Download presentation
Presentation is loading. Please wait.

1
Red Cell Exchange for Methemoglobinemia: Case Study and Review of Evidence
Kathleen Montgomery, MD, MPH December 10, 2015 Vanderbilt University School of Medicine

2
Case 50 year old African American male presented to VUMC 11/21/2015 with newly diagnosed T-cell acute lymphoblastic leukemia Found to have spontaneous tumor lysis syndrome

3
Tumor Lysis Syndrome Intracellular components (nucleic acids, potassium) released into extracellular compartment Induced by cytotoxic chemotherapy or spontaneous Results in hyperuricemia, hyperkalemia, hyperphosphatemia*, and hypocalcemia* *Spontaneous TLS does not result in hyperphosphatemia!

4
Tumor Lysis Syndrome

5
Tumor Lysis Syndrome Uric acid crystals are diamond or barrel shaped crystals that are typically yellow to orange-brown in color Uric acid crystals are insoluble - precipitate in renal tubules and cause acute kidney failure and death Electrolyte abnormalities can cause fatal arrhythmias

6
Case 50 year old male presented to VUMC with newly diagnosed T-cell acute lymphoblastic leukemia Found to have spontaneous tumor lysis syndrome Potassium: 7.3 mmol/L (ref: ) Uric Acid: 13.3 mg/dL (ref: ) Phosphate: 4.7 mg/dL (ref: ) Calcium: 9.0 mg/dL (ref: ) Creatinine: 1.64 mg/dL (ref: ) BUN: 34 mg/dL (ref: 8-26)
 Uric Acid: 13.3 mg/dL (ref: ) Phosphate: 4.7 mg/dL (ref: ) Calcium: 9.0 mg/dL (ref: ) Creatinine: 1.64 mg/dL (ref: ) BUN: 34 mg/dL (ref: 8-26)")
7
Case Patient was given allopurinol (600mg) & rasburicase (7.5 mg)
9
Rasburicase Recombinant Urate Oxidase
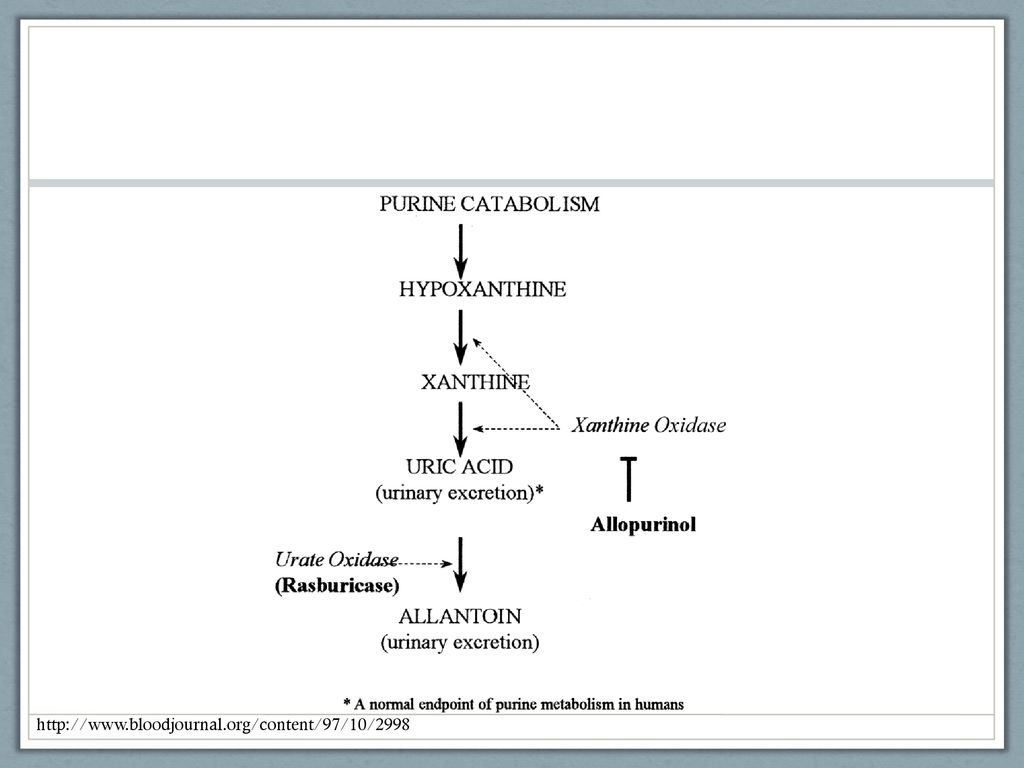
Recommended for use during tumor lysis syndrome (or prophylactically for patients at high risk); 0.2 mg/kg/day for up to 5 days Oxidizes uric acid into allantoin, which is highly soluble and freely excreted by the kidneys
; 0.2 mg/kg/day for up to 5 days. Oxidizes uric acid into allantoin, which is highly soluble and freely excreted by the kidneys.")
10
Case Following rasburicase & allopurinol:
Uric acid: > 7.3 -> 2.1 (mg/dL)
")
11
Case Rasburicase Ras Hemoglobin: mg/dL
Heinz bodies appear as small round inclusions within the red cell body, though they are not visible when stained with Romanowsky dyes. They appear more clearly when supravitally stained[5] (e.g., with new methylene blue or bromocresol green). Heinz bodies are formed by damage to the hemoglobin component molecules, usually through oxidant damage, or from an inherited mutation (i.e. change of an internal amino acid residue). As a result, an electron from the hemoglobin is transferred to an oxygen molecule, which creates areactive oxygen species (ROS) that can cause severe cell damage leading to premature cell lysis.[6] Damaged cells are cleared by macrophages in thespleen, where the precipitate and damaged membrane are removed, leading to characteristic "bite cells". The patient’s hemoglobin decreased from 14.5 mg/dL to 7.7 mg/dL over 5 days
