Download presentation
Presentation is loading. Please wait.

1
Effects of introducing then removing cost-sharing for drugs among people with schizophrenia in Quebec: A natural experiment Eric Latimer, Ph.D. Canadian Health Economics Study Group May 27 2010

2
Co-authors Willy Wynant, M.S. 1 Adonia Naidu, M.Sc. 2 Robin Clark, Ph.D. 3 Ashok Malla, M.D. 2,4 Erica Moodie, Ph.D. 1 Robyn Tamblyn, Ph.D. 1 1 Department of Epidemiology, Biostatstics and Occupational Health, McGill University 2 Douglas Mental Health University Institute 3 Department of Psychiatry, McGill University 4 Family Medicine and Community Health, Center for Health Policy and Research, University of Massachusetts Medical School Acknowledgement: Michal Abrahamowicz for contribution to original study design

3
Study funding Fonds de la recherche en santé du Québec

4
BACKGROUND

5
Schizophrenia Disabling mental illness Several subtypes Positive and negative symptoms Usually develops around 18 for males, 25 for females (plus or minus several years) About 1% of the population
 About 1% of the population")
6
Antipsychotics Help control positive symptoms (psychotic episodes) Reduce re-hospitalisations Significant side-effects Ineffective for 20 to 30% of people with schizophrenia
 Reduce re-hospitalisations Significant side-effects Ineffective for 20 to 30% of people with schizophrenia")
7
Introduction of cost-sharing in August 1996 For welfare recipients and seniors Welfare recipients: ceiling of $50 per quarter $16.67 per month for people with mental illness Tamblyn et al. 2001: Reduction in use of medications Increase in adverse events (deaths, hospitalizations and nursing homes) and ER visits
 and ER visits.")
8
Consistent with other studies Ward et al. 06 (and others): Antipsychotics compliance: Hospitalisations Suicides, mortality Soumerai et al. 94: Capping prescriptions for people with schizophrenia in NH: Antipsychotics Emergency psychiatric services Government costs
: Antipsychotics compliance: Hospitalisations Suicides, mortality Soumerai et al. 94: Capping prescriptions for people with schizophrenia in NH: Antipsychotics Emergency psychiatric services Government costs.")
9
Selective removal of cost- sharing in October 1999 For welfare recipients classified as disabled Includes people with schizophrenia classified as disabled, who typically consume antipsychotics No studies of effects of removing cost- sharing for antipsychotics identified

10
Qualitative interviews

11
In 2004-2005, 23 interviews with psychiatrists, nurses and social workers were conducted at 8 different sites in 6 Québec cities or towns Consumers considered, but not included for reasons of efficiency (many interviews needed to obtain representative sample) Urban and rural, teaching and non-teaching sites included Questions on various topics, including of relevance here: Effects of introducing, then removing cost- sharing on people with schizophrenia
 Urban and rural, teaching and non-teaching sites included Questions on various topics, including of relevance here: Effects of introducing, then removing cost- sharing on people with schizophrenia")
12
Main comments from qualitative interviews Some schizophrenia patients more closely followed than others – cost- sharing would have bigger impact on them Removal of cost-sharing expected to have smaller impact

13
OBJECTIVES Re-evaluate impact of introducing cost- sharing on use of medications, for people with schizophrenia, with larger sample Evaluate impact of removing cost- sharing 39 months later

14
Data

15
Identification of patients Data extracted for people who had at least one prescription of antipsychotics between Jan, 1 st 1993 and Dec, 31 st 2004 while on welfare status 107,005 individuals Extracted from RAMQ: Welfare status Prescription data (DIN, duration, dose, charge, etc.) Medical service data (type of service, Dx, etc.) Extracted from Med-Echo: Hospitalization data (Adm. & discharge dates, Dx, etc.)
.")
16
Data cleaning

17
Data cleaning procedures on prescription data Conservative methods to ensure that all the corrections are plausible. When a value seems incorrect, either: At least 2 arguments concur to correct a value and we make this correction Or we drop this prescription Focus on cost, quantity and duration fields

