Download presentation
Presentation is loading. Please wait.

1
1 Clinical and Technology Integration to Support Transformation November 7, 2013 Stephen A. Morgan, M.D. Chief Medical Information Officer Senior Vice President Carilion Clinic

2
Greetings from Western Virginia 2

4
Carilion Clinic continues to be the premier healthcare delivery system in western Virginia Accountable medical group with approximately 600 physicians, 150 advanced care practitioners 300 affiliated physicians. 850,000 primary care visits and 50,000 urgent care visits Full or partial interests in eight hospitals Full range of services and an active graduate medical education program 56 percent inpatient market share in total service area More than twice that of nearest competitor (HCA) Health plan Offering Medicare advantage and Medicaid plans The Market 85% FFS Dominant payor with 70% market share
 Health plan Offering Medicare advantage and Medicaid plans The Market 85% FFS Dominant payor with 70% market share.")
5
Carilion Clinic Mission: Improve the Health of the Communities We Serve Vision 2017: We are committed to a Common Purpose of Better Patient Care, Better Community Health and Lower Cost

6
Building Blocks of our Success Physician leadership Technology –EHR - –Data Analytics -

7
Building Blocks of our Success Patient Engagement Partnerships –Payers –Service Providers Provider Engagement

8
Whats Driving Change Rising health care costs Unstable economy Changes in consumer demand Advances in technology Generational differences in physician work/life balance Working to license Working in teams Workforce shortages 8

9
An all too familiar story… 9

10
Our National Spend Average Healthcare Spending per Capita,1980–2009 Adjusted for differences in cost of living Source: OECD Health Data 2011 (June 2011). Dollars THE COMMONWEALTH FUND

11
Our National Health 11

12
12 Life expectancy improved by 3 years Years with disability increased US fell from 14 th to 26 th compared to other nations. Leading cause for premature deaths include CVD Lung Cancer CVA Leading cause of Disabilities Back Pain Musculoskeletal issues Depression / Anxiety

13
13 Demographic Trends 1/3 US population – Baby Boomers 10,000 people a day reach 65 1 in 10 Baby Boomers is managing multiple chronic illnesses; by 2030: 1 in 4 have diabetes 1 in 2 have arthritis 1 in 2.5 will be obese Treatment of patients with co-morbities cost 7 x those without chronic illness 2/3 Medicare spending - 5 or more chronic conditions

14
Health Care Costs Concentrated in Sick Few Sickest 10 Percent Account for 65 Percent of Expenses Source: Agency for Healthcare Research and Quality analysis of 2009 Medical Expenditure Panel Survey. Distribution of health expenditures for the U.S. population, by magnitude of expenditure, 2009 1% 5% 10% 50% 65% 22% 50% 97% $90,061 $40,682 $26,767 $7,978 Annual mean expenditure

15
Challenges with Todays Care Healthcare costs growing; burden to business Overuse; volume treadmill Inconsistent care; fragmentation Lack of coordination Payment model at odds with countering rising costs Data held close to the vest 15

16
The Hope 16 Improve access Improve health outcomes Reduce cost

17
The Strategy: Follow the Money To optimize the healthcare dollar and improve health outcomes, both government and private payers are (gradually) shifting from volume-based reimbursement to value-based reimbursement 17
 shifting from volume-based reimbursement to value-based reimbursement 17")
18
Emerging Payment Models Bundle payments Pioneer ACO MSSP ACO: Advanced payment model FQHC Medical Homes Value based payment models-P4P State engagement models – for integration of dual eligible individuals 18

19
Is Reform Possible? Able to manage risk Integration Engaged physician leadership Effective health information management Time to change – pace 19

21
Our Areas of Focus Population Health –PCMH Care coordination for high-risk and high-frequency patients Wellness, prevention, Choosing Wisely Payment reform Provider Engagement Health IT Integration 21

22
PHM INITIATIVES 22

23
System PHM Initiatives Transformation Oversight Committee –Oversees work of committees in 3 areas: Care Integration Informatics Finances/Contracting Initial focus on COPD Led by Chief Strategy Officer

