Download presentation
Presentation is loading. Please wait.

1
Approach to Adrenal Incidentalomas
Moayad Assiri Urology R4 KAUH

2
Definition. Prevalence. Causes led to it discovery. DDx. Diagnostic approach -Hormonally. -Imaging. -? FNA. Management approach. F\U. Summary. References.

3
(Clinically inapparent adrenal masses).
Definition (Clinically inapparent adrenal masses). adrenal tumor not suspected prior to radiological studies led to it discovery. A disease of modern technology. J Endocrinal Metab Clin North Am 1997 Except: -Pt w known non adrenal malignant tumor. -pt known HTN.
. adrenal tumor not suspected prior to radiological studies led to it discovery. A disease of modern technology. J Endocrinal Metab Clin North Am Except: -Pt w known non adrenal malignant tumor. -pt known HTN.")
4
Incidence of adrenal masses is 9 - 12% in autopsies.
Incidence of AI is 2- 5 %. > Rt > lt . Bil 2 – 10 %. NATIONAL INSTITUTES OF HEALTH Management of the Clinically Inapparent Adrenal Mass (Incidentaloma). Final Statement. July 16, 2002
. Final Statement. July 16,")
5
Adrenal Incidentalomas Study - Chi Mei Medical Center
1998 Jan – 2002 Dec Abdominal CT scan 70,101 in 5 years 127 cases of AI in 256 cases of adrenal tumors Incidence of AI: 0.18% Hormonally active: 4%

6
Mayo clinic 61,054 CT scans performed . Adrenal mass in 2066 pts ( 3.4%). 16.5% were present incidental ( <1 cm ). Overall, AI 259 pts ( 0.4% ) 50% metastatic ca. 25% other known lesions. 7.5% symptomatic tumors.
 50% metastatic ca. 25% other known lesions. 7.5% symptomatic tumors.")
7
Abecassis et al, Toronto, Canada
Prevalence of Adrenal Incidentalomas on CT Imaging Study Year Number of Scans Number with Mass Frequency (%) Abecassis et al, Toronto, Canada 1985 1,459 19 1.3 Belldegrun et al, Boston, MA 1986 12,000 88 0.7 Caplan et al, LaCrosse, WI 1994 1,779 33 1.9 Glazer et al, St. Louis, MO 1982 2,200 16 Herrera et al, Rochester, MN 1991 61,054 259 0.4 Prinz et al, Chicago,IL 1,423 4 0.3 TOTAL(average) 79,915 419 (0.9) Cheng & Shen 2003 70101 127 0.18
 Abecassis et al, Toronto, Canada , Belldegrun et al, Boston, MA , Caplan et al, LaCrosse, WI , Glazer et al, St. Louis, MO , Herrera et al, Rochester, MN , Prinz et al, Chicago,IL. 1, TOTAL(average) 79, (0.9) Cheng & Shen")
8
Causes led to discover IA
342 cases, men and 206 women Reasons for CT scan: nonspecific abdominal pain, % known abdominal or thoracic disease, renal problems, musculoskeletal pain Acta Endocrine (copenh)1989
1989.")
9
Age-dependent occurrence of adrenal adenomas
Increases with Age 1% in age < 30 y. 3 -7 % in age > 50 y. Compensatory growth in response to local ischemic damage of arteriosclerotic disease Higher number of diagnostic procedures performed in aged patients N Engl J Med, 1990

10
Age-dependent occurrence of adrenal cortical adenomas autopsy studies with total of 57,262 subjects
Endocrine and Metabolism Clinics of North America 2000; 29(1):
:")
11
Clinical characteristics
Per definition ,NO clinical symptoms or signs of adrenal disease should be present at the time of Dx. More detailed Q and careful PE might reveal evidence of subtle hormonal excess; -recent w.t gain -skin atrophy. -episodic of headaches.

