Download presentation
Presentation is loading. Please wait.

1
The Massachusetts Rural Health Landscape Cathleen McElligott, Director Massachusetts State Office of Rural Health Massachusetts Dept of Public Health Cathleen.mcelligott@state.ma.us Cathleen.mcelligott@state.ma.us January 2011 – UMMS Rural Scholars Program

2
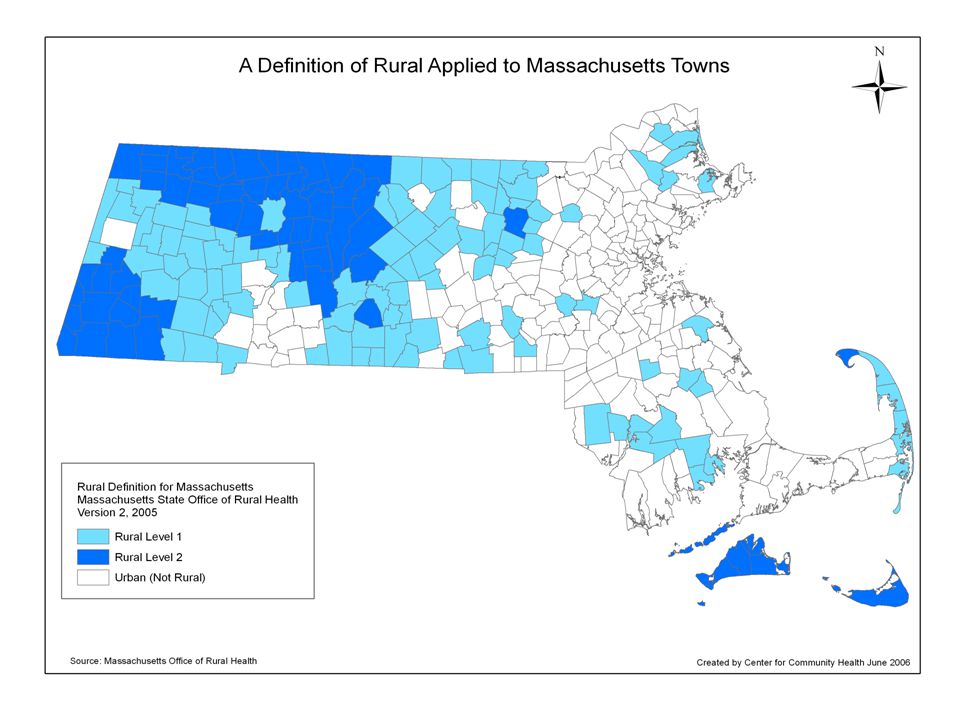
Rural Massachusetts Mass. often thought of as urban because dense concentration of people in metro Boston and eastern cities, BUT.... 713,968 people live in the 65% of state's landmass classified as rural (Census Bureau). Nearly half of MA towns are rural (46%) by a federal definition, primarily in western, central, and coastal southeast MA. Rural MA population density is only 109 people per square mile, comparable with other rural areas of the U.S. (density for urban MA= 2,115 ppsm)
. Nearly half of MA towns are rural (46%) by a federal definition, primarily in western, central, and coastal southeast MA. Rural MA population density is only 109 people per square mile, comparable with other rural areas of the U.S. (density for urban MA= 2,115 ppsm).")
4
A Few Notes on Rural Definitions There are MANY! Typically based on factors such as… Population size Population density Distance from core cities/commuting distance

5
A Few Key Federal Definitions Census BureauRuralIs not in an urbanized area or an urbanized cluster Office of Management and Budget (OMB) RuralIs outside of a metropolitan statistical area University of Washington School of Medicine Rural Health Research Center (WWAMI) Supported by USDA/Economic Research Service and HRSA/Federal Office of Rural Health Policy RuralMeets a Rural Urban Commuting Area Code (RUCAs) for rural (codes 4 through 10 in the taxonomy)
 RuralIs outside of a metropolitan statistical area University of Washington School of Medicine Rural Health Research Center (WWAMI) Supported by USDA/Economic Research Service and HRSA/Federal Office of Rural Health Policy RuralMeets a Rural Urban Commuting Area Code (RUCAs) for rural (codes 4 through 10 in the taxonomy)")
6
National Rural Health Association Definition of Rural, Policy Statement, November 2005 NRHA strongly recommends that definitions of rural be specific to the purposes of the programs in which they are used. Programs targeting rural communities and providers do so for particular reasons…..these reasons should be the guidance for selecting the criteria for a programmatic designation. This will ensure that a designation is appropriate for a specific program, while limiting the possibilities that other unrelated programs adopt a definition, which is not created to fit that program.