. Heinz bodies are formed by damage to the hemoglobin component molecules, usually through oxidant damage, or from an inherited mutation (i.e. change of an internal amino acid residue). As a result, an electron from the hemoglobin is transferred to an oxygen molecule, which creates areactive oxygen species (ROS) that can cause severe cell damage leading to premature cell lysis.[6] Damaged cells are cleared by macrophages in thespleen, where the precipitate and damaged membrane are removed, leading to characteristic bite cells . The patient’s hemoglobin decreased from 14.5 mg/dL to 7.7 mg/dL over 5 days.")
12
Rasburicase Adverse Effect: Hemolysis
Contraindicated in G6PD deficiency; causes delayed hemolysis Hydrogen peroxide (oxidant) is a byproduct of uric acid -> allantoin reaction G6PD deficient patients have reduced tolerance to oxidative stress Result: Heinz bodies, red cell rigidity, and destruction by macrophages in the reticuloendothelial system (extravascular hemolysis) – “bite cells” It is not practical (or possible) to test for G6PD deficiency in the acute phase Heinz bodies appear as small round inclusions within the red cell body, though they are not visible when stained with Romanowsky dyes. They appear more clearly when supravitally stained[5] (e.g., with new methylene blue or bromocresol green). Heinz bodies are formed by damage to the hemoglobin component molecules, usually through oxidant damage, or from an inherited mutation (i.e. change of an internal amino acid residue). As a result, an electron from the hemoglobin is transferred to an oxygen molecule, which creates areactive oxygen species (ROS) that can cause severe cell damage leading to premature cell lysis.[6] Damaged cells are cleared by macrophages in thespleen, where the precipitate and damaged membrane are removed, leading to characteristic "bite cells".
 is a byproduct of uric acid -> allantoin reaction. G6PD deficient patients have reduced tolerance to oxidative stress. Result: Heinz bodies, red cell rigidity, and destruction by macrophages in the reticuloendothelial system (extravascular hemolysis) – bite cells It is not practical (or possible) to test for G6PD deficiency in the acute phase. Heinz bodies appear as small round inclusions within the red cell body, though they are not visible when stained with Romanowsky dyes. They appear more clearly when supravitally stained[5] (e.g., with new methylene blue or bromocresol green). Heinz bodies are formed by damage to the hemoglobin component molecules, usually through oxidant damage, or from an inherited mutation (i.e. change of an internal amino acid residue). As a result, an electron from the hemoglobin is transferred to an oxygen molecule, which creates areactive oxygen species (ROS) that can cause severe cell damage leading to premature cell lysis.[6] Damaged cells are cleared by macrophages in thespleen, where the precipitate and damaged membrane are removed, leading to characteristic bite cells .")
13
Case