12
Àdrenal incidentaloma
Majority are neither function nor malignant 70-90%. The malignant tumors may and may not secrete hormonal. The 3 mains hormone-producing tumors: Cortisone producing adenoma SCCS 11%. Pheochromocytoma 7%. Aldoestrone producing adenoma 2%.

13
________________________________________
PREVALENCE OF ADRENAL INCIDENTALOMAS IN DIFFERENT SERIES _______________________________ Type of Tumor Mantero et al Al-SIE Othorst _______________________________________________ Nonhypersecretory tumors Hypersecretory tumors Cortisol-secreting adenomas Aldosteronomas Pheochromocytomas Adrenal carcinomas Myelolipomas Cysts Ganglioneuromas Metastases Unselected patients Oncological patients ________________________________________ AI-SIE: Adrenal Incidentaloma Study Group of the Italian Society of Endocrinology Prevalence (%) Endocrine and Metabolism Clinics of North America 2000; 29(1):
 Endocrine and Metabolism Clinics. of North America 2000; 29(1):")
14
Adrenal cancer Benign Adenoma 50% Cyst 10% Myelolipoma 10%
Pheochromocytoma % Metastases % Adrenal Cancer % The incidental adrenal mass. Am J Med 1996

15
Differential Diagnosis of Adreanl Incidentalomas
Benign nonfunctioning Adenoma Adrenolipoma Amyloidosis Cyst / Pseudocyst Ganglioneuroma Granuloma Infection Hamartoma Hemangioma Leiomyoma Lipoma Myelolipoma Malignant nonfunctioning Angiosarcoma Ganglioneuroblastoma Leiomyosarcoma Malignant schwannoma Metastatic carcinoma Malignant melanoma Malignant lymphoma Adrenocortical carcinoma Endocrine and Metabolism Clinics of North America 2000; 29(1):
:")
16
- Mistaken vasculature - Liver - Lymph nodes - Pancreatic mass
Differential Diagnosis of Adreanl Incidentalomas Pseudoadrenal mass - Mistaken vasculature Liver - Lymph nodes - Pancreatic mass - Spleen - Renal mass - Stomach mass - Technical artifact Hyperfunctioning mass - Pheochromocytoma - Preclinical Cushing’s syndrome - Primary aldosteronism - Nodular hyperplasia - Congenital adrenal hyperplasia - Masculinizing or feminizing tumor - Primary malignancy (Adrenocortical carcinoma) Endocrine and Metabolism Clinics of North America 2000; 29(1):
 Endocrine and Metabolism Clinics. of North America 2000; 29(1):")
17
After incidental discovery of an adrenal mass, 2 questions should be addressed
Functional status hormonally active even in the absence of a classic clinical presentation Malignant potential any chance that the mass is malignant

18
Important consideration
Trying not to miss important pathology. Trying no to subject the pt to unnecessary procedure or surgery. Cost effect.

19
1-Endocrinology investigation significant endocrine activity increase with increase tumor size

20
Subclinical Cushing’s Syndrome
Most frequent hormonal abnormality (5 – 20%) Autonomous cortisol secretion without stigmata of Cushing’s syndrome Diagnostic criteria not yet clearly defined 10-20 mg/day Controlled Primarily By ACTH Negative and Positive Feedback Between Cortisol and ACTH at Pituitary and Hypothalamic Levels
 Autonomous cortisol secretion without stigmata of Cushing’s syndrome. Diagnostic criteria not yet clearly defined mg/day. Controlled Primarily By ACTH. Negative and Positive Feedback Between Cortisol and ACTH at Pituitary and Hypothalamic Levels.")
21
Dx Increased Urinary Free Cortisol (UFC)
Unsuppressed Serum Cortisol Levels After 1-mg Overnight Dexamethasone Low ACTH Levels No Clinical Signs Of Cushing Syndrome Mantero F, Masini AM, Opocher G, Giovagnetti M, Arnaldi G. Horm Res 47:284–289, 1997

