Download presentation
Presentation is loading. Please wait.

1
Is Methylene Blue Safe In Patients With Methemoglobinemia And Glucose 6-phosphate Dehydrogenase (G6PD) Deficiency? Bob Hoffman New York City Poison Center, NY, USA

2
Overview Review of G6PD deficiency Review of methemoglobinemia (very brief) Review of methylene blue (MB) (brief) Attempt to answer the question –Expert opinion –Case reports –In Vitro data
 Review of methylene blue (MB) (brief) Attempt to answer the question –Expert opinion –Case reports –In Vitro data")
3
Introduction G6PD deficiency – one of the most common inherited disorders, 400 million people affected –Largely in tropical and subtropical countries Selection advantages –Against Plasmodium falciparum infection Most affected individuals asymptomatic, but the risk of acute hemolysis is well known

4
Frequency of G6PD deficiency

5
Genetics > 400 variants described Different electrophoretic mobility, kinetic properties. 5 classes according to the residual enzyme activity based (WHO). Mediterranean and African (A-) variants –The most clinically significant. Activity scarcely detectable in the Mediterranean type but close to normal in the African variant.
. Mediterranean and African (A-) variants –The most clinically significant. Activity scarcely detectable in the Mediterranean type but close to normal in the African variant..")
6
Inheritance of G6PD Deficiency

8
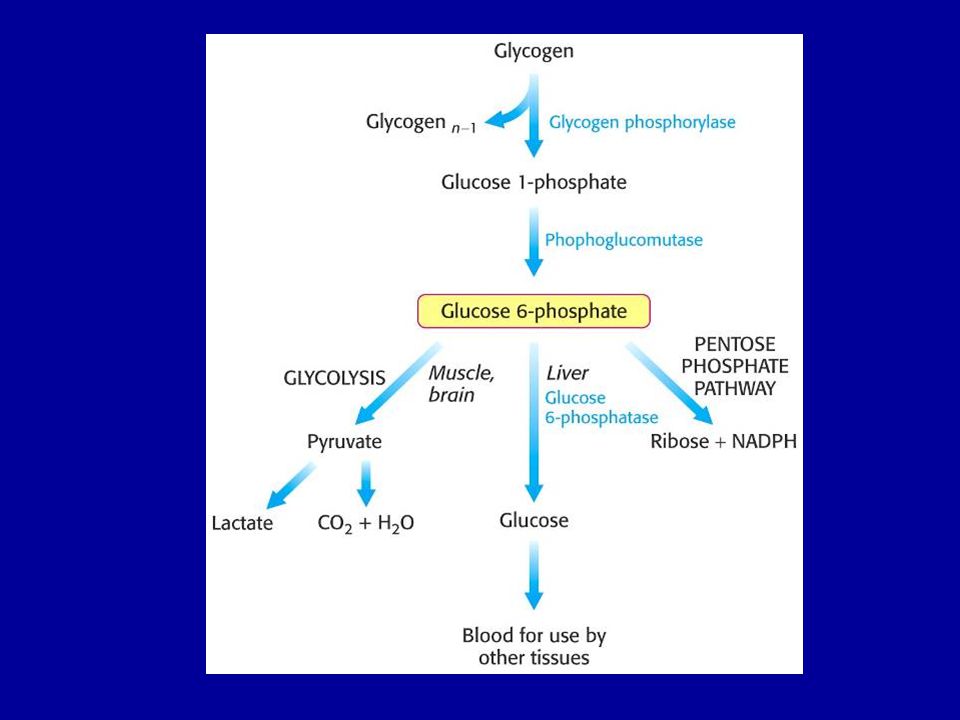
What Do We Need G6PD For? Phosphogluconate pathway Pentose phosphate pathway Hexose monophosphate pathway Hexose monosphosphate shunt