14
Case 6 hours after rasburicase, the patient’s oxygen saturation was persistently reading 85% despite 10L O2 by high-flow nasal cannula and 100% oxygen through a nonrebreather Co-oximetry revealed a metHg of 10.3%

15
Rasburicase Adverse Effect: Methemoglobinemia
Seen in <1% of patients Similar mechanism to hemolysis: hydrogen peroxide formed, G6PD deficient patients have reduced tolerance to oxidative stress Oxidation of Hb iron -> methemoglobinemia It is not practical (or possible) to test for G6PD deficiency in the acute phase
 to test for G6PD deficiency in the acute phase.")
16
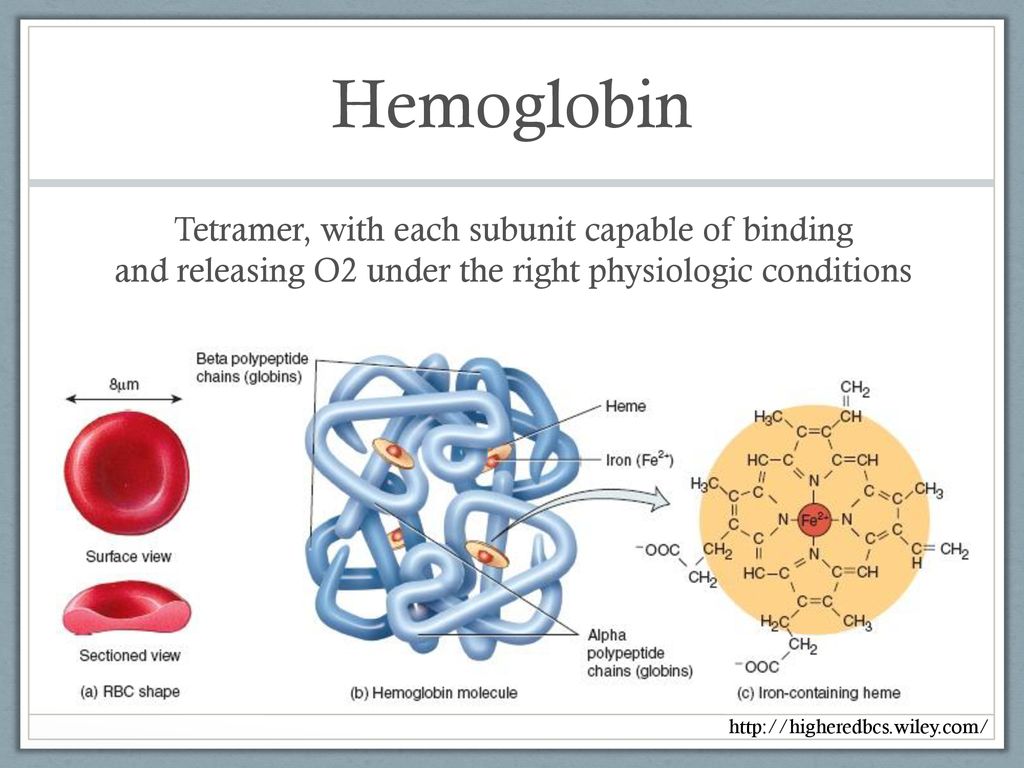
Hemoglobin Tetramer, with each subunit capable of binding and releasing O2 under the right physiologic conditions
17
Methemoglobin (Divalent: Ferrous) Capable of binding O2
(Triavalent: Ferric) Incapable of binding O2
 Incapable of binding O2.")
18
Methemoglobin Methemoglobin left- shifts the hemoglobin dissociation curve of the other three iron molecules, making it harder to offload oxygen to end-organ tissues

19
Methemoglobinemia Under normal conditions, cytochrome B5 reductase & other enzymes keep MetHb levels below 1% Hereditary mutations: Cytochrome B5 reductase Hemoglobin (e.g. HbM) Acquired: Numerous drugs and toxins (dapsone, antimalarials, local anesthetics) G6PD deficiency can exacerbate in times of oxidative stress
 Acquired: Numerous drugs and toxins (dapsone, antimalarials, local anesthetics) G6PD deficiency can exacerbate in times of oxidative stress.")
20
Methemoglobinemia First symptom: cyanosis unresponsive to O2
Pulse oximeter is unreliable, as metHb is detected by sensors for both oxyhemoglobin (940 nm) & deoxyhemoglobin (660 nm) Co-oximetry needed for diagnosis Blood is “chocolate brown” Tubes 1 & 2 – 70% metHb Tube 3 – 20% metHb Tube 4 – 0% metHb Image from:
 & deoxyhemoglobin (660 nm) Co-oximetry needed for diagnosis. Blood is chocolate brown Tubes 1 & 2 – 70% metHb. Tube 3 – 20% metHb. Tube 4 – 0% metHb. Image from:")
21
Methemoglobinemia 20-30%: Anxiety, tachycardia, lightheadedness, headache 30-50%: Fatigue, tachypnea, confusion, dizziness 50-70%: Coma, seizures, dysrhythmias, acidosis

