
 or unilateral (n = 50) spinal anesthesia with 8 mg hyperbaric bupivacaine 0.5%.")
30
Unilateral bupivacaine spinal anesthesia for outpatient knee arthroscopy. Italian Study Group on Unilateral Spinal Anesthesia. Fanelli G, Borghi B, Casati A, Bertini L, Montebugnoli M, Torri G. Can J Anaesth Aug;47(8): RESULTS: Three patients in each group were excluded due to failed block. Readiness for surgery required 13 min ( min) with bilateral and 16 min ( ) with unilateral spinal block (P = ). Sensory and motor blocks on the operated limb were T9 (T12 - T2) with a Bromage score 0/1/2/3: 0/2/0/45 in the unilateral group and T7 (T12 - T1) with Bromage score 0/1/2/3: 4/1/6/36 with bilateral block(P = and P = 0.016, respectively).
 with bilateral and 16 min ( ) with unilateral spinal block (P = ). Sensory and motor blocks on the operated limb were T9 (T12 - T2) with a Bromage score 0/1/2/3: 0/2/0/45 in the unilateral group and T7 (T12 - T1) with Bromage score 0/1/2/3: 4/1/6/36 with bilateral block(P = and P = 0.016, respectively).")
31
Unilateral bupivacaine spinal anesthesia for outpatient knee arthroscopy. Italian Study Group on Unilateral Spinal Anesthesia. Fanelli G, Borghi B, Casati A, Bertini L, Montebugnoli M, Torri G. Can J Anaesth Aug;47(8): Vasopressor was required only in five bilateral patients (P = 0.02). Two segment regression of sensory level and home discharge required 81+/-25 min and 281+/-83 min with bilateral block, and 99+/-28 min and 264+/-95 min with unilateral block (P = and P = 0.90, respectively).
. Two segment regression of sensory level and home discharge required 81+/-25 min and 281+/-83 min with bilateral block, and 99+/-28 min and 264+/-95 min with unilateral block. (P = and P = 0.90, respectively).")
32
Unilateral bupivacaine spinal anesthesia for outpatient knee arthroscopy. Italian Study Group on Unilateral Spinal Anesthesia. Fanelli G, Borghi B, Casati A, Bertini L, Montebugnoli M, Torri G. Can J Anaesth Aug;47(8): CONCLUSION: Seeking unilateral distribution of spinal anesthesia provided more profound and longer lasting block in the operated limb, less cardiovascular effects, and similar home discharge compared with bilateral spinal anesthesia, with only a slight delay in preparation time.

33
Unilateral spinal block for outpatient knee arthroscopy: a dose-finding study. Borghi B, et al. A. J Clin Anesth Aug;15(5):351-6. To evaluate the onset time, success rate, and recovery profile of unilateral spinal anesthesia produced with 4 mg, 6 mg, and 8 mg of 0.5% hyperbaric bupivacaine. MEASUREMENTS AND MAIN RESULTS: The onset time of surgical block; 13 +/- 5 minutes in Group 4 10 +/- 4 minutes in Group 6 (p = 0.006), 9 +/- 4 minutes in Group 8 (p = 0.002). The maximum level of sensory block on the operative and nonoperative sides was; T(10) (T(12)-T(6)) and / (/-L(2)) in Group 4 (p = ), T(8) (T(12)-T(6)) and / (/-L(5)) in Group 6 (p = ), T(7) (T(12)-T(5)) and / (/-T(10)) in Group 8 (p = ).
, 9 +/- 4 minutes in Group 8 (p = 0.002). The maximum level of sensory block on the operative and nonoperative sides was; T(10) (T(12)-T(6)) and / (/-L(2)) in Group 4 (p = ), T(8) (T(12)-T(6)) and / (/-L(5)) in Group 6 (p = ), T(7) (T(12)-T(5)) and / (/-T(10)) in Group 8 (p = ).")
34
Unilateral spinal block for outpatient knee arthroscopy: a dose-finding study. Borghi B, et al. A. J Clin Anesth Aug;15(5):351-6. A strictly unilateral sensory block was observed in; 27 Group 4 patients (90%), 28 Group 6 patients (93%) 23 Group 8 patients (77%) (p = 0.28). Complete unilateral motor block was observed in; 29 Group 4 patients (97%), 28 Group 6 patients (93%), 28 Group 8 patients (93%) (p = 0.80). No failed blocks were reported.
, 28 Group 6 patients (93%) 23 Group 8 patients (77%) (p = 0.28). Complete unilateral motor block was observed in; 29 Group 4 patients (97%), 28 Group 6 patients (93%), 28 Group 8 patients (93%) (p = 0.80). No failed blocks were reported.")
35
Unilateral spinal block for outpatient knee arthroscopy: a dose-finding study. Borghi B, et al. A. J Clin Anesth Aug;15(5):351-6. Complete regression of spinal anesthesia required; 71 +/- 20 minutes in Group 4 (range: 40 to 110 min), 82 +/- 25 minutes in Group 6 (range: 30 to 160 min), 97 +/- 37 minutes in Group 8 (range: 50 to 120 min) (p = 0.003).
, 82 +/- 25 minutes in Group 6 (range: 30 to 160 min), 97 +/- 37 minutes in Group 8 (range: 50 to 120 min) (p = 0.003).")
36
Unilateral spinal block for outpatient knee arthroscopy: a dose-finding study. Borghi B, et al. A. J Clin Anesth Aug;15(5):351-6. CONCLUSIONS: Hyperbaric bupivacaine 4 mg injected slowly through pencil-point directional needles in patients who are maintained in the lateral decubitus position for 15 minutes provided a surgical block that was mostly restricted to the operative side and adequate to perform knee arthroscopy, with a faster recovery profile than when a 6 mg or 8 mg dose was used.