10
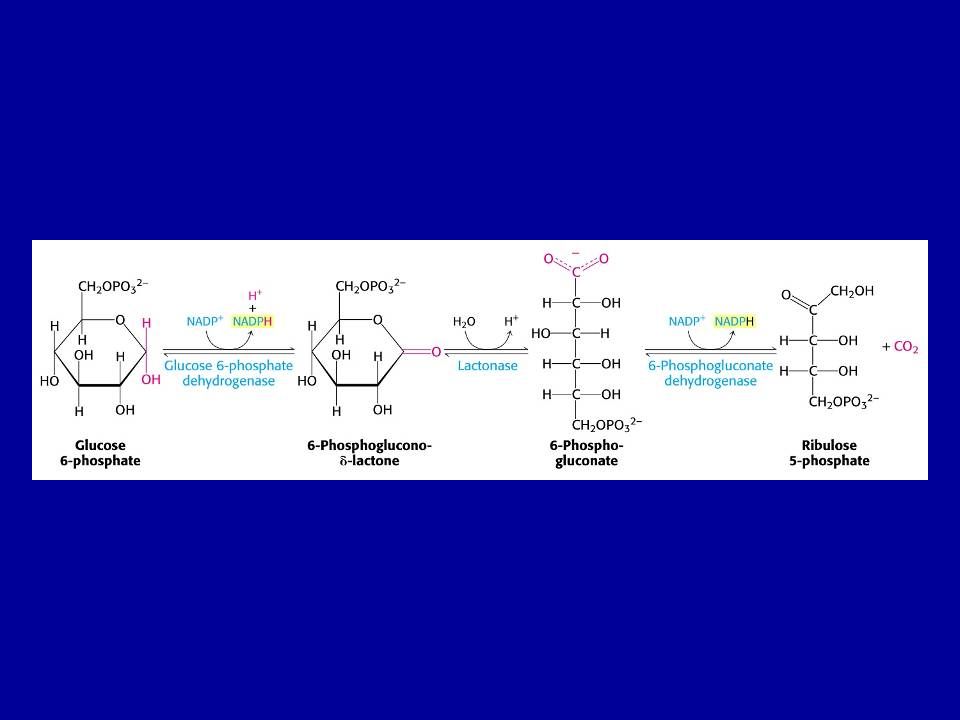
G6PD Catalyzes the first step in the pentose phosphate pathway