22
Dexamethasone Suppression Test
Low-dose: 1mg dexamethasone at 2300, followed by assay of cortisol at 0800 the following day Cortisol > 3 mcg/dl suggests autonomous secretion High-dose: 8 mg dexamethasone at 2300 with assay of cortisol at 0800 the next day Cortisol > 1 mcg/dl indicates autonomous secretion Reduces false positives “Intermediate-dose”: 2 – 3 mg dexamethasone at 2300, followed by cortisol at 0800 Cortisol > 3 mcg/dl reportedly suggestive of autonomy Easier to perform overnight suppression rather than 2-day oral load

23
Association with Metabolic Syndrome?
May contribute to, and worsen, hypertension, obesity , diabetes, dyslipidemia and osteoporosis 1990’s Italian multiinstitutional study collection 1004 patients with adrenal incidentaloma 41% prevalence HTN 10% prevalence DM 28% prevalence obesity

24
Pheochromocytoma Approximately 5-7 % of adrenal incidentalomas.
0.5% among screened hypertensive pt’s Can be clinically silent and not suggested by history Mixed recommendations on diagnostic testing

25
Dx 24-h Urinary fractionated catecholamine excretion or free metanephrines. 24 hour urine fractionated metanephrines recommended by some as first diagnostic test Especially in incidentalomas without radiographic features suggestive of pheochromocytoma Sensitivity and specificity between 91 – 98% Increased even further when fractionated catecholamines added

26
Plasma Free Metanephrines
Used when imaging characteristics and other pre-test probability of pheochromocytoma are high, but 24 hr urine normal Due to high sensitivity (97 – 100%) but low specificity (85 – 89%, ) of test Negative result quite effective at ruling out
 but low specificity (85 – 89%, ) of test. Negative result quite effective at ruling out.")
27
Which Is Better? Catecholamine-Secreting Tumors Histologically Proven In 31 of 340 Patients: Sensitivity Of Plasma Free Metanephrine 97% Specificity 98% Sensitivity Of Urinary Total Metanephrine And Catecholamines 90%; Specificity 85% Sawka et al. JCEM 88(2):
:")
28
Aldosteronism (Conns Sx)
Quite rare cause <1% Most have already been diagnosed before become large enough to be detected by CT/MRI Should be evaluated in all hypertensive patients with incidentaloma Serum potassium not sufficient, but should be included Common to have normokalemia with aldosterone producting adrenal tumor 7 – 38%.

29
Signs and Symptoms in Primary Hyperaldosteronism
Hypertension Headache Weakness And/Or Fatigue Paresthesias Muscle Cramps Polyuria, Polydipsia, Nocturia Arrhythmias

30
Aldosterone Production
ug/day Stimulated by the Renin-Angiotensin System Decreased Perfusion Pressure Hyperkalemia Stimulates and Hypokalemia Inhibits Aldosterone Secretion ACTH Acutely May Stimulate Aldosterone Secretion

31
Dx Plasma aldosterone/plasma renin activity ratio greater than 30 highly suggestive Especially with plasma aldosterone >15 ng/dl Confirm with aldosterone suppression test IV 0.9 NS infusion – 2L over 2 hrs, with supine aldosterone >10 suggestive Can also do 24 hour urinary aldosterone while patient orally ingests 5000 mg sodium/day x 3 days Urinary aldosterone >14 mcg/24º ACE’s and ARB’s can also falsely elevated PRA and should typically be avoided during testing