37
SSA Bupivacain Chirocain Ropivacain

38
A comparison of intrathecal plain solutions containing ropivacaine 20 or 15 mg versus bupivacaine 10 mg. Kallio H, Snäll EV, Kero MP, Rosenberg PH Anesth Analg Sep;99(3):713-7, This prospective, randomized, double-blinded study included 90 ambulatory lower-extremity surgery patients who received 2 mL of; ropivacaine 1%, 20 mg ropivacaine 0.75%, 15 mg bupivacaine 0.5% mg

39
Återhämtning Kallio H, et al A&A 2004

40
Kraft Kallio H, et al A&A 2004

41
Comparison of hyperbaric and plain ropivacaine 15 mg in spinal anaesthesia for lower limb surgery.
Br J Anaesth Nov;93(5): Kallio H, Snäll EV, Tuomas CA, Rosenberg PH. BACKGROUND: Previously, plain ropivacaine 15 mg given intrathecally has been shown to be feasible for ambulatory surgery of lower-extremities. Hypothetically, hyperbaric solution could improve and shorten the block. METHODS: This prospective, randomized, double-blind study included 56 patients undergoing surgery of lower extremities. They received intrathecally either 1.5 ml of ropivacaine 10 mg ml(-1) and 0.5 ml of glucose 300 mg ml(-1) (HYP) or 2 ml of ropivacaine 7.5 mg ml(-1) (PL). RESULTS: All patients in Group HYP achieved T(10) dermatome analgesia but only 64% (18/28) of Group PL. T(10) analgesia was reached in 5 min (median, range 5-20 min) in the HYP group vs 10 min (5-45 min) in the PL group (P=0.022), and full motor block in 10 min (5-45 min) vs 20 min (5-60 min) (P=0.003), respectively. Group HYP had a longer duration of analgesia at T(10); 83 min (5-145 min) vs 33 min (0-140 min) (P=0.004). Duration of sensory block from injection of the anesthetic to complete recovery was shorter in Group HYP than in Group PL, 210 min ( min) vs 270 min ( min) (P<0.001), as was duration of motor block, 120 min (5-150 min) vs 210 min ( min) (P<0.001). Patients of Group HYP attained discharge criteria earlier than those of Group PL (P=0.009). CONCLUSION: In comparison with the plain solution, 15 mg of intrathecal hyperbaric ropivacaine produced a faster onset, greater success rate of analgesia at the level of T(10) dermatome, and faster recovery of the block.
: Kallio H, Snäll EV, Tuomas CA, Rosenberg PH. BACKGROUND: Previously, plain ropivacaine 15 mg given intrathecally has been shown to be feasible for ambulatory surgery of lower-extremities. Hypothetically, hyperbaric solution could improve and shorten the block. METHODS: This prospective, randomized, double-blind study included 56 patients undergoing surgery of lower extremities. They received intrathecally either 1.5 ml of ropivacaine 10 mg ml(-1) and 0.5 ml of glucose 300 mg ml(-1) (HYP) or 2 ml of ropivacaine 7.5 mg ml(-1) (PL). RESULTS: All patients in Group HYP achieved T(10) dermatome analgesia but only 64% (18/28) of Group PL. T(10) analgesia was reached in 5 min (median, range 5-20 min) in the HYP group vs 10 min (5-45 min) in the PL group (P=0.022), and full motor block in 10 min (5-45 min) vs 20 min (5-60 min) (P=0.003), respectively. Group HYP had a longer duration of analgesia at T(10); 83 min (5-145 min) vs 33 min (0-140 min) (P=0.004). Duration of sensory block from injection of the anesthetic to complete recovery was shorter in Group HYP than in Group PL, 210 min ( min) vs 270 min ( min) (P<0.001), as was duration of motor block, 120 min (5-150 min) vs 210 min ( min) (P<0.001). Patients of Group HYP attained discharge criteria earlier than those of Group PL (P=0.009). CONCLUSION: In comparison with the plain solution, 15 mg of intrathecal hyperbaric ropivacaine produced a faster onset, greater success rate of analgesia at the level of T(10) dermatome, and faster recovery of the block.")
42
Comparison of hyperbaric and plain ropivacaine 15 mg in spinal anaesthesia for lower limb surgery.
Br J Anaesth Nov;93(5): Kallio H, Snäll EV, Tuomas CA, Rosenberg PH. BACKGROUND: Previously, plain ropivacaine 15 mg given intrathecally has been shown to be feasible for ambulatory surgery of lower-extremities. Hypothetically, hyperbaric solution could improve and shorten the block. METHODS: This prospective, randomized, double-blind study included 56 patients undergoing surgery of lower extremities. They received intrathecally either 1.5 ml of ropivacaine 10 mg ml(-1) and 0.5 ml of glucose 300 mg ml(-1) (HYP) or 2 ml of ropivacaine 7.5 mg ml(-1) (PL). RESULTS: All patients in Group HYP achieved T(10) dermatome analgesia but only 64% (18/28) of Group PL. T(10) analgesia was reached in 5 min (median, range 5-20 min) in the HYP group vs 10 min (5-45 min) in the PL group (P=0.022), and full motor block in 10 min (5-45 min) vs 20 min (5-60 min) (P=0.003), respectively. Group HYP had a longer duration of analgesia at T(10); 83 min (5-145 min) vs 33 min (0-140 min) (P=0.004). Duration of sensory block from injection of the anesthetic to complete recovery was shorter in Group HYP than in Group PL, 210 min ( min) vs 270 min ( min) (P<0.001), as was duration of motor block, 120 min (5-150 min) vs 210 min ( min) (P<0.001). Patients of Group HYP attained discharge criteria earlier than those of Group PL (P=0.009). CONCLUSION: In comparison with the plain solution, 15 mg of intrathecal hyperbaric ropivacaine produced a faster onset, greater success rate of analgesia at the level of T(10) dermatome, and faster recovery of the block.