18
Numbers of prescriptions affected by data cleaning (based on 03 and 04 data only) Problems of duration of prescription (number of days) = 0 & quantity of drug (i.e., total number of pills or ml) = 0 & drug cost = 0 when all not equal to zero but at least one equal to zero 442 (0.02%) prescriptions are concerned Duration of prescription > 270 days 131 (0.01%) prescriptions, only 7 could be corrected Problem with the ratio cost to quantity 91 (<0.01%) prescriptions were concerned, no one could be corrected Problem of low dose 34 (<0.01%) prescriptions were concerned, only 4 could be corrected Patients with prescriptions that could not be corrected were eliminated from the study
 Problems of duration of prescription (number of days) = 0 & quantity of drug (i.e., total number of pills or ml) = 0 & drug cost = 0 when all not equal to zero but at least one equal to zero 442 (0.02%) prescriptions are concerned Duration of prescription > 270 days 131 (0.01%) prescriptions, only 7 could be corrected Problem with the ratio cost to quantity 91 (<0.01%) prescriptions were concerned, no one could be corrected Problem of low dose 34 (<0.01%) prescriptions were concerned, only 4 could be corrected Patients with prescriptions that could not be corrected were eliminated from the study")
19
Adjustment of prescription durations

20
Adjustments of the prescriptions: why? If we draw successions of prescriptions for some patients we observe different patterns : Jan, 1 st Jan, 14 th Jan, 12 th Jan, 25 th Jan, 1 st Jan, 15 th Jan, 1 st Jan, 12 th Pills are lost 2 pills these days 1/ 2/ 3/ Could be interpreted as 2 prescriptions of the same DIN:

21
Bases for adjustment of the prescription start dates and durations Consulted community pharmacist near Douglas Institute A renewal less than 20% ahead of end of previous prescription is assumed to be an early refill But, since a pharmacist must justify to the RAMQ why s/he would have accepted to fill a renewal prescription if the patient asks for a refill more than 20% too early, we do not do this automatically in such a case. Consecutive refills that are more than 20% too early suggest a problem – normally such events, if accepted by the pharmacist, are rare (e.g., going on vacation, lost pills) It could be an increase in dose It could be an early renewal, concurrent with a new prescription, to synchronize the prescriptions
 It could be an increase in dose It could be an early renewal, concurrent with a new prescription, to synchronize the prescriptions.")
22
Adjustment of the prescriptions: algorithm Two prescriptions of the same DIN and the same dosage overlapped (even by more than 20%): we moved the start date of the prescription forward, to make the prescription begin when the previous one ended Except if it was a too early renewal for the second time: we supposed that this prescription began when it was filled and that the remaining pills were lost. Synchronized prescriptions = if there was a synchronization (two or more DINs filled on the same day) the prescription was considered as beginning when filled and the previous one was stopped (considered as if the pills were lost)
 the prescription was considered as beginning when filled and the previous one was stopped (considered as if the pills were lost).")
23
Adjustments of the prescriptions: hospitalizations Sometimes a patient was supposed to fill a prescription during a hospitalization (even when the hospitalization was for a psychiatric reason). We supposed that all these pills were lost When a hospitalization occurred at a time when the patient was on a prescription we supposed that all the pills from that prescription were not taken anymore and were considered as lost

24
Construction of the cohort On welfare from 1993 to 2004 (ignoring interruptions < 1 month) 18+ in 1995 and alive in 2004 At least one prescription of antipsychotics every 180 days from Jan 1 st 1993 to July 31 st 1996, removing hospitalization days Schizophrenia Dx either on hospitalization records OR medical records one or more times in the period 1993 – July 31 st 1996 N=4,401
 18+ in 1995 and alive in 2004 At least one prescription of antipsychotics every 180 days from Jan 1 st 1993 to July 31 st 1996, removing hospitalization days Schizophrenia Dx either on hospitalization records OR medical records one or more times in the period 1993 – July 31 st 1996 N=4,401")
25
Proportion of days in month patient had access to antipsychotics Proportion of days in month that antipsychotics available while in community Adjustment for hospitalisations < 10 days in community : Proportion undefined

26
First 9 months of 1993 excluded No data from 1992 Don’t know when 1992 prescriptions end Maximum prescription duration is 9 months