11
Regulatory enzyme The enzyme is highly specific for NADP + ; the K m for NAD + is 1000 greater than for NADP +.

13
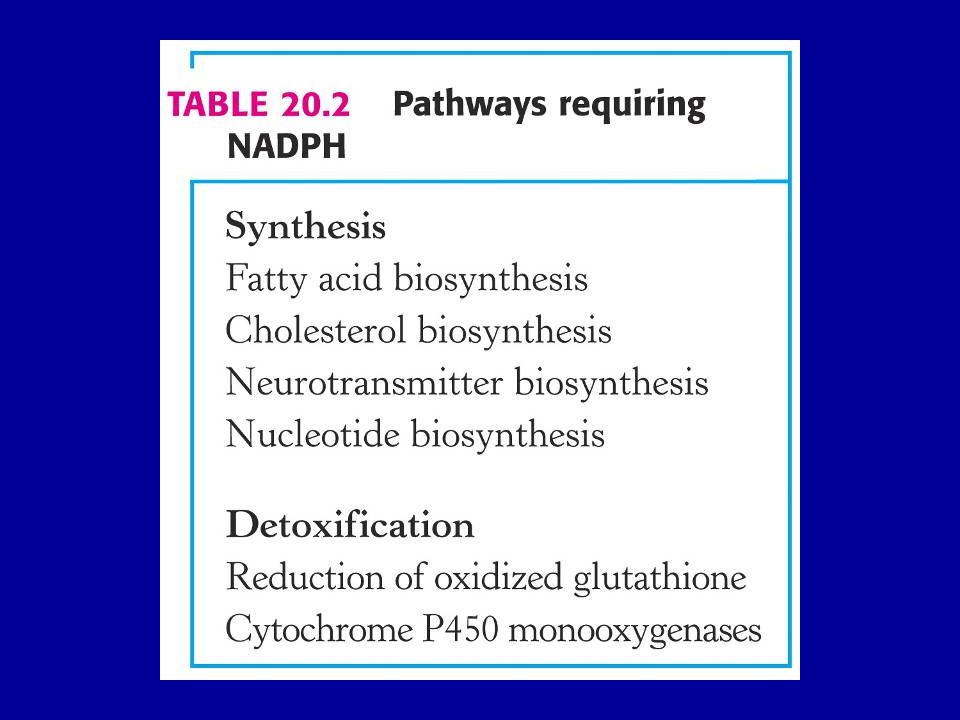
Pentose Phosphate Yields Ribulose (ribose) 5-phosphate –Essential nucleotide in biosynthesis leading to: DNA RNA Various cofactors –CoA, FAD, SAM, NAD + /NADP +
 5-phosphate –Essential nucleotide in biosynthesis leading to: DNA RNA Various cofactors –CoA, FAD, SAM, NAD + /NADP +")
15
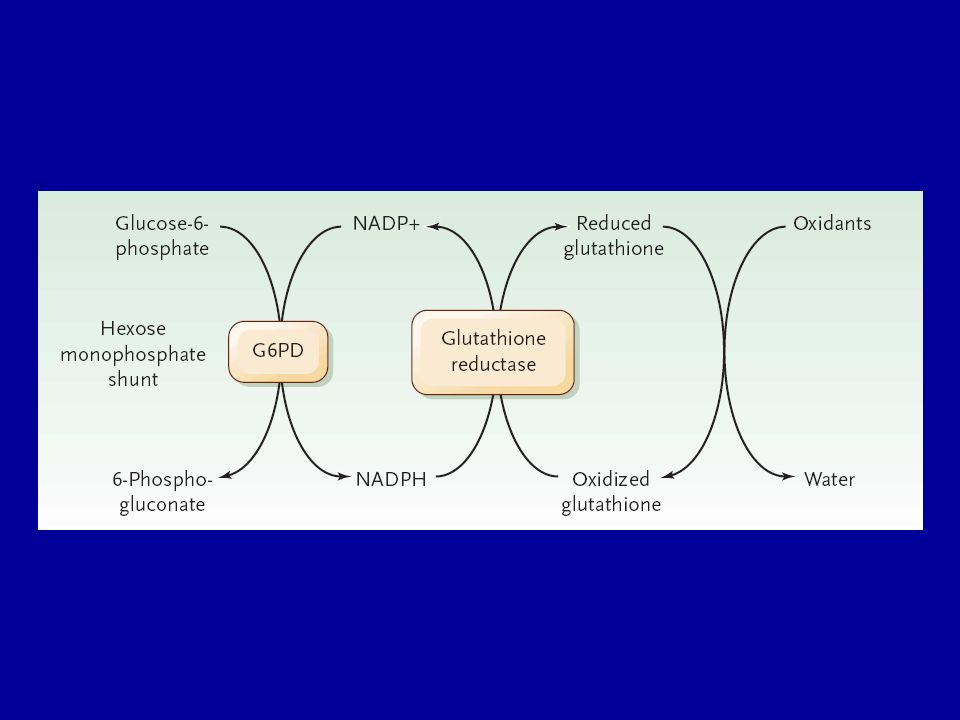
Glutathione reductase uses NADPH as a cofactor to reduce GSSG back to two moles of GSH.

16
G6PD Deficiency G6PD deficiency is not the absence of G6PD, it is a decreased activity –Many cells express G6PD –Red cells are the only important cell line because they lack a nucleus –Activity of G6PD highest (normal) in young erythrocytes and decreases with aging –Oxidants preferentially destroy senescent red blood cells
 in young erythrocytes and decreases with aging –Oxidants preferentially destroy senescent red blood cells")
17
Response to Oxidants

18
Oxidant Response If not reduced: –Some produce hemolysis Oxidation of the hemoglobin chain –Some produce MetHb Oxidation of iron –Some produce both?

