Download presentation
Presentation is loading. Please wait.

1
Allergic Bronchopulmonary Aspergillosis (ABPA)
CF cases are slightly different (eg, criteria for dx, lab values)
")
2
ABPA – Definition and Epidemiology
Hypersensitivity reaction d/t colonization of bronchi by Aspergillus bronchial obstruction, inflammation, mucous plugging bronchiectasis, fibrosis, resp failure Occurs primarily in pts w/ asthma (prevalence = 1-2%) or CF (prevalence = 1-15%) Most cases present in the 3rd to 4th decade No gender predilection Some pts have (+) family history of ABPA
 or CF (prevalence = 1-15%) Most cases present in the 3rd to 4th decade. No gender predilection. Some pts have (+) family history of ABPA.")
3
Pathophyisology Incompletely understood
Genetic predisposition + inhalation of Aspergillus fumigatus spores (that later germinate into hyphae and release antigens) 1) Airway barrier compromise (in part by dec’d mucociliary clearance, and action of proteolytic and mycotoxins) 2) Activation of innate lung immunity Influx of inflammatory cells 3) Presentation of antigens to T cells Activation of Th2 cells and inc’d production of Th2 cytokines (Il-4, -5, and -13) Inc’d total and A fumigatus-specific IgE, mast cell degranulation, and eosinophilic response. 4) Also Type III (IgG and IgA) hypersensitivity reactions “No apparent relation b/w intensity of exposure to airborne Aspergillus spores and rates of sensitization to the fungus as measured by skin testing”.
 1) Airway barrier compromise (in part by dec’d mucociliary clearance, and action of proteolytic and mycotoxins) 2) Activation of innate lung immunity Influx of inflammatory cells. 3) Presentation of antigens to T cells Activation of Th2 cells and inc’d production of Th2 cytokines (Il-4, -5, and -13) Inc’d total and A fumigatus-specific IgE, mast cell degranulation, and eosinophilic response. 4) Also Type III (IgG and IgA) hypersensitivity reactions. No apparent relation b/w intensity of exposure to airborne Aspergillus spores and rates of sensitization to the fungus as measured by skin testing .")
4
Pathology Varies b/w different patients and w/in different lung ares w/in a pt Typical Histology Mucus, fibrin, Curschmann spirals, Charcot-Leyden crystals, inflammatory cells (primarily eosinophils). Hyphae can often be seen in the bronchiectatic cavities Other Possible Findings Fungal growth in lung parenchyma Non-caseating granulomas w/ eosinophils and multi-nucleated giant cells centered on airways Invasive aspergillosis (rare)
. Hyphae can often be seen in the bronchiectatic cavities. Other Possible Findings. Fungal growth in lung parenchyma. Non-caseating granulomas w/ eosinophils and multi-nucleated giant cells centered on airways. Invasive aspergillosis (rare)")
5
Clinical Presentation
Common Sxs Low-grade fever Wheezing Bronchial hyperactivity Hemoptysis Productive cough (often w/ expectoration of brownish black sputum) Occasionally aSx’c and dx’d on routine screening (eg, 2/2 aSx’c consolidation).
 Occasionally aSx’c and dx’d on routine screening (eg, 2/2 aSx’c consolidation).")
6
Physical Exam Can be normal Other possible findings include:
Polyphonic wheezing Clubbing (16%) Coarse crackles (15%) Sxs of pulmonary HTN and/or respiratory failure
 Coarse crackles (15%) Sxs of pulmonary HTN and/or respiratory failure.")