22
Case The patient was given 1mg/kg IV methylene blue
standard therapy for methemoglobinemia

23
Rasburicase-induced methemoglobinemia: Reported Cases
PubMed ID

24
Methylene Blue Provides an additional avenue for reducing MetHb
In glucose-6-phosphate dehydrogenase deficiency, NADP cannot be oxidized to NADPH; methylene blue cannot be reduced into methylene leucoblue Methylene blue is an oxidant – patient gets worse!

25
Case After receiving methylene blue, metHb increased
Ras MetHb % G6PD screen was sent: the patient was found to be deficient!

26
G6PD Deficiency Caused by single nucleotide substitution (many identified) X-linked recessive inheritance In the US, African-American males have the highest prevalence (10%) – Mediterraneans also at increased risk Confers resistance to P. falciparum and P. vivax
 – Mediterraneans also at increased risk. Confers resistance to P. falciparum and P. vivax.")
27
G6PD Deficiency: Testing issues
Reliability: Testing in the setting of hemolysis can result in false-negatives: The most severely deficient RBCs have been removed from circulation via hemolysis Re-test 3 months later to confirm a negative result Practicality: If patient has severe tumor lysis syndrome or methemoglobinemia, it is impractical to wait for G6PD results before giving rasburicase or methylene blue* *7 of 9 reported cases of rasburicase-induced metHb occurred in patients with G6PD deficiency!

28
Methylene Blue discontinued, Ascorbic Acid/Vitamin C started
Case Methylene Blue discontinued, Ascorbic Acid/Vitamin C started Vitamin C Methylene Blue Ras Ras MetHb %

29
Primary team consults transfusion medicine:
Case Primary team consults transfusion medicine: “Will you do a red cell exchange for this patient with 13% methemoglobinemia?”

30
Indications for Red Cell Exchange
American Society for Apheresis Guidelines – 2013 Category I – Apheresis accepted as a first-line therapy Category II – Apheresis accepted as a second-line therapy Category III – Optimum role of apheresis is not established; decision-making should be individualized Category IV – Published evidence demonstrates or suggests apheresis to be ineffective or harmful (IRB approval recommended)
")
31
Indications for Red Cell Exchange
American Society for Apheresis Guidelines – 2013 Category I – HbSS acute stroke, Severe babesiosis Category II – HbSS Acute chest syndrome, HbSS stroke prophylaxis, HbSS vaso-occlusive pain crisis, severe malaria Category III – HbSS pripism, HbSS multiorgan failure; tacrolimus overdose, Incompatible hematopoietic stem cell transplant Category IV – None

32
Indications for Red Cell Exchange
American Society for Apheresis Guidelines – 2013 Methemoglobinemia = NOT LISTED! Case reports: 1 cases of successful automated red cell exchange for metHb 1 case of successful “exchange transfusion” (unspecified) for rasburicase-induced metHb 1 case of rasburicase-induced metHb successfully managed with ascorbic acid (but patient never received methylene blue) Few other nonspecific successful “exchanges” for metHb of other causes
 for rasburicase-induced metHb. 1 case of rasburicase-induced metHb successfully managed with ascorbic acid (but patient never received methylene blue) Few other nonspecific successful exchanges for metHb of other causes.")
33
RCE for MetHb: Published Case

34
RCE for MetHb: Published Case
26 month old African American boy Presented after drinking 3oz artificial fingernail remover fluid containing nitroethane Cyanotic on presentation, and O2 sat remained at 80% after ventilation with 100% O2 MetHb 39%, no change with methylene blue Was found to have G6PD deficiency