: Kallio H, Snäll EV, Tuomas CA, Rosenberg PH. BACKGROUND: Previously, plain ropivacaine 15 mg given intrathecally has been shown to be feasible for ambulatory surgery of lower-extremities. Hypothetically, hyperbaric solution could improve and shorten the block. METHODS: This prospective, randomized, double-blind study included 56 patients undergoing surgery of lower extremities. They received intrathecally either 1.5 ml of ropivacaine 10 mg ml(-1) and 0.5 ml of glucose 300 mg ml(-1) (HYP) or 2 ml of ropivacaine 7.5 mg ml(-1) (PL). RESULTS: All patients in Group HYP achieved T(10) dermatome analgesia but only 64% (18/28) of Group PL. T(10) analgesia was reached in 5 min (median, range 5-20 min) in the HYP group vs 10 min (5-45 min) in the PL group (P=0.022), and full motor block in 10 min (5-45 min) vs 20 min (5-60 min) (P=0.003), respectively. Group HYP had a longer duration of analgesia at T(10); 83 min (5-145 min) vs 33 min (0-140 min) (P=0.004). Duration of sensory block from injection of the anesthetic to complete recovery was shorter in Group HYP than in Group PL, 210 min ( min) vs 270 min ( min) (P<0.001), as was duration of motor block, 120 min (5-150 min) vs 210 min ( min) (P<0.001). Patients of Group HYP attained discharge criteria earlier than those of Group PL (P=0.009). CONCLUSION: In comparison with the plain solution, 15 mg of intrathecal hyperbaric ropivacaine produced a faster onset, greater success rate of analgesia at the level of T(10) dermatome, and faster recovery of the block.")
43
Comparison of plain and hyperbaric solutions of ropivacaine for spinal anaesthesia.
Br J Anaesth Jan;94(1): Epub 2004 Oct 29. Fettes PD, Hocking G, Peterson MK, Luck JF, Wildsmith JA. BACKGROUND: Preliminary work has shown that ropivacaine provides spinal anaesthesia of shorter duration than bupivacaine, and may be of particular use in the day-case setting. However, there are few data comparing the actions of plain and hyperbaric solutions of this drug. METHODS: Forty ASA grade I-II patients undergoing elective perineal surgery under spinal anaesthesia were randomized to receive 3 ml ropivacaine 5 mg ml(-1), either in plain solution or with glucose 50 mg ml(-1). The extent and duration of sensory and motor block, pulse rate, blood pressure, and time to mobilization were recorded. RESULTS: Two patients (one per group) were withdrawn because of total block failure. There were significant differences in median time to onset of sensory block at T10 (plain 10 min; hyperbaric 5 min; P<0.01), median maximum extent (plain T8; hyperbaric T4; P<0.05), and median duration of sensory block at T10 (plain 25 min; hyperbaric 115 min; P<0.001). However, median times to complete regression of both sensory (270 vs 240 min; P<0.05) and motor (180 vs 120 min; P<0.001) block were longer in the plain group. Patients therefore mobilized sooner in the hyperbaric group (218 [n=16] vs 286 min [n=17]; P<0.01). All the hyperbaric blocks were adequate for surgery, but three patients receiving plain ropivacaine required general anaesthesia. CONCLUSION: Addition of glucose 50 mg ml(-1) to ropivacaine 5 mg ml(-1) increases the speed of onset, block reliability, duration of useful block for perineal surgery, and speed of recovery. Plain solutions are less reliable for surgery above a dermatomal level of L1.
: Epub 2004 Oct 29. Fettes PD, Hocking G, Peterson MK, Luck JF, Wildsmith JA. BACKGROUND: Preliminary work has shown that ropivacaine provides spinal anaesthesia of shorter duration than bupivacaine, and may be of particular use in the day-case setting. However, there are few data comparing the actions of plain and hyperbaric solutions of this drug. METHODS: Forty ASA grade I-II patients undergoing elective perineal surgery under spinal anaesthesia were randomized to receive 3 ml ropivacaine 5 mg ml(-1), either in plain solution or with glucose 50 mg ml(-1). The extent and duration of sensory and motor block, pulse rate, blood pressure, and time to mobilization were recorded. RESULTS: Two patients (one per group) were withdrawn because of total block failure. There were significant differences in median time to onset of sensory block at T10 (plain 10 min; hyperbaric 5 min; P<0.01), median maximum extent (plain T8; hyperbaric T4; P<0.05), and median duration of sensory block at T10 (plain 25 min; hyperbaric 115 min; P<0.001). However, median times to complete regression of both sensory (270 vs 240 min; P<0.05) and motor (180 vs 120 min; P<0.001) block were longer in the plain group. Patients therefore mobilized sooner in the hyperbaric group (218 [n=16] vs 286 min [n=17]; P<0.01). All the hyperbaric blocks were adequate for surgery, but three patients receiving plain ropivacaine required general anaesthesia. CONCLUSION: Addition of glucose 50 mg ml(-1) to ropivacaine 5 mg ml(-1) increases the speed of onset, block reliability, duration of useful block for perineal surgery, and speed of recovery. Plain solutions are less reliable for surgery above a dermatomal level of L1.")
45
Erfarenheterna från Finland