7
Dx'c Criteria Major Criteria: (? 6 of 8 needed for dx) 2 Types
1) H/o asthma 2) Immediate skin test reactivity to Aspergillus antigens 3) Precipitating serum Abs to A. fumigatus 4) Serum total IgE > 1000 ng/mL (can be lower if on steroids) 5) Peripheral eosinophilia > /mm(3) 6) Infiltrates on CXR or HRCT 7) Central bronchiectasis on chest CT 8) Elev’d specific serum IgE and IgG to A. fumigatus Other Common Findings -- Expectoration of mucous plugs. Aspergillus in sputum, late skin reactivity to Aspergillus Ag 2 Types ABPA-CB (central bronchiectasis) -- 1, 2, 4, 7, 8 ABPA-S (seropositive) -- 1, 2, 3, 4 but NO accompanying central bronchiectasis No one dx’c test. Criteria are controversial and continue to be modified d/t the lack of evidence on the # of criteria needed Skin test -- Uses A fumigatus antigen. Test is read q 15 min x 1 hr and again at 6-8 hours. Interpretation Type I ( 1 of the characteristic findings of ABPA) - (+) wheal and erythema after 1 min that reaches maximum intensity after min, and resolves w/in 1-2 hours. Indicates presence of A fumigatus specific IgE Abs Type III (immune complex hypersensitivity) - Any amount of subcut edema after 6 hours. Often do skin test first. If this is (-) as is intradermal reactivity to Aspergillus, ABPA is essentially excluded. If skin prick is (+), check total serum IgE and precipitans to Aspergillus. If IgE < 1000 or if precipitans are (-), Aspergillus is excluded.
 H/o asthma. 2) Immediate skin test reactivity to Aspergillus antigens. 3) Precipitating serum Abs to A. fumigatus. 4) Serum total IgE > 1000 ng/mL (can be lower if on steroids) 5) Peripheral eosinophilia > /mm(3) 6) Infiltrates on CXR or HRCT. 7) Central bronchiectasis on chest CT. 8) Elev’d specific serum IgE and IgG to A. fumigatus. Other Common Findings -- Expectoration of mucous plugs. Aspergillus in sputum, late skin reactivity to Aspergillus Ag. 2 Types. ABPA-CB (central bronchiectasis) -- 1, 2, 4, 7, 8. ABPA-S (seropositive) -- 1, 2, 3, 4 but NO