35
RCE for MetHb: Published Case
Failed methylene blue, G6PD deficient Whole-blood exchange (2 blood volumes), metHb 32% RCE (1.3 volumes), MetHb 7% The boy was discharged, one week later MetHb 1% Exchange transfusion has traditionally been recom- mended for treatment of patients whose acquired methe- moglobinemia is refractory to methylene blue [23]. How- ever, our case demonstrates that some patients may not benefit from manual whole blood exchange. The whole blood exchange procedure required the manufacture of an expensive blood product consisting of RBC reconsti- tuted in AB plasma. The volumes removed and infused with each cycle were limited to under 10% of the pa- tient’s whole blood volume. After a 4 1 ⁄ 2 -hr procedure to exchange two whole blood volumes, approximately one- sixth of the patient’s affected RBC remained in his cir- culation [34]. In addition, the duration of the procedure likely allowed sufficient time for the replacement RBC to be slowly affected by the ongoing stimulus to form met- hemoglobin. The automated RBC exchange did not require recon- stitution of the replacement blood product with plasma. The patient’s platelets were returned to him, and he was maintained in even fluid balance and stable blood Hb concentration during the procedure. The 40-min auto- mated 1.3 volume RBC exchange removed almost 80% of the affected RBC from his circulation [34]. His met- hemoglobin level was successfully diminished by the procedure and did not rise thereafter.
, metHb 32% RCE (1.3 volumes), MetHb 7% The boy was discharged, one week later MetHb 1% Exchange transfusion has traditionally been recom- mended for treatment of patients whose acquired methe- moglobinemia is refractory to methylene blue [23]. How- ever, our case demonstrates that some patients may not. benefit from manual whole blood exchange. The whole. blood exchange procedure required the manufacture of. an expensive blood product consisting of RBC reconsti- tuted in AB plasma. The volumes removed and infused. with each cycle were limited to under 10% of the pa- tient’s whole blood volume. After a ⁄ 2. -hr procedure to. exchange two whole blood volumes, approximately one- sixth of the patient’s affected RBC remained in his cir- culation [34]. In addition, the duration of the procedure. likely allowed sufficient time for the replacement RBC to. be slowly affected by the ongoing stimulus to form met- hemoglobin. The automated RBC exchange did not require recon- stitution of the replacement blood product with plasma. The patient’s platelets were returned to him, and he was. maintained in even fluid balance and stable blood Hb. concentration during the procedure. The 40-min auto- mated 1.3 volume RBC exchange removed almost 80% of the affected RBC from his circulation [34]. His met- hemoglobin level was successfully diminished by the. procedure and did not rise thereafter.")
36
Exchange transfusion for rasburicase-induced MetHbemia
12 year old male with newly diagnosed T-ALL Uric acid elevated (22.1 mg/dL) Rasburicase was administered, 12h later uric acid was <0.2 mg/dL Developed hypoxia unresponsive to oxygen, MetHB found to be 7-10% Given methylene blue, MetHb stayed at 7% Double-volume exchange transfusion (unspecified) brought his MetHb to 0%, where it remained
 Rasburicase was administered, 12h later uric acid was <0.2 mg/dL. Developed hypoxia unresponsive to oxygen, MetHB found to be 7-10% Given methylene blue, MetHb stayed at 7% Double-volume exchange transfusion (unspecified) brought his MetHb to 0%, where it remained.")
37
Case The patient had persistently elevated MetHb (13%) with shortness of breath and continued O2 requirement despite ascorbic acid treatment The decision was made to proceed with limited red cell exchange (1600mL), with a goal MetHb of <8% Post-RCE MetHb 8.3%, decreased dyspnea and O2 requirement
, with a goal MetHb of <8% Post-RCE MetHb 8.3%, decreased dyspnea and O2 requirement.")
38
Case Methylene Blue Ascorbic Acid RBC Exchange Ras Ras Ras

39
Case

40
Question for thought: Should we do RBC exchange for methemoglobinemia?
Few published cases showing effectiveness of exchange transfusion – nearly all pediatrics One discussing RCE specifically RCE was successful after manual exchange transfusion failure

41
Question for thought: At what %MetHb should we exchange?
Risk-benefit – central line placement, blood product exposure. Published case: 32% MetHb Treating the patient vs. treating the numbers Is the patient symptomatic? At what level do we give methylene blue? “Treatment should be considered when MetHb reaches 30% in an asymptomatic patient and 20% in a symptomatic patient” – Patnaik, 2014 UpToDate: “If the patient is symptomatic or if the methemoglobin level is >20 percent, specific therapy is urgently indicated.”

