Download presentation
Presentation is loading. Please wait.

1
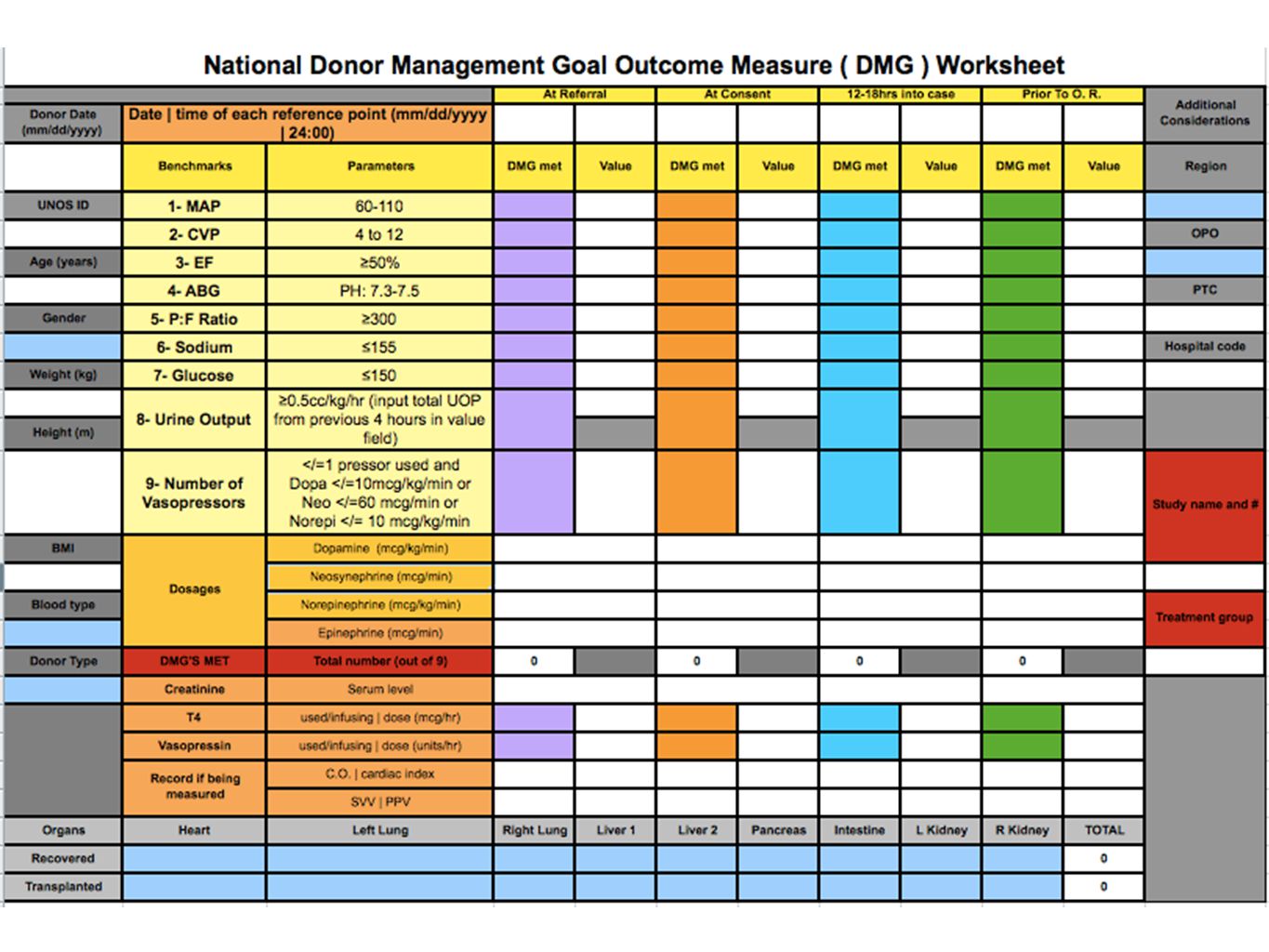
DMG Update UNOS Region 5 Collaborative
December 12, 2012 Darren Malinoski, MD Megan Crutchfield, MPH Section of Surgical Critical Care Portland VA Medical Center

2
Questions to Run On Do these data raise any questions or research ideas? How will you use this information moving forward? I would like to thank all of the members of the region 5 DMG workgroup and would be happy to entertain any questions.