accompanying central bronchiectasis. No one dx’c test. Criteria are controversial and continue to be modified d/t the lack of evidence on the # of criteria needed. Skin test -- Uses A fumigatus antigen. Test is read q 15 min x 1 hr and again at 6-8 hours. Interpretation. Type I ( 1 of the characteristic findings of ABPA) - (+) wheal and erythema after 1 min that reaches maximum intensity after min, and resolves w/in 1-2 hours. Indicates presence of A fumigatus specific IgE Abs. Type III (immune complex hypersensitivity) - Any amount of subcut edema after 6 hours. Often do skin test first. If this is (-) as is intradermal reactivity to Aspergillus, ABPA is essentially excluded. If skin prick is (+), check total serum IgE and precipitans to Aspergillus. If IgE < 1000 or if precipitans are (-), Aspergillus is excluded.")
8
Radiographic Features - CXR
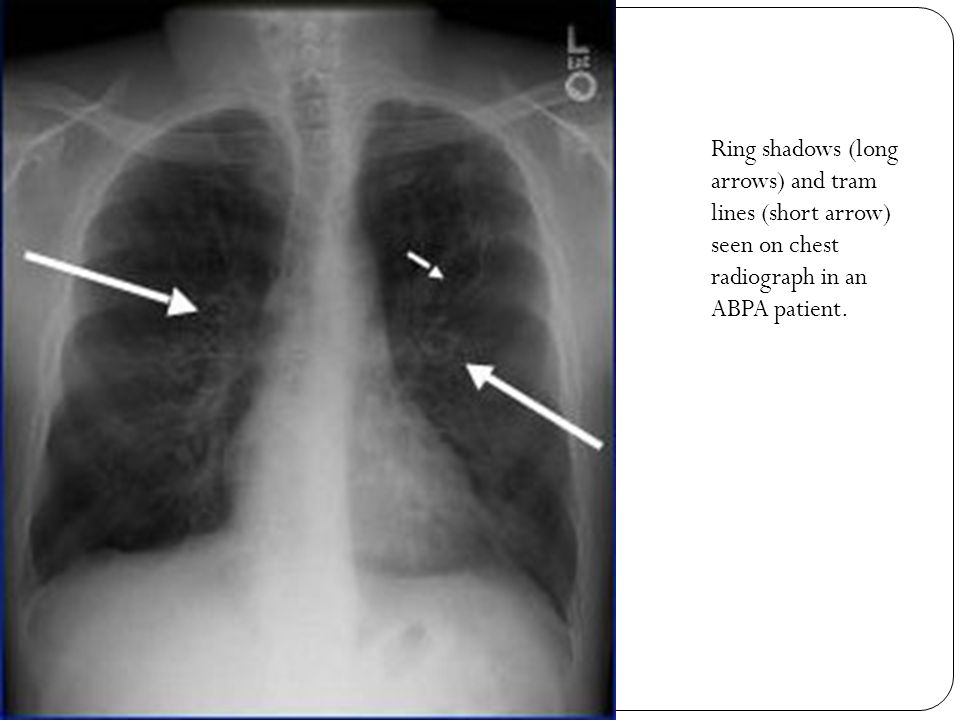
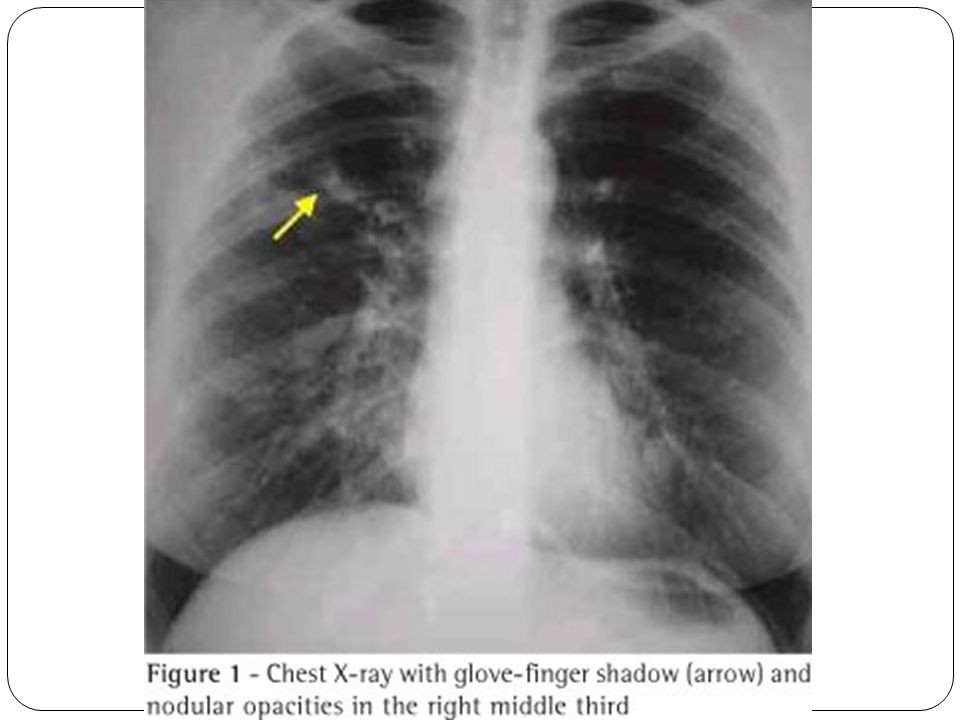
Parenchymal infiltrates (generally of upper lobes) Atelectasis d/t mucous plugging Findings c/w bronchiectasis “Tram line” shadows d/t thickened non-dilated bronchial walls “Parallel lines” d/t ectactic bronchi Ring shadows d/t mucous filled bronchi or small abscesses “Toothpaste shadows” d/t mucous plugging in 2nd to 4th order bronchi “Gloved finger shadows” (branched tubular radiodensities, 2-3 cm long, 5-8 cm wide, extending from the hilum) d/t intrabronchial exudates w/ bronchial wall thickening
 Atelectasis d/t mucous plugging. Findings c/w bronchiectasis. Tram line shadows d/t thickened non-dilated bronchial walls. Parallel lines d/t ectactic bronchi. Ring shadows d/t mucous filled bronchi or small abscesses. Toothpaste shadows d/t mucous plugging in 2nd to 4th order bronchi. Gloved finger shadows (branched tubular radiodensities, 2-3 cm long, 5-8 cm wide, extending from the hilum) d/t intrabronchial exudates w/ bronchial wall thickening.")
10
Ring shadows (long arrows) and tram lines (short arrow) seen on chest radiograph in an ABPA patient.