46
Olika spinaler och tid till utskrivning

47
Median upper level operative side

48
Percent having S1 block

49
Recovery of motor function

50
Spinal anaesthetic technique
Low dose Low volume Low injection speed Lateral position for 10 minutes L 2/3 27 G Quincke needle

51
Success rate

52
Success rate

53
Success rate

54
Quality aspects

55
Quality aspects

56
A comparison of selective spinal anesthesia with hyperbaric bupivacaine and general anesthesia with desflurane for outpatient knee arthroscopy. Anesth Analg Dec;99(6): , Korhonen AM, Valanne JV, Jokela RM, Ravaska P, Korttila KT. Abstract In this randomized and controlled trial, 64 adult ambulatory knee arthroscopy patients received either selective spinal anesthesia (SSA) with 4 mg of hyperbaric bupivacaine or general anesthesia (GA) with desflurane. We conducted the study to determine whether SSA with small-dose bupivacaine provides equal fast-tracking possibilities, a shorter stay in the postanesthesia care unit, and earlier discharge home compared with GA with desflurane. Patients with a high risk for postoperative nausea and vomiting received prophylaxis in the GA group. No difference was seen in the fast-tracking possibilities or time in the postanesthesia care unit between the groups. Home readiness was achieved after 114 (31-174) and 129 (28-245) min (NS) in the SSA and GA groups, respectively. In the hospital, the pain scores were significantly (P < 0.001) lower in the SSA group compared with the GA group and the need for postoperative opioids was significantly (P = 0.008) larger after GA. The incidence of postoperative nausea and vomiting was 0% versus 19% in the SSA and GA groups (P = 0.024), respectively. We conclude that for outpatients undergoing knee arthroscopy, SSA with hyperbaric bupivacaine provides equal recovery times with less frequent side effects compared with GA with desflurane.
: , Korhonen AM, Valanne JV, Jokela RM, Ravaska P, Korttila KT. Abstract. In this randomized and controlled trial, 64 adult ambulatory knee arthroscopy patients received either selective spinal anesthesia (SSA) with 4 mg of hyperbaric bupivacaine or general anesthesia (GA) with desflurane. We conducted the study to determine whether SSA with small-dose bupivacaine provides equal fast-tracking possibilities, a shorter stay in the postanesthesia care unit, and earlier discharge home compared with GA with desflurane. Patients with a high risk for postoperative nausea and vomiting received prophylaxis in the GA group. No difference was seen in the fast-tracking possibilities or time in the postanesthesia care unit between the groups. Home readiness was achieved after 114 (31-174) and 129 (28-245) min (NS) in the SSA and GA groups, respectively. In the hospital, the pain scores were significantly (P < 0.001) lower in the SSA group compared with the GA group and the need for postoperative opioids was significantly (P = 0.008) larger after GA. The incidence of postoperative nausea and vomiting was 0% versus 19% in the SSA and GA groups (P = 0.024), respectively. We conclude that for outpatients undergoing knee arthroscopy, SSA with hyperbaric bupivacaine provides equal recovery times with less frequent side effects compared with GA with desflurane.")
61
Artroskopi av knät Locally applied anaesthesia?? Number of ports
SURGERY Meniscus resection Shaving ”other major”?? Irrigating fluid Fluid pressure Tourniquet Time Pressure

62
Försök till sammanfattning
Unilateral ”selektiv” walking spinal för operation nedre extremiteten L3-4 ”lätt” sänkt huvudända vid knä op 4 mg Marcain tung Bättre kvalitet men mer klåda med 10 microgr fentanyl Långsam injektion Behåll sidoläge ca 10 minuter