32
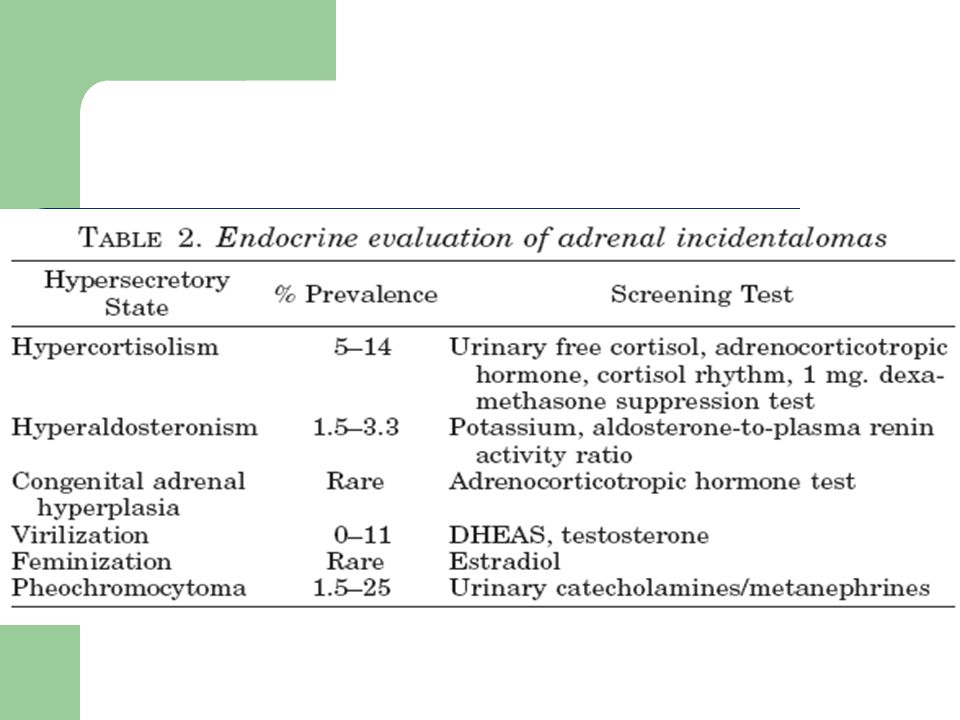
Appropriate screening tests should be performed if the patient has clinical features that are suggestive of increased adrenal function Diagnosis Suggestive Clinical Features Laboratory Tests Pheochromocytoma Hypertension, Paroxysmal Symptoms (eg, palpitation, diaphoresis, headache, pallor, tremor) 24-hr urine: fractionated metanephrines fractionated catecholamines Blood: fractionated metanephrines SC Cushing's syndrome (SCCS) Central obesity, proximal muscle weakness, thin skin, supraclavicular fat pad, facial plethora For patients lacking symptoms of CS: 1-mg overnight dexamethasone suppression test
 24-hr urine: fractionated metanephrines fractionated catecholamines. Blood: fractionated metanephrines. SC Cushing s syndrome (SCCS) Central obesity, proximal muscle weakness, thin skin, supraclavicular fat pad, facial plethora. For patients lacking symptoms of CS: 1-mg overnight dexamethasone suppression test.")
33
Diagnosis Suggestive Clinical Features Laboratory Tests Primary aldosteronism Hypertension, hypokalemia Plasma aldosterone concentration Plasma renin activity Adrenocortical carcinoma Mass effect symptoms, symptoms related to excess glucocorticoid, mineralocorticoid, androgen, or estrogen secretion Serum dehydroepiandrosterone sulfate Measures of clinically indicated steroid

35
Stepwise diagnostic approach
Step I : 1- 24-h Urinary catecholamine excretion or free metanephrines. 2- Serum cortisol after dexamethasone suppression 1mg at 11 pm PO. 3-HTN , Serum K and – PAC\PRA ratio.

36
Stepwise diagnostic approach
Step II : confirmatory test. 1- MRI . CT scan or 123-I-MIBG scintigraphy or 131 I-MIBG. 2- high-dose dexamethasone 8mg suppression test. If +ve .CRH test analysis of diurnal cortisol secretion , and 24-h urine free cortisol. 3- confirm with aldosterone suppression test. And 24-h urine aldosterone .

37
Stepwise diagnostic approach
Step III. Revaluation -repeat screening tests after 2 years in patient with a tumor size of > 3 cm.