19
Physiology Direct reduction of the oxidant Oxidant Reduced Oxidant Glutathione Sulfhydryls Ascorbate Catalase

21
RBCs with Heinz Bodies Precipitation of hemoglobin due to disulfide bond formation between Hb molecues Upper photo shows distorted RBCs with large Heinz bodies Bottom photo shows RBC stained with methylene blue

22
Methemoglobin Definition Oxidation of the iron molecule in hemoglobin from its normal Fe 2+ to Fe 3+ Fe N N N N histidine O 2- Oxyhemoglobin C O COHb O H H Methemoglobin

23
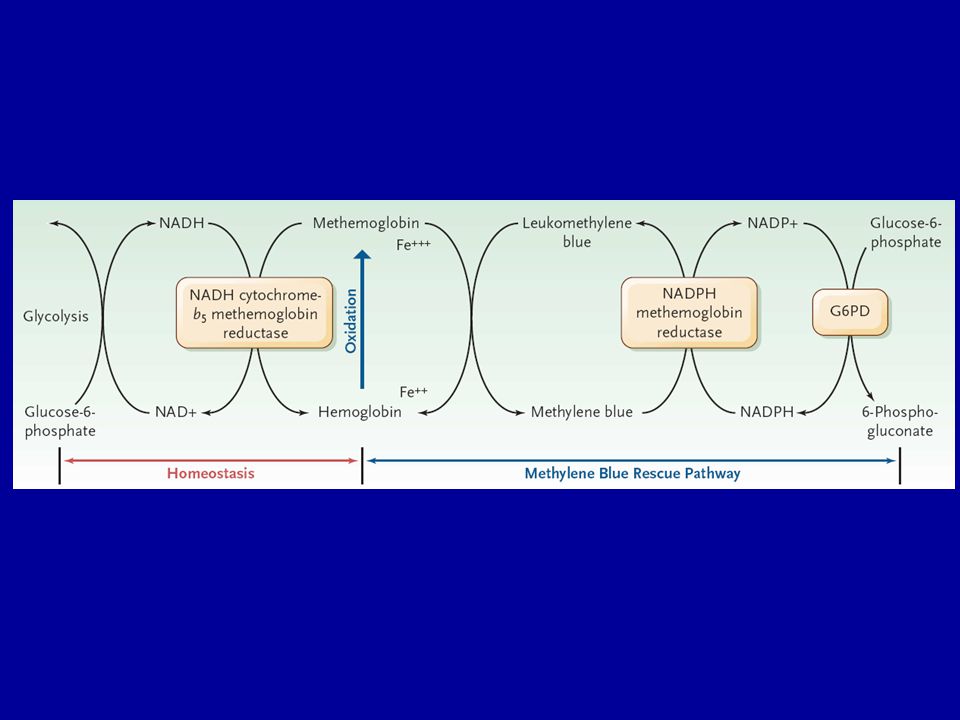
Physiology The oxidant is reduced by Hb (forming MetHb) Then MetHb is reduced back to Hb MetHb Reduced Hb NADH MetHb reductase (67%) Ascorbate (15%) Glutathione (12%) NADPH Met Hb reductase (5%)
 Then MetHb is reduced back to Hb MetHb Reduced Hb NADH MetHb reductase (67%) Ascorbate (15%) Glutathione (12%) NADPH Met Hb reductase (5%)")
25
Can You Use Methylene Blue In Patients with G6PD Deficiency?

26
Famous Textbook Quotes Methylene blue remains the first line therapy even in patients with known G6PD deficiency –Brent Should never be administered to someone with known G6PD deficiency –Shannon Should be used cautiously in patients with G6PD deficiency –Dart

27
28 year old man Ingested 60-120mL of 18% aniline MetHb 11 gm/dL (70-80%) 75 mg methylene blue given Didn’t get better G6PD screening showed deficiency (A - ) Given ascorbate Hemolyzed, Hb fell, recovered –Rosen PJ: Failure of methylene blue treatment in toxic methemoglobinemia. Association with glucose-6-phosphate dehydrogenase deficiency. Ann Intern Med 1971;75:83-6