63
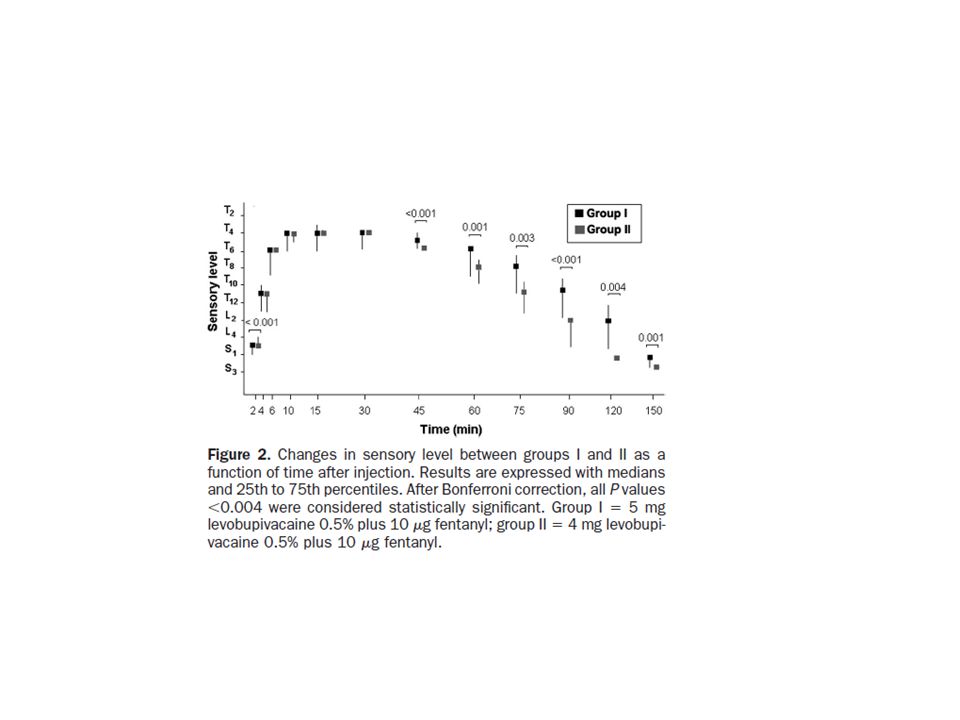
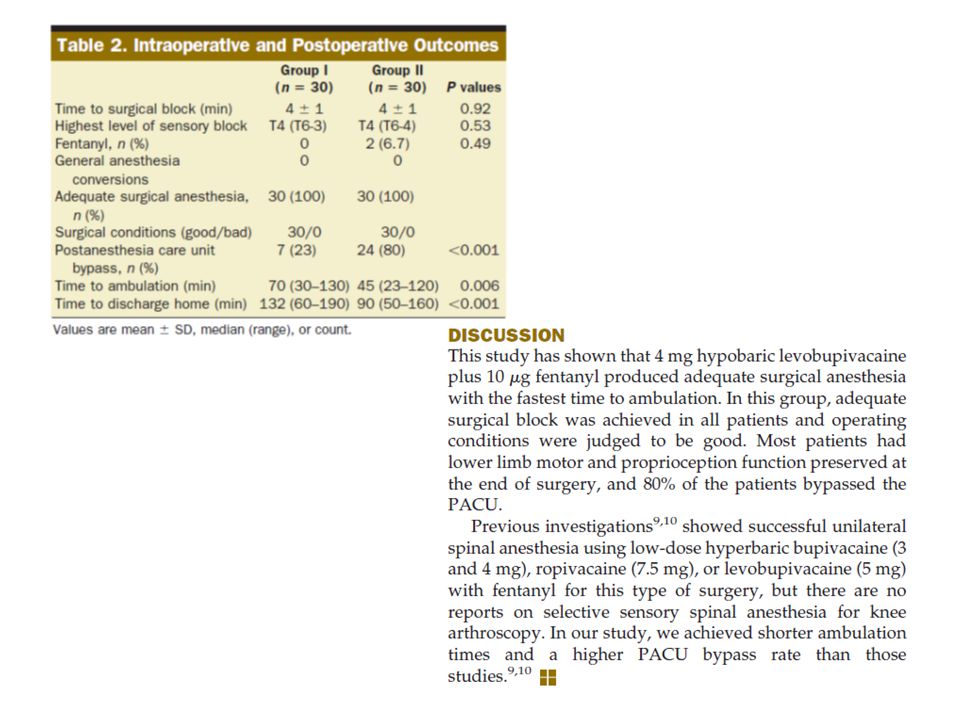
Men så kom det studier från Spain….
Group I received 5 mg (1 mL) levobupivacaine 0.5% (Chirocane 0.5%; Abbott Laboratories, Madrid, Spain) with 10 g fentanyl (0.2 mL). Group II received 4 mg (0.8 mL) levobupivacaine 0.5%with 10 g fentanyl. Group III received 3 mg (0.6 mL) levobupivacaine 0.5% with 10 g fentanyl. All solutions were prepared to a total volume of 3 mL with sterile water. The solutions had a specific gravity of , , and mg/mL, at 25°C, respectively (Anton Paar, Graz, Austria). Spinal anesthesia was performed by one of the authors who was not involved in further patient evaluation. The spinal technique was performed in the sitting position with a midline approach at the L3-4 intervertebral space using a 27-gauge Whitacre spinal needle (Becton Dickinson Medical Systems, Madrid, Spain). After sitting for 2 minutes, patients were placed in the supine position with the back section of the surgical table elevated to 20° to 30° for 5 to 10 minutes. 3 mg avbröts för mycket failures
 levobupivacaine 0.5% (Chirocane 0.5%; Abbott Laboratories, Madrid, Spain) with 10 g fentanyl (0.2 mL). Group II received 4 mg (0.8 mL) levobupivacaine 0.5%with 10 g fentanyl. Group III received 3 mg (0.6 mL) levobupivacaine 0.5% with 10 g fentanyl. All solutions were prepared to a total volume of 3 mL with sterile water. The solutions had a specific gravity of , , and