38
2- Imaging

39
Imaging Characteristics
Hounsfield Units for Relative Densities of Various Substances Substance Hounsfield units(H) -1,000 Air -50 Fat Water +40 Soft tissue (i.e., muscle) +100 to +400 Calculus + 1,000 Bone Hounsfield units = units of x-ray attenuation used in CT. each pixel is assigned a value on a scale from ,000 to +1,000. CT Scan Hounsfield Scale Measures xray attenuation Each number represents a shade of grey, with air and bone Water as zero Air = -1000 Bone = +1000
 -1,000. Air Fat. Water Soft tissue (i.e., muscle) +100 to Calculus. + 1,000. Bone. Hounsfield units = units of x-ray attenuation used in CT. each pixel is assigned a value on a scale from -1,000 to +1,000. CT Scan. Hounsfield Scale. Measures xray attenuation. Each number represents a shade of grey, with air and bone. Water as zero. Air = Bone =")
40
CT scan Attenuation On CT Scan Is Measured In Hounsfield Units (HU)
Lipid-Rich Masses Are Usually Benign Lipid-Rich Lesions Have Low Attenuation Low Attenuation Lesions Have Low HU Values

41
Computed Tomographic Scans
Unenhanced CT: Adenomas: < 10 HU Malignancies: > 18 HU Sensitivity: 73% Specificity: 96% Delayed Enhanced CT: Adenomas: < 30 HU Malignancies: > 30 HU Sensitivity 95% And Specificity: 100%

42
Adrenocortical carcinoma
Size large, typically > 4 cm Shape irregular with unclear margins Texture inhomogenous with mixed densities compared with liver Laterality usually solitary and unilateral CT > 10 HU without contrast and >30-40 HU 30 min after contrast administration MRI hyperintense to liver on T2-weighted image Presence of necrosis, hemorrhage, or calcifications-- common Growth usually rapid

43
Adrenal cancer CT Contrast-enhanced CT scan through the abdomen of a 56-year-old man reveals a complex solid and cystic, calcified mass (arrow) in the right suprarenal fossa extending into the adjacent liver. The tumor proved at surgery to be a carcinoma of the adrenal cortex. .
 in the right suprarenal fossa extending into the adjacent liver. The tumor proved at surgery to be a carcinoma of the adrenal cortex. .")
44
Malignant Potential Imaging phenotype and mass size are two major predictors of malignancy Additional test that may be preformed to predict malignancy include image-guided needle biopsy and iodocholesterol scintigraphy Hormonal evaluation is not predictive of malignancy Approximately 41% of 1,891 published cases of adrenocortical carcinoma, was not hormone-secreting

45
size The probability that an AI is ACC is increases with increasing size of the lesion. 90% of all ACC is > 6 cm in size. The prevalence of ACC related to size of tumor 2% in tumors < 4 cm. 6% in tumors 4-6 cm. 25% in tumor > 6 cm. Resection all tumor > 4 cm - 8 benign tumors removed for each cancer resected.

46
Imaging Phenotypes of Adrenal Incidentalomas Adrenal cortical adenomas
Size small, typically < 3 cm Shape round to oval with smooth margins Texture homogenous and low density compared with liver Laterality usually solitary and unilateral CT < 10 HU without contrast and <37 HU 30 min after contrast administration MRI isointense to liver on T2-weighted image Presence of necrosis, hemorrhage, or calcifications-- rare Growth usually stable size over time or very slow growth

47
Adrenal adenoma hypodense
Abdominal CT showing a 1.5-cm round hypodense left adrenal cortical adenoma (arrow).
.")
48
Pheochromocytoma Size large, typically > 3 cm
Shape round to oval with smooth margins Texture inhomogenous with cystic texture Laterality usually solitary and unilateral CT >10 HU without contrast and >40 HU 30 min after contrast administration, usually vascular, marked enhancement MRI marked hyperintense compared with liver on T2-weighted image Presence of necrosis, hemorrhage, or calcifications-- hemorrhage and cystic necrotic areas common Growth very slow