3
The History of DMGs in Region 5
Phase 1 – retrospective – 10 DMGs 2007 Prior to recovery 320 donors Phase 2 – prospective – 9 DMGs July 2008 – July 2010 Three time points 914 donors Phase 3 – prospective – modified the 9 DMGs Aug 2010 – Feb 2012 Four time points 1684 donors Phase 4 – The WEB PORTAL…

5
UNOS Region 5 DMG Web Portal Launched in March – supported by Tii
Linked to DonorNet Forced field entry Generates reports Recipient data added by Tii Fields for study data

6
Regional Update Phase 4 – THE WEB PORTAL Same DMGs as Phase 3
DMGs at four time points Novel parameters: SVV/PPV/swan-ganz Automatic calculations and forced field entries BMI, donor hospital, registry, and research sections Outcome data added daily March 2012 through September 2012

7
Regional Update – Phase 4
807 donors (94% of donors in Unet) 534 SCD 181 ECD 92 DCD 3.23 OTPD (all donors) SCD – 3.78 ECD – 2.35 DCD – 2.02
 534 SCD. 181 ECD. 92 DCD OTPD (all donors) SCD – ECD – DCD –")
8
Phase 4 – organ utilization

9
The History of DMGs in Region 5
Phase 1 – retrospective – 10 DMGs DMGs met in 30% Phase 2 – prospective – 9 DMGs DMGs met in 13%, 29%, and 34% Phase 3 – prospective – modified DMGs DMGs met in 9%, 21%, 48%, and 59% Phase 4 – the WEB PORTAL… DMGs met in 13%, 19%, 42%, and 60%* *(DCDDs and DNDDs used in phase 4)
")
10
Web Portal Reports

11
Association between meeting the DMG Bundle and OTPD
OTPD WHEN DMGs NOT MET VS MET AT EACH TIME POINT REFERRAL AUTHORIZATION 12-18 HOURS PRIOR TO OR NOT MET MET Phase 1 --- 3.34 4.35 Phase 2 3.28 3.92 3.10 3.99 3.02 4.04 Phase 3 3.38 3.35 3.25 3.80 2.87 3.87 2.53 3.88 Phase 4 3.22 3.83 3.13 2.42 Go to 2 decimal points for OTPD and no SD. Bold the ones that have a p <0.05 *(DCDDs and DNDDs used in phase 4), statistics not done yet
, statistics not done yet.")
12
DMG web portal next steps
DMG Workgroup Considerations Add pediatric DMGs Modify existing DMGs Glucose threshold Add insulin dosages Modify report format Add other OPOs

13
Association between Different Glucose thresholds and OTPD
OTPD WHEN GLUCOSE LEVEL MET VS NOT MET AT EACH TIME POINT REFERRAL AUTHORIZATION 12-18 HOURS PRIOR TO OR OTPD p < 150 3.41 0.989 3.45 0.236 3.47 0.450 0.200 > 150 3.35 3.42 3.39 < 180 0.162 0.449 3.44 0.737 3.48 0.015 > 180 3.34 3.29 < 200 3.46 0.102 0.410 0.259 0.006 > 200 3.32 3.40 3.38 3.21