28
What happened between the 0 and 4 hour levels?

29
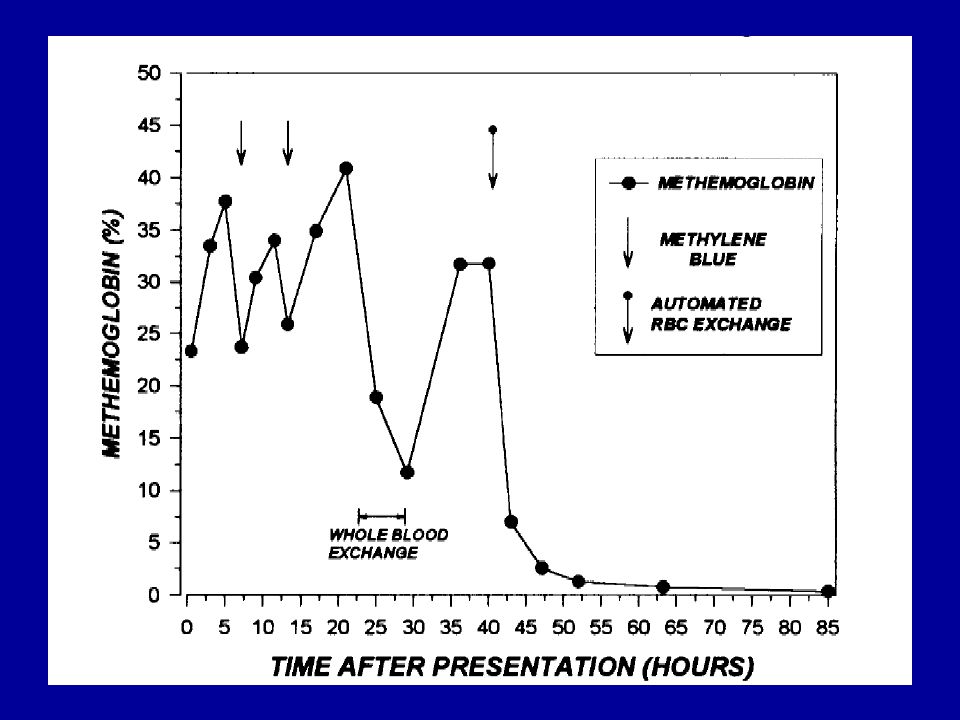
26 month, 9.8-kg boy with G6PD deficiency Ingested 90 mL of nitroethane – MetHb 23.3% MetHb rises to 37%, then over 40% Cyanotic, in respiratory failure, intubated Two doses of methylene blue (2mg/kg) given “without response” No hemolysis Finally treated with exchange transfusion –Golden PJ: Treatment of high-risk, refractory acquired methemoglobinemia with automated red blood cell exchange. J Clin Apher 1998;13:28-31.

31
74 G6PD deficient men 3 day regimen –Chloroquine 1500 mg –Methylene blue 780 mg (mg/kg PO BID) No hemolysis occurred –Mandi G: Safety of the combination of chloroquine and methylene blue in healthy adult men with G6PD deficiency from rural Burkina Faso. Trop Med Int Health. 2005;10:32-8.

32
3 case reports Intraamniotic methylene blue given for PROM (2); IV for maternal MetHb (1) –Dose varied All developed elevated bilirubin Only 2 G6PD deficient –Gauthier TW: Methylene blue-induced hyperbilirubinemia in neonatal glucose-6-phosphate dehydrogenase (G6PD) deficiency. J Matern Fetal Med. 2000;9:252-4.