11
Radiographic Findings - HRCT
Widespread proximal cylindrical bronchiectasis (mostly of upper lobes) Bronchial wall thickening Mucous plugging Atelectasis Peripheral airspace consolidation Ground-glass attenuation Mosaic perfusion Air trapping
 Bronchial wall thickening. Mucous plugging. Atelectasis. Peripheral airspace consolidation. Ground-glass attenuation. Mosaic perfusion. Air trapping.")
12
Top R - Bilateral central bronchiectasis w/ centrilobular nodules & tree-in-bud opacities in L lung.
Top L - Bilateral central bronchiectasis w/ many mucus-filled bronchi. Bottom L & R - High- attenuation mucoid impaction.

13
PFTs Not really used in dx’g ABPA but findings can show
Airflow obstruction Mixed obstructive and restrictive pattern if bronchiectasis or fibrosis Air trapping Dec’d FEV1 and RV (+) Bronchodilator response in < 50%
 Bronchodilator response in < 50%")
14
Stages of ABPA (not necessarily progressive)
Stage I = Acute flare Infiltrates, markedly elev’d IgE Stage II = Remisson No infiltrates, off steroids > 6 mos, elev’d or NL IgE Stage III = Recurrent exacerbations Stage IV = Glucocorticoid-dependent asthma Infiltrates present intermittently or not at all, elev’d or NL IgE Stage V = Fibrotic (end stage) lung dz Fibrotic, bullous, cavitary lung lesions, IgE may be normal
 lung dz. Fibrotic, bullous, cavitary lung lesions, IgE may be normal.")
15
Tx - Goals 1) Early control of immunologic activity / inflammation to try to prevent progression to bronchiectasis and fibrosis 2) Monitoring for response and early detection of relapses 3) ?? Dec fungal burden in airways
 Monitoring for response and early detection of relapses. 3) Dec fungal burden in airways.")
16
Tx - Steroids Doses vary depending on stage and prescriber preference. Higher dosages for longer durations may be more effective for tx’g flares. Stages 1 & 3 – Prednisone mg/kg Qday x 14 days, then QOD x 6-8 wks, then taper by 5-10 mg q 2 weeks until d/c’d Should see resolution of infiltrates and 35-50% dec in serum total IgE (measured q1-2 months during acute treatment) Stage 2 – Steroids not needed. Monitor IgE q6 months x 1 year then q 1-2 years. Doubling of baseline IgE indicates relapse (stage 3) Stage 4 – Steroid dependent. Aim for lowest possible dose Stage 5 – Steroids not helpful Steroid “prophylaxis” – Ca, Vit D, bisphosphonate Need systemic form (inhaled form may help w/ underlying asthma but has no efficacy in ABPA)
 Stage 2 – Steroids not needed. Monitor IgE q6 months x 1 year then q 1-2 years. Doubling of baseline IgE indicates relapse (stage 3) Stage 4 – Steroid dependent. Aim for lowest possible dose. Stage 5 – Steroids not helpful. Steroid prophylaxis – Ca, Vit D, bisphosphonate. Need systemic form (inhaled form may help w/ underlying asthma but has no efficacy in ABPA)")
17
Tx - Itraconazole Dec’s antigenic stimulus for bronchial inflammation, possibly by dec;g specific Aspergillus IgG Dec’d metabolism of steroids, so may be able to use lower dosages 16 week course + steroids significant increased likelihood of clinical response (46 vs 19%) 200 TID x 3 days, then 200 BID x 16 wks, +/- Qday x 16 wks Monthly LFTs
 200 TID x 3 days, then 200 BID x 16 wks, +/- Qday x 16 wks. Monthly LFTs.")
18
Resources UpToDate – Allergic bronchopulmonary aspergillosis (Weller, PF) Mason: Murray & Nadel's Textbook of Respiratory Medicine, 4th ed. Allergic Bronchopulmonary Aspergillosis, from MD Consult Chest (135:3) - Argawal. Allergic Bronchopulmonary Aspergillosis. _18/lesson17.php
 - Argawal. Allergic Bronchopulmonary Aspergillosis. _18/lesson17.php.")
Similar presentations
 Infections (pneumonia, airways disease)>")


 Airway.>")










 SHEN JIN The First Affiliated Hospital of Kunming Medical College.>")