24
24 System PHM Initiatives Problem Focus Areas Patient Risk Levels

25
25 System PHM Initiatives Program Infrastructure Areas 1 and 2: Disease-Focused Ambulatory Case Management and High Utilization Management Area 3: Ambulatory Quality / Pay for Performance (P4P) INFORMATION & GUIDES Data Analytics and Reporting Clinical Protocols and Pathways CULTURE CHANGE & ENGAGEMENT Patient Education and Engagement Organizational Change Management (Provider and Staff Training and Engagement) TOOLS & RESOURCES Point-of-Care Decision Support Centralized Patient Outreach EHR Care Plans Extensivist Team Palliative Care and Hospice Home Health
 INFORMATION & GUIDES Data Analytics and Reporting Clinical Protocols and Pathways CULTURE CHANGE & ENGAGEMENT Patient Education and Engagement Organizational Change Management (Provider and Staff Training and Engagement) TOOLS & RESOURCES Point-of-Care Decision Support Centralized Patient Outreach EHR Care Plans Extensivist Team Palliative Care and Hospice Home Health")
26
Carilion Clinic: PCMH Today Total Program Sites: 27 Family Medicine - 21 Internal Medicine - 4 Pediatrics - 2 Recognition Status Level 3 Recognition – 27 Panel Size: 200,000 77% of Department Patients Providers: 136 Physicians - 106 ACPs - 30 Care Coordinators Budgeted Positions: 22 FTEs

27
PAYMENT REFORM 27

28
Accountable Care Activities Payor Arrangements –Managed Medicare and Medicaid Owned – Medicaid HMO –MajestaCare Contracted MAP –Humana, UHC –Aetna ACO (Whole Health) Doctors Connected –ACO MSSP Commercial –Anthem PC2
 Doctors Connected –ACO MSSP Commercial –Anthem PC2")
29
New Contracting Offsetting costs of PCMH o Medicare Advantage Contracts – Humana & United o Managed Medicaid PMPMs o Anthem PC2 & Aetna PCMH program o 2013 - Medicare Reimbursement for care coordination in 30 days following IP / SNF discharge Additional gain sharing opportunities o Medicare Shared Savings Plan o Aetna partnership with Carilion ACO o Managed Medicaid & Medicare Advantage plans

30
PROVIDER ENGAGEMENT 30

31
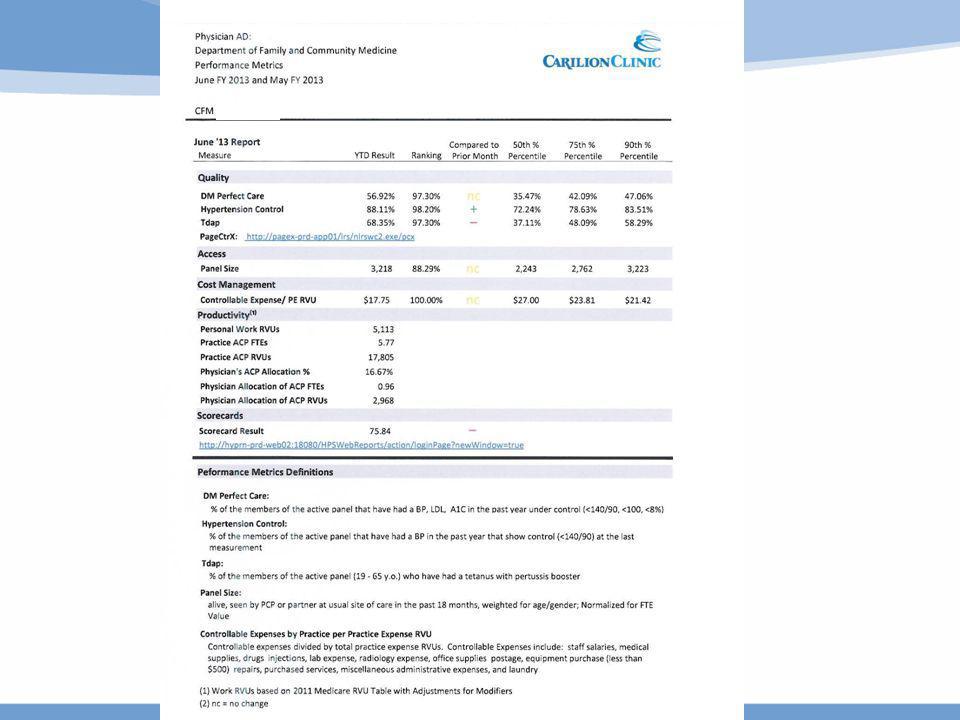
Physician Compensation Moving from Volume to Value Major Components: –Personal RVUs (~ 85%) –ACP oversight (RVUs) (~ 5%) –Performance metrics (~ 10%) Panel size Quality metrics Expense management
 –ACP oversight (RVUs) (~ 5%) –Performance metrics (~ 10%) Panel size Quality metrics Expense management")
32
Care Integration Sub-Group of Transformation Oversight Oversight of integrated projects –Representatives from all departments –Education for first year Payment reform Understanding our data / opportunities –Process improvement –Transitions of care Employed providers 32