28
Estimation strategy Test for fixed effects or random effects Allow for different intercepts, linear and quadratic time trends during pre-cost- sharing, cost-sharing, and post-cost- sharing periods

29
Results

30
Age and sex by stability subgroup

33
Average APR in 6 months prior to cost-sharing introduction minus average APR in 6 months after cost- sharing introduced (N=4401) Median difference= 0.005Mean difference= 0.046
 Median difference= 0.005Mean difference= 0.046")
34
Average APR during 6 months after cost- sharing removed minus average APR during 6 months prior to cost-sharing removal (N=4401) Median difference= 0 Mean difference=.0174596
 Median difference= 0 Mean difference=")
35
Hausman test Rejected at p<0.01 Use fixed effects

38
Regression: High Stability Subgroup (N=1466)
")
39
Regression: Medium Stability Subgroup (N=1501)
")
40
Regression: Low Stability Subgroup (N=1434)
")
41
Sensitivity analysis Remove values 3 months before and 3 months after August 1 1996 and October 1 1999 To mitigate any effects of stockpiling or delaying purchasing of medications in anticipation of policy change Results qualitatively similar

42
Discussion

43
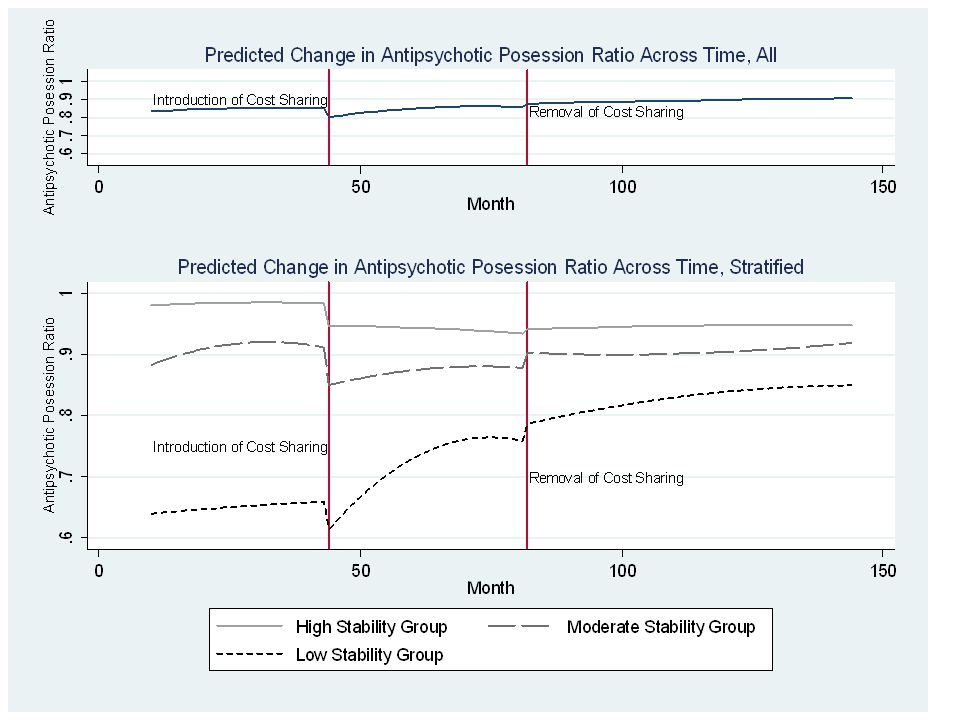
Conclusions High-stability group: Permanent reduction in APR, small effect of removing cost-sharing Other groups: Long-term trends towards increased consumption Apparently greater effect of removing cost- sharing

44
Limitations Non-experimental design: possible confounding CV classification crude Schizophrenia Dx identification Fixed cohort – drop-outs (welfare exit, death) ignored, possible bias
 ignored, possible bias")
45
Implications Removing cost-sharing was effective policy Permanent effect of having introduced cost-sharing – especially for high stability group Further evidence that cost-sharing for antipsychotics undesirable

Similar presentations






-Armenia Migration and Remittances: Data from CRRC DI Surveys Yerevan April 29, 2008>")

 AcademyHealth Meeting, Seattle, June 25, 2006.>")