mg/mL, at 25°C, respectively (Anton Paar, Graz, Austria). Spinal anesthesia was performed by one of the authors who was not involved in further patient evaluation. The spinal technique was performed in the sitting position with a midline approach at the L3-4 intervertebral space using a 27-gauge Whitacre spinal needle (Becton Dickinson Medical Systems, Madrid, Spain). After sitting for 2 minutes, patients were placed in the supine position with the back section of the surgical table elevated to 20° to 30° for 5 to 10 minutes. 3 mg avbröts för mycket failures.")
66
The patient was placed in the sitting position
Combined spinal–epidural anesthesia (CSEA) was instituted in the sitting position with a midline approach at the L2–L3 level in all subjects
 was instituted in the sitting position with a midline approach at the L2–L3 level in all. subjects.")
67
Ropivacaine 0.5%, 5 mg (Naropin; AstraZeneca, USA), was mixed with 25 μg fentanyl and sterile water.
The specific gravity of this mixture was 1.002; as the specific gravity of cerebrospinal fluid is 1.003–1.008 at 378C, this mixture would be hypobaric in this fluid. Specific gravity was determined with a refractometer (American Optical Company, Chicago, IL, USA), measured at 378C.
, measured at 378C.")
68
Levobupivacaine 0.75%, 3.75 mg (Chirocaine; Abbott Laboratories, North Chicago, IL, USA), was mixed with 25 μg fentanyl and sterile water; the specific gravity of this mixture was