33
Working with Community Providers Open Medical Model - Hospitals Involvement of medical directors with LOS committee Data sharing and transparency Involvement in decision making EMR Joint leadership and affiliation 33

34
HEALTHCARE IT AND ACCOUNTABLE CARE

35
Health IT is essential not only to accountable care organizations (ACO) but also healthcare in general Kathleen Sebelius, MPA, Secretary of the U.S. Department of Health & Human Services

36
Population Health Management Fundamental to every major healthcare reform initiative today – Patient-Centered Medical Home –Accountable Care Organization EHRs alone are not sufficient to manage populations effectively Provider groups and health systems that automate the spectrum of population health functions will be best positioned to succeed

37
Healthcare IT and ACOs The Critical List Population identification - attribution Identification of care gaps – Decision Support Risk Stratification Cross Continuum Care management Quality and Outcomes measurement Patient engagement Telemedicine Mixing claims and clinical data Predictive modeling Clinical information exchange

38
PATIENT ENGAGEMENT

40
40 Bridging the gap between home, hospital, office and beyond…

41
CARE COORDINATION

42
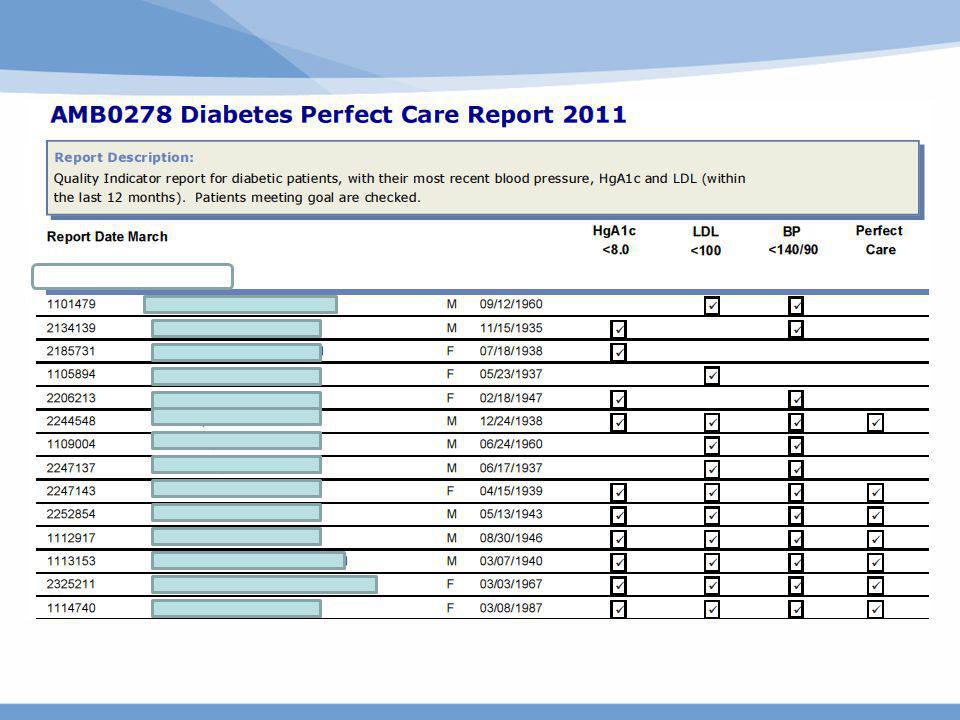
Chronic Disease Registries

43
High Risk Patients for Re-admission

44
Care Plans Across the Continuum Developing a disease management section in the EMR navigator High risk patients flagged Using problem lists and linked episodes Viewed by IP, AMB, and ED.