49
Pheochromocytoma silent
Abdominal CT showing an 8-cm left adrenal mass (arrow) discovered incidentally. Note the vascular and inhomogenous imaging characteristics of this mass. Biochemical evaluation was consistent with a clinically silent pheochromocytoma, which was confirmed at surgery..
 discovered incidentally. Note the vascular and inhomogenous imaging characteristics of this mass. Biochemical evaluation was consistent with a clinically silent pheochromocytoma, which was confirmed at surgery..")
50
MRI of the abdomen shows a 4
MRI of the abdomen shows a 4.5-cm right adrenal pheochromocytoma (arrows). Upper panel: T1-weighted image. Lower panel: T2-weighted image shows increased signal intensity typical of a pheochromocytoma.
. Upper panel: T1-weighted image. Lower panel: T2-weighted image shows increased signal intensity typical of a pheochromocytoma.")
51
Metastasis Size variable, frequently < 3 cm
Shape round to irregular with unclear margins Texture inhomogenous Laterality often bilateral CT > 10 HU without contrast and >40 HU 30 min after contrast administration, usually vascular, enhancement on tumor rim MRI hyperintense compared with liver on T2-weighted image Presence of necrosis, hemorrhage, or calcifications-- hemorrhage and cystic necrotic areas common Growth usually slow

52
Imaging Characteristics
Adenoma Adrenocortical Carcinoma Pheochromocytoma Metastasis Size < 3 cm diameter >4 cm diameter >3 cm diameter Usually <3 cm Shape Round, smooth Margins Irregular, no clear margins Round/oval, clear margins Oval/irregular, unclear margins Texture Homogenous Heterogenous, mixed densities Heterogenous, cystic Lateralize Solitary, unilateral Solitary, unilateraly Bilateral CT Attenuation <10 HU >25 HU CT Washout at 10 minutes >50% <50% T2 MRI Appearance (compare to liver) = + +++ Necrosis, Ca, hemorrhage Rare Common Occasional Growth rate Slow Rapid Variable
 = Necrosis, Ca, hemorrhage. Rare. Common. Occasional. Growth rate. Slow. Rapid. Variable.")
53
Nuclear Imaging Radionuclide Scintigraphy
PET – most useful in patients with oncologic history and incidentaloma 100% sensitive determining both metastasis and benign adenomas based on adrenalectomy studies

55
MIBG – used to confirm suspicion of pheochromocytoma, little utility in eval of incidentalomas in general

56
NP-59 – radiolabeled cholesterol derivative, preferentially taken up by adrenal adenomas
Unilateral uptake suggests functional adenomas, and may be useful in screening for subclinical cushing’s syndrome

57
3- Fine-needle aspiration biopsy
(FNA) cannot distinguish a benign adrenal mass from the rare adrenal carcinoma. It can distinguish between an adrenal tumor and a metastatic tumor. FNA may be indicated : when there is a suspicion of cancer outside the adrenal gland, or in the patient undergoing a staging evaluation for a known cancer. ? Infection. NATIONAL INSTITUTES OF HEALTH Management of the Clinically Inapparent Adrenal Mass (Incidentaloma). Final Statement. July 16, 2002
 cannot distinguish a benign adrenal mass from the rare adrenal carcinoma. It can distinguish between an adrenal tumor and a metastatic tumor. FNA may be indicated : when there is a suspicion of cancer outside the adrenal gland, or in the patient undergoing a staging evaluation for a known cancer. Infection. NATIONAL INSTITUTES OF HEALTH Management of the Clinically Inapparent Adrenal Mass (Incidentaloma). Final Statement. July 16,")
58
FNA is not useful in the routine evaluation.
Tumors that most commonly metastasize to adrenals are carcinomas of lung, breast, kidney and gastrointestinal tract, melanoma or lymphoma FNA is not free of S.E . FNA is not useful in the routine evaluation. Pheochromocytoma should always be excluded before attempting FNA biopsy of an adrenal mass NATIONAL INSTITUTES OF HEALTH Management of the Clinically Inapparent Adrenal Mass (Incidentaloma). Final Statement. July 16, 2002
. Final Statement. July 16,")
60
Bilateral masses Analyses from two large adrenal incidentaloma studies with 887 and 202 patients showed that bilateral masses were found in 10 to 15 percent of cases. Bilateral adrenal masses can be seen with metastatic disease, congenital adrenal hyperplasia, cortical adenomas, lymphoma, infection (eg, tuberculosis, fungal), hemorrhage, ACTH-dependent Cushing's, pheochromocytoma, amyloidosis, infiltrative disease of the adrenal glands, and ACTH-independent bilateral macronodular adrenal hyperplasia
, hemorrhage, ACTH-dependent Cushing s, pheochromocytoma, amyloidosis, infiltrative disease of the adrenal glands, and. ACTH-independent bilateral macronodular adrenal hyperplasia.")
61
Adrenalectomy? Individualized approach
The decision to operate on pt should be based on : Suspicious of the presence of malignancy. Evidence of function of the tumor. Pt age . Pt preference .