33
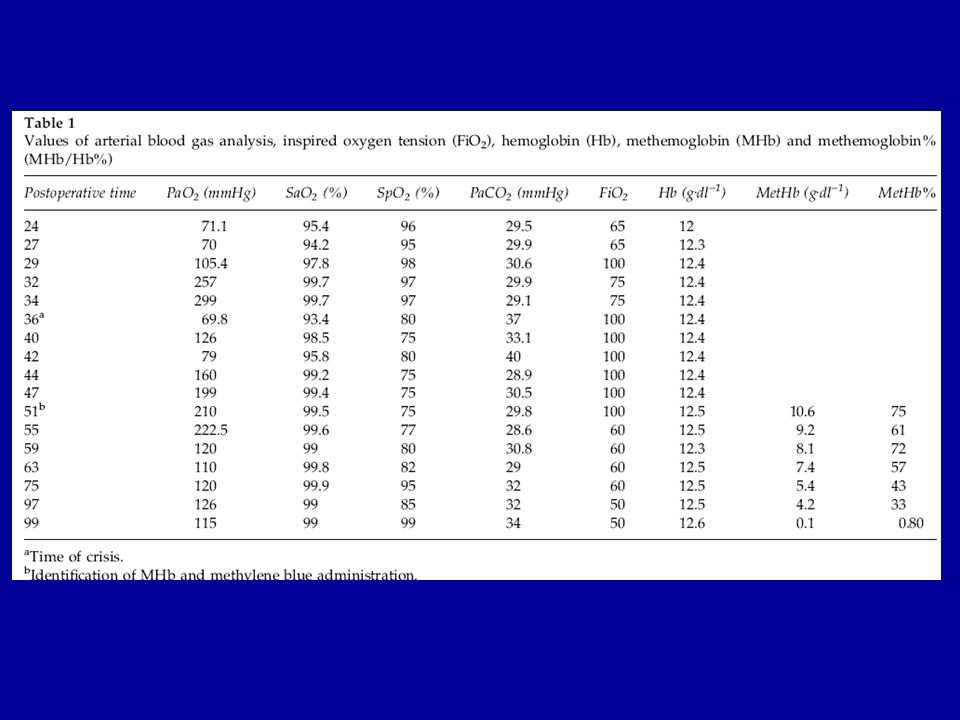
Neonate, known G6PD deficiency Multiple cardiac abnormalities Undergoes surgical repair on day 28 of life Requires nitroglycerin IV Develops MetHb: 75% Given low dose (0.1 mg/kg) methylene blue Has mild hemolysis requiring no therapy –Middali MM: Postoperative methemoglobinemia with associated G-6-P-D deficiency in infant cardiac surgery--enigmas in diagnosis and management. Paediatr Anaesth 2005;15:334-7.

35
59-year-old man with metastatic renal cell CA Trial of 3-aminopyridine-2-carboxaldehyde thiosemicarbazone (3-AP; Triapine) Developed MetHb 35% Given 3 doses (1 mg/kg) methylene blue MetHb fell to 10%, then 6.5 % Masive hemolysis Severe G6PD deficiency confirmed later –Foltz LM: Recognition and management of methemoglobinemia and hemolysis in a G6PD- deficient patient on experimental anticancer drug Triapine. Am J Hematol 2006;81:210-1.

36
Metoclopramide 10 mg administered twice Cyanosis and dyspnea; 28 hours later MetHb was 43% Ascorbic acid 150 mg and methylene blue 60 mg given Consciousness deteriorated Methylene blue 40 mg was repeated at 2 hours Deteriorated rapidly and he died 12 hours Blood taken a before death was hemolysed Postmortem: b5R and severely G6PD deficient –Karadsheh NS: Metoclopramide-induced methemoglobinemia in a patient with co-existing deficiency of glucose-6-phosphate dehydrogenase and NADH-cytochrome b5 reductase: failure of methylene blue treatment Haematologica 2001;86:659

37
25 year old man; large dermal exposure to aniline 5 hours later – MetHb 51% Methylene blue 40mg IV improved symptoms MetHb fell to 2.1% Developed significant hemolysis G6PD deficient Recovered (transfused) –Liao YP: Hemolytic anemia after methylene blue therapy for aniline-induced methemoglobinemia. Vet Hum Toxicol. 2002;44:19-21.

38
In Vivo Summary Does Methylene blue fail? –Often works –Usually slowly Does methylene blue cause hemolysis –It can, and it can be severe –Especially when hemolysis is present prior to therapy