8
Main Rural Health System Issues Low population density Distance and isolation

9
Rural Healthcare Because population is smaller and spread out, program fixed costs can be higher per person served Building a system with lower volume while maintaining quality and accessibilty In addition to access to care and good health outcomes The economic impact of the health system in rural MA needs to be considered Largest employer and economic engine in rural areas

10
Rural MA Socioeconomic Barriers Incomes lower Rely heavily on tourism, service, agricultural, and fishing economies Some rural towns are former small mill towns where the mill has closed or greatly downsized Higher proportion of self-employed, family workers, and small businesses; often do not provide health insurance Number of persons in rural areas with advanced education lower than the State average

11
Geographic Barriers for Rural MA Such as: Mountains, hills, oceans, winding country roads, long distances, lack of public transportation Low population densities Patchwork quilt of small towns Lack of inexpensive and fast telecommunications, (broadband, high speed internet, cell phone) further isolate rural communities from more centralized or regionalized state programs.
 further isolate rural communities from more centralized or regionalized state programs.")
12
Publicly Financed Care & Services With the economic demographic the rural population is more dependent on publicly-funded health services, as are the providers. Berkshire County, 50.5% of pregnant women have publicly financed prenatal care compared to 34.2% statewide. High proportion of elderly population; Medicare is payer of major importance.

13
Rural Appropriate Models Allow rural communities to develop models that work for them and not scale down urban models. Within state and federal programs, rural communities need to be allowed to develop rural-appropriate models and demonstrate rural best practices. Build on strengths of rural communities e.g., innovativeness, good collaborators, strong community support and involvement, good at developing new programs, strong sense of place and community, good system thinkers, etc. Need support for innovative and coordinated workforce programs to build on what has been started with rural health organizations.

14
A Special Population When DPH is identifying health disparities it needs to consider RURAL as a special population...with a geographic health disparity. Health problems in rural areas are as real as other areas, just not as visible because the populations are smaller. Rural areas deserve to be counted, studied, and reported on in state data reports. You will find health disparities only where you look.

15
When you see one rural area you have seen one rural area. Some similar characteristic needs, challenges, and strengths as a group. But, always have to look at each rural area so you do not mask needs or challenges for particular rural parts of the state.

16
Health Care Safety Net 69 acute care hospitals in MA 9 are smaller community hospitals in rural communities (SHIP eligible) 3 are Critical Access Hospitals (1 a former CAH) 1 is a certified as Rural Medicare Dependent Hospital (has submitted CAH application) Also 2 moderately sized PPS hospitals in rural areas 52 CHC organizations with 184 access sites in MA 6 CHC organizations serving rural with 10 rural sites 1 is a CMS certified Rural Health Clinic About 4 applications in for new CHC rural expansion sites Still huge rural gaps, working on….. A few other: rural school based health centers, outpatient hospital clinics, VA vans, Wampanoag Tribe, etc.

17
MA SORH Three Federal Grants 1. State Office of Rural Health Program 2. Massachusetts Rural Hospital Flexibility Program 3. Small Rural Hospital Improvement Program

18
Mass SORH Established in 1994 at Mass DPH Funding Federal Office of Rural Health Policy/HRSA MDPH state matching funds Builds partnerships to improve access to health services, build better systems of care, and improve health status in rural communities.