62
Adrenalectomy? Recommended for: all patients with mass size > 6 cm,
pheochromocytoma, aldosteronism, and Cushing’s syndrome Aldosteronism and CS can be treated medically, but surgical approach favored Medical Spironolactone Inhibits sodium-postassium exchange in the distal tubule, normalizes serum K and may lower blood pressure.

63
4 – 6 cm masses Either surgical approach or close follow-up considered reasonable *Strongly consider adrenalectomy: if imaging phenotype suspicious, increase in size > 1 cm during f/u, or development of hormonal hyperfunction during f/u.

64
No difference between open and laparoscopic approaches
Considered in SCS, especially in pt’s < 40 or 50 y/o, and those with disorders attributable to hypercortisolism - Caution for postoperative adrenal insufficiency in SCS patients taken to adrenalectomy. No difference between open and laparoscopic approaches Complication rate of ~3% Special consideration : -Poor surgical patient – FU. -Not possible or difficult FU – Sx. Izaki H et al. Indications for laparoscopic adrenalectomy for non-functional adrenal tumor with hypertension: usefulness of adrenocortical scintigraphy. Int J Urol 2006:13(6):
:")
65
52 patients underwent adrenalectomy 5 patients had malignancy:
342 pts AI. 52 patients underwent adrenalectomy 5 patients had malignancy: 4 adrenocortical carcinomas and one metastasis 1.2% of 342 had cancer No malignancy < 5 cm in diameter 287 of 342 had follow-up; 90% at one year None had extension of tumor or hormonal excess Herrera et al, Surgery

66
(1) Hormonal screening on patients with an AI > 1 cm,
Conclusions: (1) Hormonal screening on patients with an AI > 1 cm, (2) any patient with a hyper-secretory state should undergo adrenalectomy, (3) advise adrenalectomy on AIs > 4 cm and (4) comparison CT scans at 3 month intervals for those choosing observation only of their AI < 4 cm Herrera et al, Surgery
 Hormonal screening on patients with an AI > 1 cm, (2) any patient with a hyper-secretory state should undergo adrenalectomy, (3) advise adrenalectomy on AIs > 4 cm and. (4) comparison CT scans at 3 month intervals for those choosing observation only of their AI < 4 cm. Herrera et al, Surgery.")
67
National survey on AI Purpose: To evaluate AI based on imaging size alone Strict exclusion criteria 1004 enrolled; 584 women and 420 men All patients underwent CT scan or MRI Montero, JCEM

68
85% underwent hormonal evaluation Results:
9.2% had SCS, 1.6% had an aldosteronoma and 4.2% had pheochromocytomas All these patients underwent adrenalectomy A total of 380 patients underwent adrenalectomy. Montero, JCEM