14
Published/presented/ongoing research projects

15
HRSA Mild Hypothermia RCT
HRSA-funded multi-OPO randomized controlled trial Intervention: Mild Hypothermia (34-35C) vs. Normothermia ( ) for > 12 hrs prior to organ recovery Main outcome measures: DGF and SGF Inclusion criteria: hemodynamically stable abdominal organ donors
 vs. Normothermia ( ) for > 12 hrs prior to organ recovery. Main outcome measures: DGF and SGF. Inclusion criteria: hemodynamically stable abdominal organ donors.")
16
HRSA Mild Hypothermia RCT
Enrolled 123 Donors since March 15th 4 hypothermic donors with adverse events Hypokalemia <3.0 x 2 Arrhythmia – SVT and a.fib x 3 Afib – intermittent prior to BD, spontaneous conversion after K replaced (dropped to 2.9) SVT – short run during prep in OR Now replace K to 3.5 prior to enrollment and maintain PEA arrest and rapid recovery of organs in Normothermia group *No hemodynamic instability in Hypothermia group
 SVT – short run during prep in OR. Now replace K to 3.5 prior to enrollment and maintain. PEA arrest and rapid recovery of organs in Normothermia group. *No hemodynamic instability in Hypothermia group.")
17
HRSA Mild Hypothermia RCT
Challenges: Determining when thoracic organs have been ruled out Optimal notification of recipient centers Next Steps: Propose expansion to all research-authorized DNDDs – add thoracic donors Trend towards increase in PaO2:FiO2 over time in hypothermia group (299 to 330, p=0.08) 22 Lungs and 12 Hearts
 22 Lungs and 12 Hearts.")
21
DMG/Variable OR (>4 OTPD) 95% CI p value
Continuous Variables Age (years) 0.944 0.923 – 0.966 < 0.001 Creatinine (mg/dL) 0.636 0.409 – 0.987 0.044 Categorical Variables Thyroid Hormone use 1.969 1.082 – 3.582 0.026 CVP 4 – 10 mmHg 1.897 1.021 – 3.527 0.043 EF > 50% 3.988 2.095 – 7.592 P:F > 300 on PEEP 5 4.591 2.478 – 8.506 Na 135 – 160 mEq/L 3.352 1.141 – 9.851 0.028 “Goals met” 4.394 2.497 – 7.732
 – < Creatinine (mg/dL) – Categorical Variables. Thyroid Hormone use – CVP 4 – 10 mmHg – EF > 50% – P:F > 300 on PEEP – Na 135 – 160 mEq/L – Goals met –")
23
- In press with the American Journal of Transplantation
Variable OR 95% CI p Age (per year) 1.02 0.003 Creatinine prior to recovery (per mg/dL) 1.4 0.001 ECD 0.9 0.664 Cold ischemia time (per hour) 1.03 0.011 DMGs met at consent 0.5 0.019 - In press with the American Journal of Transplantation
 Creatinine prior to recovery (per mg/dL) ECD Cold ischemia time (per hour) DMGs met at consent In press with the American Journal of Transplantation.")
24
Registered Organ Donors Receive Similar Levels of Intensive Care from Donor Hospitals Compared to Non-Registered Donors: An Opportunity to Increase Public Intent to Donate Intent to donate affected by perception that patients with “pink dot” on license will receive less care from doctors Objective: compare the rate of “meeting DMGs” between registered and non-registered donors

25
Not on State Registry (n=489)
Registered Organ Donors Receive Similar Levels of Intensive Care from Donor Hospitals Compared to Non-Registered Donors: An Opportunity to Increase Public Intent to Donate [all donors included] Not on State Registry (n=489) On State Registry (n=144) p value DMGs met at referral 9% 0.846 DMGs met at consent 22% 20% 0.655 DMGs met hours 48% 52% 0.334 DMGs met prior to OR 58% 69% 0.019 OTPD 0.104 -presented at 2012 ATC
 On State Registry (n=144) p value. DMGs met at referral. 9% DMGs met at consent. 22% 20% DMGs met hours. 48% 52% DMGs met prior to OR. 58% 69% OTPD presented at 2012 ATC.")
26
Conclusions Patients who are registered to be organ donors and suffer devastating brain injuries appear to receive the same level of critical care support from their healthcare providers prior to their intent to donate being established as those who are not registered to be organ donors. Registered donors are more likely to meet pre-determined critical care endpoints of resuscitation after consent for organ donation.