45
TRANSPARENT DATA DELIVERY TO PROVIDERS

46
46

50
Primary Care Group Dashboard

51
PAYOR DATA

52
ED Frequent Flyers

53
ENTERPRISE DATA WAREHOUSE Putting it all together

54
Enterprise Data Warehouse

55
EARLY OUTCOMES 55

56
Aetna Whole Health ACO Outcomes BaselineCurrent (2011) (2012-2013) Bed Days/1,000 125.7 118.3 Readmission Rate 5.6% 4.9% Avoidable ER Visits/1,000 113.3 85.9 Hi-Tech imaging/1,000 69.2 62.8
 ( ) Bed Days/1, Readmission Rate 5.6% 4.9% Avoidable ER Visits/1, Hi-Tech imaging/1,")
57
Aetna Whole Health ACO Outcomes Quality Metric Baseline 2011Current 2012-2013*Benchmark Colorectal Screening76%83%63% Diabetes HgbA1c testing 91.2%93.8%91% Diabetes Lipid Profile testing 88%89%87% Patients with CAD on lipid lowering RX 100%99%**98% *Benchmark= HEDIS 2012 75 percentile **Aetna Benchnark

58
Carilion Patient Centered Medical Home Outcomes Comparative Clinical Performance Measures: 2009-2012 Q-4 2009 Q-2 2012 Percent Change (%) 1. Body Mass Index (BMI) Measured for Patients <18 Years of Age39.5%92.9%135.2% 2. Pneumococcal Vaccination for Patients >65 Years of Age74.2%79.0%6.5% 3. Breast Screening for Female Patients 40-69 Years of Age56.2%66.8%18.9% 5. A1c Testing for Diabetics 18-75 Years of Age85.2%91.9%7.9% 6. Persistent Asthmatics with Controller Medications Prescribed86.2%93.1%8.0% 7. Diabetics with Blood Pressure Controlled at <140 SBP / 90 DBP68.4%72.2%5.6% 8. Hypertensive Patients with Blood Pressure Controlled at <140 SBP / 90 DBP64.6%67.6%4.6% Source: 70,000 patient study in 20 Carilion mature medical homes during the period 2009 – 2012; "The Impact of the Patient-Centered Medical Home on Hypertension."
 Measured for Patients <18 Years of Age39.5%92.9%135.2% 2. Pneumococcal Vaccination for Patients >65 Years of Age74.2%79.0%6.5% 3. Breast Screening for Female Patients Years of Age56.2%66.8%18.9% 5. A1c Testing for Diabetics Years of Age85.2%91.9%7.9% 6. Persistent Asthmatics with Controller Medications Prescribed86.2%93.1%8.0% 7. Diabetics with Blood Pressure Controlled at <140 SBP / 90 DBP68.4%72.2%5.6% 8. Hypertensive Patients with Blood Pressure Controlled at <140 SBP / 90 DBP64.6%67.6%4.6% Source: 70,000 patient study in 20 Carilion mature medical homes during the period 2009 – 2012; The Impact of the Patient-Centered Medical Home on Hypertension. .")
59
Care Coordination – Early Success in Quality Metrics Two Year Retrospective Study 2,800 Diabetes Mellitus (DM) Patients with Care Coordination compared to 30,000 DM patients with usual care in Carilion Clinical Outcome Data Diabetic Patients in PCMH Sites who received Care Coordination Relative Impact A1c Reduction No Care Coordination- 0.07 Care Coordination - 0.60 8.5 LDL Reduction No Care Coordination - 9.5 Care Coordination -14.2 1.5 BMI (Body Mass Index) Reduction No Care Coordination - 2.8 Care Coordination - 5.0 1.8 DBP (Diastolic Blood Pressure) Reduction No Care Coordination - 2.1 Care Coordination - 3.8 1.8 SBP (Systolic Blood Pressure) Reduction No Care Coordination - 2.8 Care Coordination - 5.0 1.8
 Patients with Care Coordination compared to 30,000 DM patients with usual care in Carilion Clinical Outcome Data Diabetic Patients in PCMH Sites who received Care Coordination Relative Impact A1c Reduction No Care Coordination Care Coordination LDL Reduction No Care Coordination Care Coordination BMI (Body Mass Index) Reduction No Care Coordination Care Coordination DBP (Diastolic Blood Pressure) Reduction No Care Coordination Care Coordination SBP (Systolic Blood Pressure) Reduction No Care Coordination Care Coordination")
60
Median = 6.8 Average = 7.3 80% N = 23,473 patients with type 2 DM

61
Is it Easy? Costly Disrupted relationships Staff felt disengaged Leadership turnover Staff felt disengaged Management in new territory Support systems not ready for change 61

62
Key Drivers Physician Leadership and engagement –CMO, CSO, CMIO, Department Chairs Information Technology –EMR – EPIC, MyChart –Telemedicine –Data Warehouse Aligned Incentives –System Balanced Scorecard –Physician Compensation Contracting / Payment Reform

Similar presentations