42
Question for Thought: To what goal %MetHb should we exchange?
Diminishing returns with RCE as level decreases Published case showed 7% post-procedure MetHb; generally <10% is goal with methylene blue therapy Is the patient symptomatic?

43
Questions for Thought Should all males of African or Mediterranean descent be screened for G6PD before administering rasburicase? Since most reports of rasburicase-induced methemoglobinemia have occurred in G6PD deficient patients, should methylene blue be contraindicated in this setting?

44
Summary Numerous drugs and toxins can cause methemoglobinemia, especially in the setting of G6PD deficiency Rasburicase can cause methemoglobinemia and hemolysis through oxidative stress (especially in G6PD deficient patients) Methylene blue exacerbates methemoglobinemia in G6PD deficient patients
 Methylene blue exacerbates methemoglobinemia in G6PD deficient patients.")
45
Summary In patients with refractory methemoglobinemia or G6PD deficiency, red cell exchange may be an effective treatment Only one case report has detailed RBC exchange for MetHb (32%), achieving final MetHb level of 7% There are no evidence-based recommendations for methemoglobin thresholds or treatment goals
, achieving final MetHb level of 7% There are no evidence-based recommendations for methemoglobin thresholds or treatment goals.")
46
Questions?

47
References Bhat P, Sisler I, Collier AB 3rd. Exchange transfusion as treatment for rasburicase-induced methemoglobinemia in a glucose-6-phosphage dehydrogenase deficient patient. Pediatr Blood Cancer Oct;51(4):568 Browning LA, Kruse JA. Hemolysis and methemoglobinemia secondary to rasburicase administration. Ann Pharmacother Nov;39(11): Cheah CY, Lew TE, Seymour JF, Burbury K. Rasburicase causing severe oxidative hemolysis and methemoglobinemia in a patient with previously unrecognized glucose-6-phosphate dehydrogenase deficiency. Acta Haematol. 2013;130(4):254-9. Coiffier B, Altman A, Pui CH, Younes A, Cairo MS. Guidelines for the management of pediatric and adult tumor lysis syndrome: an evidence-based review. Journal of Clinical Oncology Jun; 26(16): Golden PJ, Weinstein R. Treatment of high-risk, refractory acquired methemoglobinemia with automated red blood cell exchange. Journal of Clinical Apheresis. 1998;13:28-31. Patnaik S, Manivachagan MN, James EJ, Ebenezer K. Methylene blue unresponsive methemoglobinemia. Indian Journal of Critical Care Medicine Apr; 18(4): Sonbol MB, Yadav H, Raidya R, Rana V, Witzig TE. Methemoglobinemia and hemolysis in a patient with G6PD deficiency treated with rasburicase. Am J Hematol. 2013; 88:152-4
:568. Browning LA, Kruse JA. Hemolysis and methemoglobinemia secondary to rasburicase administration. Ann Pharmacother Nov;39(11): Cheah CY, Lew TE, Seymour JF, Burbury K. Rasburicase causing severe oxidative hemolysis and methemoglobinemia in a patient with previously unrecognized glucose-6-phosphate dehydrogenase deficiency. Acta Haematol. 2013;130(4): Coiffier B, Altman A, Pui CH, Younes A, Cairo MS. Guidelines for the management of pediatric and adult tumor lysis syndrome: an evidence-based review. Journal of Clinical Oncology Jun; 26(16): Golden PJ, Weinstein R. Treatment of high-risk, refractory acquired methemoglobinemia with automated red blood cell exchange. Journal of Clinical Apheresis. 1998;13: Patnaik S, Manivachagan MN, James EJ, Ebenezer K. Methylene blue unresponsive methemoglobinemia. Indian Journal of Critical Care Medicine Apr; 18(4): Sonbol MB, Yadav H, Raidya R, Rana V, Witzig TE. Methemoglobinemia and hemolysis in a patient with G6PD deficiency treated with rasburicase. Am J Hematol. 2013; 88:")
Similar presentations







 vs extracorpuscular Examples of.>")



 Deficiency? Bob Hoffman New York City Poison Center,>")

>")
i.>")


 in the bloodmethemoglobinblood.>")
 WINDSOR UNIVERSITY SCHOOL OF MEDICINE. IVEREN,FOLA,FLOURISH, ALLISON,>")