29
Variables Associated with Liver Graft Transplantation
Lower Age Lower BMI Male Gender SCD status (vs. ECD) Higher MAP Lower CVP Higher Ejection Fraction Higher PaO2:FiO2 Lower Glucose Vasopressin use To summarize, variables seen to associate with graft transplantation are: the donor demographics of Lower Age and BMI, Male Gender and SCD status ; And the critical care values of Higher MAP, Lower CVP, Higher Ejection Fraction; better oxygenation ratios; Lower Glucose; and the use of Vasopressin
 Higher MAP. Lower CVP. Higher Ejection Fraction. Higher PaO2:FiO2. Lower Glucose. Vasopressin use. To summarize, variables seen to associate with graft transplantation are: the donor demographics of Lower Age and BMI, Male Gender and SCD status ; And the critical care values of Higher MAP, Lower CVP, Higher Ejection Fraction; better oxygenation ratios; Lower Glucose; and the use of Vasopressin.")
30
Variables Associated with Liver Graft Discard
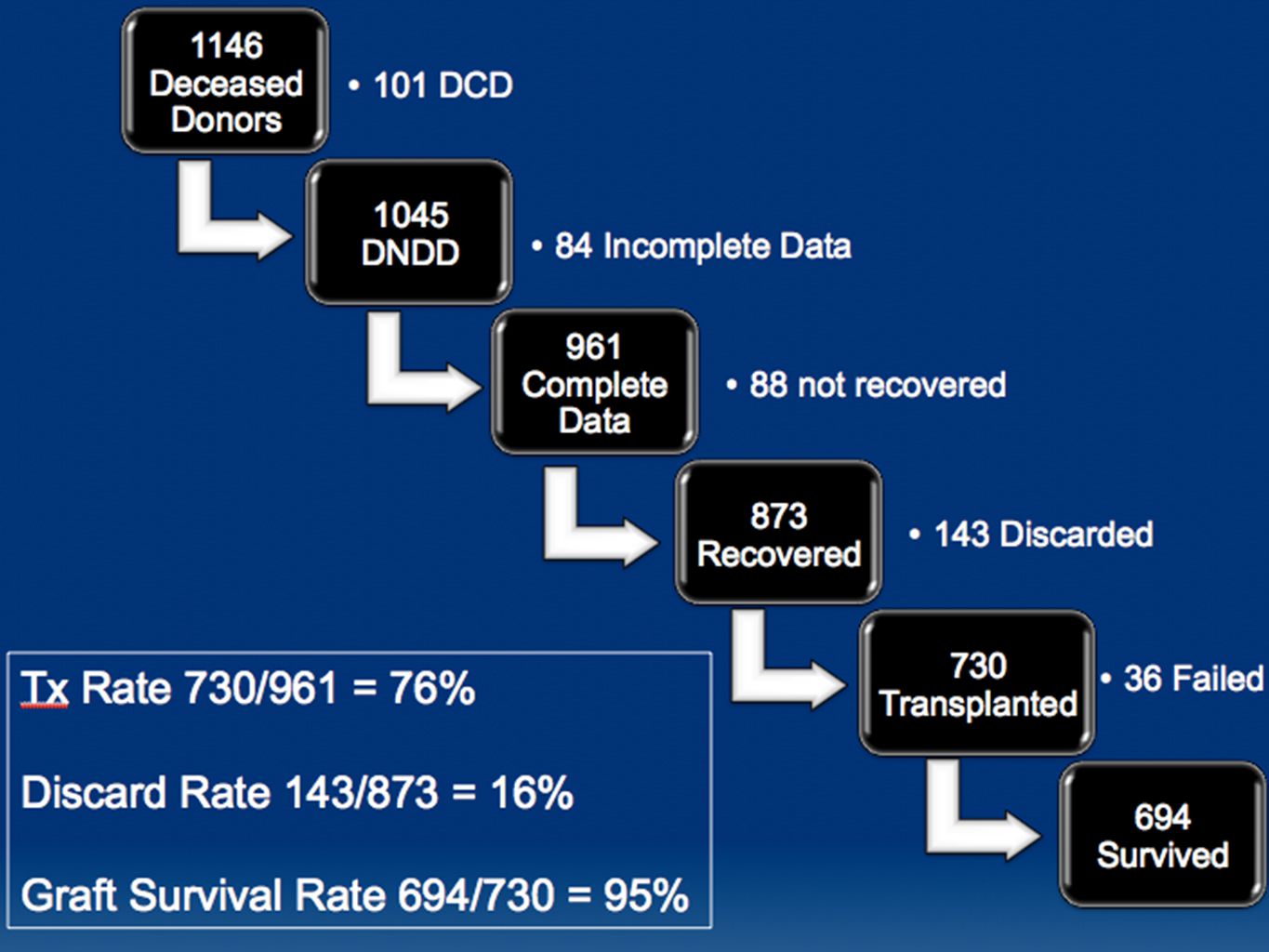
From 873 Procured livers… 730 Livers Transplanted, 143 Livers Discarded (16%) We turned to look at associations with liver graft discards. These were organs which were procured, but ultimately not used for transplant, most likely upon inspection by the transplant surgeons. And of 873 livers, 730 were used
 We turned to look at associations with liver graft discards. These were organs which were procured, but ultimately not used for transplant, most likely upon inspection by the transplant surgeons. And of 873 livers, 730 were used.")
31
Variables Associated with Liver Graft Discard
Older Age Higher BMI Female Gender ECD status (vs. SCD) Higher CVP Lower Urine Output Lower PaO2:FiO2 Lower thyroid hormone dosages The variables we found associated with graft discard were The demographics of Older Age and higher BMI, Female Gender, Extended Criteria Donor status, Higher CVP, Lower Urine Output, worse pulmonary function, Lower doses of thyroid hormone
 Higher CVP. Lower Urine Output. Lower PaO2:FiO2. Lower thyroid hormone dosages. The variables we found associated with graft discard were. The demographics of Older Age and higher BMI, Female Gender, Extended Criteria Donor status, Higher CVP, Lower Urine Output, worse pulmonary function, Lower doses of thyroid hormone.")
32
Variables Associated with Liver Graft Survival