19
State Office of Rural Health Functions Use various communications strategies for information dissemination Provide educational and networking opportunities Coordinate resources and activities Provide technical assistance for a wide range of needs Strengthen local, state, and federal partnerships Assess and document rural health needs Maintain a focal point for rural health – policy, rural-relevant programs Further strengthen a framework that links rural communities with State and Federal resources Strengthen rural health care delivery systems Develop local capacity/leadership for addressing solutions to rural health problems

20
MA SORH Programmatic Areas of Focus Healthcare workforce - recruitment/retention and pipeline Safety net development Chronic disease prevention and management Oral health care Injury prevention Elder health services Veterans services Rural Hospital Flex Program –hospitals, rural health systems, EMS Small Rural Hospital Improvement Program

21
Visit SORH On Facebook: www.facebook.com/RuralHealthMDPH www.facebook.com/RuralHealthMDPH The Web: www.mass.gov/dph/ruralhealth

22
Rural Hospital Flex Program Financial and Operational Performance Improvement Quality Improvement Health System Development and Community Engagement

23
Financial and Operational Performance Improvement Conversion of an additional hospital to CAH TA for market analysis, strategic performance assessment and planning, new service feasibility studies, management training Rural Hospital Board Development Modules (NEPI) Implementation of state and federal healthcare reform CEO/CFO Network Continued monitoring of fiscal and operational data of MA small rural hospitals Cultural competency and translation services Patient and Family Councils
 Implementation of state and federal healthcare reform CEO/CFO Network Continued monitoring of fiscal and operational data of MA small rural hospitals Cultural competency and translation services Patient and Family Councils")
24
Flex Program: Quality Improvement MA Rural Hospital Pharmacist Network Anti-Coagulation Program Diabetes Management Project 24/7 Staffing Strategies Automation and Use of Technology 34B Program implementation HIT and implementation of electronic health records (meaningful use) Massachusetts Primary Stroke Services (PSS) CAH Medicare Beneficiary Project - Hospital Compare measures
 Massachusetts Primary Stroke Services (PSS) CAH Medicare Beneficiary Project - Hospital Compare measures")
25
Flex Program: Quality Improvement Institute for Healthcare Improvement Rural Expeditions and Passport (NEPI) HCAHPS/Patient Satisfaction Patient Care Transitions STAAAR Initiative (State Action on Avoidable Re- Hospitalizations) Rural Relevant Measures
 HCAHPS/Patient Satisfaction Patient Care Transitions STAAAR Initiative (State Action on Avoidable Re- Hospitalizations) Rural Relevant Measures")
26
Health System Development and Community Engagement EMS Services Integration/Coordination EMS Quality Improvement Projects Swing Bed Program Development CAH-Community Health Center Collaboration

27
Critical Access Hospitals (CAHs) Unique CMS designation for small rural hospitals to improve the viability of these lower volume facilities and bring additional resources into the community Eligibility in a rural area, <25 beds +10 DPU, 96 hour LOS, more than 35 miles by road to next nearest hospital or a rural necessary provider Process for designation coordinated by SORH in collaboration with DHCQ and OEMS at DPH Currently we have 3 CAHs, 1 previous CAH, and working with 1 additional CAH applicant
 Unique CMS designation for small rural hospitals to improve the viability of these lower volume facilities and bring additional resources into the community Eligibility in a rural area, <25 beds +10 DPU, 96 hour LOS, more than 35 miles by road to next nearest hospital or a rural necessary provider Process for designation coordinated by SORH in collaboration with DHCQ and OEMS at DPH Currently we have 3 CAHs, 1 previous CAH, and working with 1 additional CAH applicant")
28
Benefits of CAH Status Cost-based reimbursement from Medicare which has the potential to increase revenues Focus on local community needs and enhanced networking with other parts of the healthcare system More flexible staffing and services, within state licensure laws Capital improvement costs are included in allowable costs for determining Medicare reimbursement Access to Flex Program and other targeted grant funds

29
Small Rural Hospital Improvement Program (SHIP) Makes annual grant awards of approximately $9,000 per eligible small rural hospital (less than 50 beds in a rural area as defined by MA state law/regulations). Patient Protection and Affordable Care Act re-defined the use of these funds starting in FY2010. Funds to assist with implementing: Prospective Payment Systems and delivery system changes to implement Value Based Purchasing: quality improvement, quality outcomes Accountable Care Organizations: network/service development and reporting and HIT systems. Payment Bundling

30
SHIP Hospitals in MA 9 small community hospitals in rural MA: 1. Athol Memorial Hospital, 2. Baystate Mary Lane Hospital, 3. Clinton Hospital, 4. Fairview Hospital, 5. Marthas Vineyard Hospital, 6. Nantucket Cottage Hospital, 7. Nashoba Valley Medical Center, 8. North Adams Regional Hospital, 9. Wing Memorial Hospital.