69
Each of the solutions was diluted to a total volume of 3 ml with distilled water.
The solution was injected over 150–180 s after free cerebrospinal fluid leakage was obtained through the needle, The tip of the needle was pointed in the cephalad direction during this process.

73
Spinal anesthesia mediates improved early function and pain relief following surgical repair of ankle fractures. J Bone Joint Surg Am Feb;92(2): Jordan C, Davidovitch RI, Walsh M, Tejwani N, Rosenberg A, Egol KA. BACKGROUND: To our knowledge, no study to date has compared the use of spinal and general anesthesia in patients undergoing operative fixation of an unstable ankle fracture. The purpose of this study was to assess the effects of anesthesia type on postoperative pain and function in a large cohort of patients. METHODS: Between October 2000 and November 2006, 501 patients who underwent surgical fixation of an unstable ankle fracture were followed prospectively. Patients receiving spinal anesthesia were compared with a cohort who received general anesthesia. All patients were evaluated at three, six, and twelve months postoperatively with use of standardized, validated general and limb-specific outcome instruments. Standard and multivariable analyses comparing outcomes at these intervals were performed. RESULTS: Four hundred and sixty-six patients (93%) who had been followed for a minimum of one year met the inclusion criteria. Compared with the general anesthesia group, the spinal anesthesia group had a greater mean age (p = 0.005), higher classification on the American Society of Anesthesiologists system (p = 0.03), and a greater number of patients with diabetes (p = 0.02). There was no difference in sex distribution between the groups. At three months, patients who received spinal anesthesia had significantly better pain scores (p = 0.03) and total scores on the American Orthopaedic Foot and Ankle Society outcome instrument (p = 0.02). At six months, patients in the spinal anesthesia group continued to have better pain scores (p = 0.04), but there was no longer a difference in total scores (p = 0.06). At twelve months, no difference was detected between the groups in terms of functional or pain scores. There was no difference in complication rates between the groups. CONCLUSIONS: Patients who undergo fixation of an ankle fracture under spinal anesthesia seem to experience less pain and have better function in the early postoperative period. We recommend that, unless there is a specific contraindication, patients should be offered spinal anesthesia when undergoing operative fixation of an ankle fracture.
: Jordan C, Davidovitch RI, Walsh M, Tejwani N, Rosenberg A, Egol KA. BACKGROUND: To our knowledge, no study to date has compared the use of spinal and general anesthesia in patients undergoing operative fixation of an unstable ankle fracture. The purpose of this study was to assess the effects of anesthesia type on postoperative pain and function in a large cohort of patients. METHODS: Between October 2000 and November 2006, 501 patients who underwent surgical fixation of an unstable ankle fracture were followed prospectively. Patients receiving spinal anesthesia were compared with a cohort who received general anesthesia. All patients were evaluated at three, six, and twelve months postoperatively with use of standardized, validated general and limb-specific outcome instruments. Standard and multivariable analyses comparing outcomes at these intervals were performed. RESULTS: Four hundred and sixty-six patients (93%) who had been followed for a minimum of one year met the inclusion criteria. Compared with the general anesthesia group, the spinal anesthesia group had a greater mean age (p = 0.005), higher classification on the American Society of Anesthesiologists system (p = 0.03), and a greater number of patients with diabetes (p = 0.02). There was no difference in sex distribution between the groups. At three months, patients who received spinal anesthesia had significantly better pain scores (p = 0.03) and total scores on the American Orthopaedic Foot and Ankle Society outcome instrument (p = 0.02). At six months, patients in the spinal anesthesia group continued to have better pain scores (p = 0.04), but there was no longer a difference in total scores (p = 0.06). At twelve months, no difference was detected between the groups in terms of functional or pain scores. There was no difference in complication rates between the groups. CONCLUSIONS: Patients who undergo fixation of an ankle fracture under spinal anesthesia seem to experience less pain and have better function in the early postoperative period. We recommend that, unless there is a specific contraindication, patients should be offered spinal anesthesia when undergoing operative fixation of an ankle fracture.")