39
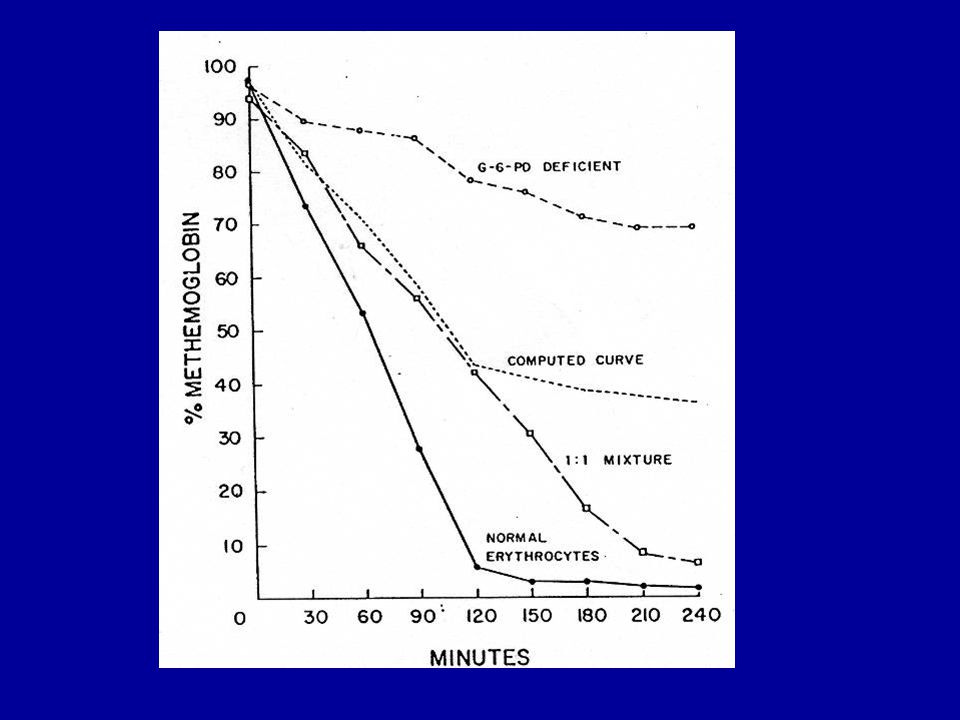
Beutler E: Methemoglobin Reduction: Studies of the interaction between cell popluations and of the role of methylene blue. Blood 1963;22:323-333 Incubated human RBCs with nitrite to induce MetHb Treated with methylene blue and glucose Observed rates of fall –Normal cells –G6PD cells (A - ) –Mixture of cells
 –Mixture of cells.")
41
Implications G6PD deficient cells clear MetHb slowly in response to methylene blue Either NADPH or leukomethylene blue can move from healthy cells to deficient cells This effect is more pronounced at lower levels of MetHb –Young cells and reticulocytes are G6PD present –Role of transfusion (fresh blood)?
")
42
Summary (1) Data on the use of methylene blue in patients with G6PD deficiency are limited –Most support some degree of efficacy –Significant risk of hemolysis Would administer methylene blue in: –Patients with no history of G6PD deficiency –Patients with known G6PD deficiency and life- threatening MetHb Ascorbate, Exchange transfusion, HBO, NAC
 Data on the use of methylene blue in patients with G6PD deficiency are limited –Most support some degree of efficacy –Significant risk of hemolysis Would administer methylene blue in: –Patients with no history of G6PD deficiency –Patients with known G6PD deficiency and life- threatening MetHb Ascorbate, Exchange transfusion, HBO, NAC")
43
Summary (2) Withhold methylene blue in: –Patients with known severe variant G6PD deficiency (Mediterranean) not significantly ill –Patients with known or suspected G6PD deficiency and marginal indications for treatment –Patients with significant active hemolysis in addition to MetHb
 Withhold methylene blue in: –Patients with known severe variant G6PD deficiency (Mediterranean) not significantly ill –Patients with known or suspected G6PD deficiency and marginal indications for treatment –Patients with significant active hemolysis in addition to MetHb")
44
Summary (3) If giving methylene blue to patients with a known or suspected history of G6PD deficiency –Keep the first dose small (1 mg/kg) –Recheck the MetHb often –Do not repeat if unsuccessful –Observe closely for hemoylsis
 If giving methylene blue to patients with a known or suspected history of G6PD deficiency –Keep the first dose small (1 mg/kg) –Recheck the MetHb often –Do not repeat if unsuccessful –Observe closely for hemoylsis")
Similar presentations







 vs extracorpuscular Examples of.>")










i.>")
 Glucose-6-P undergoes two oxidations by NADP +, the second.>")