31
How Do We Determine Which Issues? 1. Trends in health care environment 2. Opportunities, opportunities, opportunities 3. Needs assessments – qualitative and quantitative 4. Constituency interests and priorities 5. Interests of Partners 6. Priorities of funders, MDPH, EOHHS 7. Staff backgrounds

32
Key Rural Organizations Federal Office of Rural Health Policy http://ruralhealth.hrsa.gov/ National Rural Health Association http://www.nrharural.org/ New England Rural Health RoundTable http://www.newenglandruralhealth.org/ Rural Assistance Center http://www.raconline.org/

33
New England Rural Health RoundTable Rural health association for the 6 New England States linked with the National Rural Health Association Vibrant member driven organization with committed board of directors, excellent professional staff, and active committees with a broad range of activities The New England Rural Health RoundTable is the forum for promoting healthy rural communities and solutions to the unique health challenges facing rural New England.

34
NERHRTs Objectives Serve as a unified voice for the promotion of rural health needs and issues in New England. Identify rural health needs and issues in New England. Share timely information about key state and federal rural health policies and programs. Educate and advocate for rural health. Encourage networking and collaboration in support of rural health.

36
Primary Stroke Services Developed with assistance from Mass SORH Fairview Hospital (CAH) Results Oct. 06-07: 25 stroke patients 12 with ischemic stroke 5 patients received t-PA 7 patients discharged home 13 patients transferred to BMC 3 patients admitted to Fairview Hospital Symptoms onset to t-PA: 2 hours, 19 minutes

37
Emerging Challenge...Rural Dialysis (Chronic Disease Management) Encapsulates most rural issues Chronic disease management Rural access Staffing High importance...Low volume...High Cost
 Encapsulates most rural issues Chronic disease management Rural access Staffing High importance...Low volume...High Cost")
38
Western Mass EMS Council Recruitment and Retention Survey, Spring 2006 92% response rate from EMS organizations funded by Mass SORH Service Level 39% of respondents - Basic Level Only 18% of respondents - Intermediate Level is highest level 43% of respondents - Paramedic Level Personnel Status 49% respondents have paid staff 22% of respondents have a mix of paid and volunteer staff 27% of respondents have volunteer staff

39
People-Per-Dentist Ratio 30% of cities/towns in Massachusetts dont have enough dentists to care for the people who live there. Mapping Access to Oral Health Care in Mass., Catalyst Institute, Oct. 2006

40
Distribution of MassHealth (Medicaid) Dentists The majority of MassHealth dentists in Massachusetts are clustered in urban areas. Mapping Access to Oral Health Care in Mass., Catalyst Institute, Oct. 2006

42
Emergency Department Visit Rates for Fall-Related Injuries by Region Massachusetts: 2003-2005 ** * * Age-adjusted to the 2000 US standard population. Source: Division of Health Care Finance and Policy. Calendar Year 2003-2005. Emergency Department Visits * ** Statistically different from State (p.05) Red (*) = Statistically worse; Green (**) = Statistically better than state * *
 Red (*) = Statistically worse; Green (**) = Statistically better than state * *.")
43
Hospital Discharge Rates for Motor Vehicle-Related Injuries by Region, Berkshires, and Pittsfield Massachusetts: 2003-2005 Statistically different from State (p.05) Red (*) = Statistically worse; Green (**) = Statistically better Source: MDPH Bureau of Health Statistics, Research, and Evaluation
 Red (*) = Statistically worse; Green (**) = Statistically better Source: MDPH Bureau of Health Statistics, Research, and Evaluation")
Similar presentations












>")