69
Table 4 Histological picture in relation with gender, age, and mass size (CT measurement). Mantero, JCEM

70
(1) An AI > 4 cm is 93% sensitive for detecting all malignancies
Conclusions: (1) An AI > 4 cm is 93% sensitive for detecting all malignancies and (2) Pain at presentation may be associated with a malignant outcome Mantero, JCEM
 An AI > 4 cm is 93% sensitive for detecting all malignancies. and (2) Pain at presentation may be associated with a malignant outcome. Mantero, JCEM.")
71
The Mayo Clinic Study 432 Patients With Adrenal Incidentaloma Retrospectively Evaluated Tumor Diameter Averaged 2.5 cm. Most Malignant Tumors Measured > 5 cm. Removing All Tumors > 4 cm Would Have Removed Eight Benign Tumors For Every Carcinoma Incidentally discovered adrenal tumors: an institutional perspective. Herrera MF; Grant CS; van Heerden JA; Sheedy PF; Ilstrup DM. Surgery 1991 Dec;110(6):
:")
72
Incidentaloma Follow-Up
No single approach is proof yet. 1st Follow up m with another FU at 12 m. Repeat hormone screening after 12m. Then annually y

73
IA Mass Risk of progression
Adrenal Hyperfunction: Unlikely If Lesion < 3 cm Cortisol Hypersecretion Most Likely Disorder 4% After 1 Year 9.5% Within 3 Years None Thereafter Mass Enlargement: 8% After 1 Year 18% After 5 Years Most Enlargement Occurred Within 3 Years Barzon et al J Clin Endocrinol Metab 1999

74
Summary Relatively common – prevalence ~ 2 – 5 %.
Increases with age, so expected to increase further in future. 1 in every million adrenal tumors are malignant Up to 20% are hyperfunction. All patients with incidentaloma need hormonal eval -24º urinary metanephrines -Midnight dexamethasone suppression test -PAC\PRA ratio in pt’s with underlying HTN or hpokalemia. No optimal radiologic test to distinguish between benign and malignant tumors

75
Summary FNA of little value.
Sx indicated for hyperfunction masses , size >6cm and possibility of malignancy . Malignant tumors more likely to be > 4 cm Nearly all masses <4 cm are benign No consensus on follow-up

76
References NATIONAL INSTITUTES OF HEALTH Management of the Clinically Inapparent Adrenal Mass (Incidentaloma).Final Statement. July 16, 2002 Endocrine and Metabolism Clinics of North America 1997 Endocrine and Metabolism Clinics of North America 2000; 29(1): AI-SIE: Adrenal Incidentaloma Study Group of the Italian Society of Endocrinology Barzon et al J Clin Endocrinol Metab 1999 Acta Endocrine (copenh)1989 N Engl J Med, 1990
: AI-SIE: Adrenal Incidentaloma Study Group of the Italian Society of Endocrinology. Barzon et al J Clin Endocrinol Metab Acta Endocrine (copenh)1989. N Engl J Med,")
77
References Endocrine and Metabolism Clinics of North America 2000; 29(1): Mantero F, Masini AM, Opocher G, Giovagnetti M, Arnaldi G. Horm Res 47:284–289, 1997 Sawka et al. JCEM 88(2): Izaki H et al. Indications for laparoscopic adrenalectomy for non-functional adrenal tumor with hypertension: usefulness of adrenocortical scintigraphy Int J Urol 2006:13(6): Incidentally discovered adrenal tumors: an institutional perspective. Herrera MF; Grant CS; van Heerden JA; Sheedy PF; Ilstrup DM. Surgery 1991 Dec;110(6):
: Izaki H et al. Indications for laparoscopic adrenalectomy for non-functional adrenal tumor with hypertension: usefulness of adrenocortical scintigraphy. Int J Urol 2006:13(6): Incidentally discovered adrenal tumors: an institutional perspective. Herrera MF; Grant CS; van Heerden JA; Sheedy PF; Ilstrup DM. Surgery 1991 Dec;110(6):")
Similar presentations













>")

>")