730 Livers Transplanted 694 (95%) survival after 74±73 days Finally we analyzed the livers were used for transplant, which were 730 in number. At a mean follow-up of 74 days ( and some had much longer follow up) 95% of grafts were still functioning. These grafts were associated with the Donor demographics of lower age, lower BMI and SCD status. Gender was not important. Variable Graft Survival vs. Failure Age (years) 38 vs. 44 BMI (kg/m2) 26 vs. 30 SCD 96% vs. 91% Male Gender 96% vs. 94%
 survival after 74±73 days. Finally we analyzed the livers were used for transplant, which were 730 in number. At a mean follow-up of 74 days ( and some had much longer follow up) 95% of grafts were still functioning. These grafts were associated with the Donor demographics of lower age, lower BMI and SCD status. Gender was not important. Variable. Graft Survival vs. Failure. Age (years) 38 vs. 44. BMI (kg/m2) 26 vs. 30. SCD. 96% vs. 91% Male Gender. 96% vs. 94%")
33
Variables Associated with Liver Graft Survival
Cold Ischemia Time did not differ 7.4 vs. 7.7 hours, p=0.675 None of the critical care endpoints or medications were associated with graft survival In this analysis, the cold ischemia time did not differ between surviving and failing grafts. But what was interesting was that none of the DMGs obtained, or medications used were associated with graft survival. Does that mean that nothing I do in the ICU can impact on graft survival? It is possible that the care provided across the board is becoming increasingly more uniform, and there were few donors with only very low numbers of critical care endpoints met. Its also likely that transplant surgeons are getting more experience at rejecting organs that are likely to fail, because the overall failure rate of 5% is low. I’d like to think that, The selection process may have already chosen for livers managed well, and so they went on to do well. Clearly Important, recipient medical demographics and are not included in this analysis

34
Conclusions Donor age, BMI, SCD status, and gender are associated with both liver graft transplantation and discard rates Lower donor age, BMI, and SCD status are associated with graft survival rates Among the fixed Donor characteristics, we found that Donor Age, BMI, SCD, and gender were associated with both graft utilization and graft discard rates But among the organs then selected for transplant, only donor age, BMI, and SCD are associated with graft survival.

38
Questions to Run On Do these data raise any questions or research ideas? How will you use this information moving forward? I would like to thank all of the members of the region 5 DMG workgroup and would be happy to entertain any questions.

Similar presentations



















 patients Policy.>")