74
Svensk praxis – Knee arthroscopy routines and practice.
Knee Surg Sports Traumatol Arthrosc Dec;18(12): Epub 2010 Sep 21. Brattwall M, Jacobson E, Forssblad M, Jakobsson J. Source Department of Anaesthesia, Institute for Clinical Sciences at Sahlgrenska Academy, Sahlgrenska University Hospital, Mölndal, SE Gothenburg, Sweden. Knee arthroscopy is one of most commonly performed day-case orthopaedic procedures, thus consuming huge medical resources. The aim of the present questionnaire survey was to study knee arthroscopy routines and practice. METHODS: An electronic web-based survey including questions around pre-, per- and postoperative routines for elective knee arthroscopy was send to all orthopaedic units associated to the Swedish Arthroscopic Society (n = 60). RESULTS: Responses covering 37 centres out of 60 (response rate 62%) were returned. Preoperative radiograph routines varied considerable between centres; conventional radiograph varied between 5 and 100% and preoperative MRI between 5 and 80% of patients. General anaesthesia was the preferred intra-operative technique used in all centres (median 79% of patients), local anaesthesia with or without light sedation was used in all 28 out of the 37 centres responding (median 10% of cases) and spinal anaesthesia was used in 15 centres (median 5% of cases). Intra-articular local anaesthesia was provided in all but one of centres. Perioperative administration of oral NSAIDs was common (31 out 37), 6 centres (all teaching hospitals) did not routinely give pre- or postoperative NSAID. Analgesic prescription was provided on a regular base in 18 (49%) of centres; an NSAID being the most commonly prescribed. All but one centre provided written information and instruction at discharge. Referral to physiotherapy, prescribed sick leave and scheduled follow-up in the outpatient clinic diverged considerably. CONCLUSION: Routines and practice associated to elective knee arthroscopy differed; however, no clear differences in practice were seen between teaching centres, general or local hospitals apart from a lower usage of NSAID for perioperative analgesia. There is an obvious room for further standardisation in the routine handling of patients undergoing elective arthroscopy of the knee.
: Epub 2010 Sep 21. Brattwall M, Jacobson E, Forssblad M, Jakobsson J. Source. Department of Anaesthesia, Institute for Clinical Sciences at Sahlgrenska Academy, Sahlgrenska University Hospital, Mölndal, SE Gothenburg, Sweden. Knee arthroscopy is one of most commonly performed day-case orthopaedic procedures, thus consuming huge medical resources. The aim of the present questionnaire survey was to study knee arthroscopy routines and practice. METHODS: An electronic web-based survey including questions around pre-, per- and postoperative routines for elective knee arthroscopy was send to all orthopaedic units associated to the Swedish Arthroscopic Society (n = 60). RESULTS: Responses covering 37 centres out of 60 (response rate 62%) were returned. Preoperative radiograph routines varied considerable between centres; conventional radiograph varied between 5 and 100% and preoperative MRI between 5 and 80% of patients. General anaesthesia was the preferred intra-operative technique used in all centres (median 79% of patients), local anaesthesia with or without light sedation was used in all 28 out of the 37 centres responding (median 10% of cases) and spinal anaesthesia was used in 15 centres (median 5% of cases). Intra-articular local anaesthesia was provided in all but one of centres. Perioperative administration of oral NSAIDs was common (31 out 37), 6 centres (all teaching hospitals) did not routinely give pre- or postoperative NSAID. Analgesic prescription was provided on a regular base in 18 (49%) of centres; an NSAID being the most commonly prescribed. All but one centre provided written information and instruction at discharge. Referral to physiotherapy, prescribed sick leave and scheduled follow-up in the outpatient clinic diverged considerably. CONCLUSION: Routines and practice associated to elective knee arthroscopy differed; however, no clear differences in practice were seen between teaching centres, general or local hospitals apart from a lower usage of NSAID for perioperative analgesia. There is an obvious room for further standardisation in the routine handling of patients undergoing elective arthroscopy of the knee.")
75
….tack

Similar presentations