Download presentation
Presentation is loading. Please wait.

1
Remote follow up: Where are we now? Has it improved services to our patients? LYDIA BRADLEY CRM DEVICES LEAD PHYSIOLOGIST

2
Remote monitoring allows wireless & non-wireless remote interrogation of patients devices from the comfort of their own homes. Monitoring systems are designed to provide medical staff with important automated data from implanted cardiac devices without little delay allowing us to respond more rapidly to changes in the patient or device status. Remote monitoring has the potential to reduce total follow-up times in clinic and lower patient transport costs. All systems available use either a standard telephone line or a digital mobile network to transmit the data to a secure server.

3
Before remote monitoring ILR patients seen every 3/12. Now 100% virtual once 6/52 wound check done. ICD/ CRTD/ CRTP seen every 3/12. Now every 6/12 PPM pts every 12/12 with 3/12 towards ERI. Now remote monitoring supplied to eligible patients to save on frequent OPD battery checks.

4
How it works

5
Available data

6
Data can be used to diagnose patients disease status

7
Diagnostic EGM's

8
Available data

9
Systems Currently available

10
Altitude Study Sponsored by Boston Scientific The Altitude study looked at the long term outcome after ICD and CRT implantation and the influence of remote device follow-up Outcomes were compared between patients followed up in device clinic settings and those who regularly transmit remote data collected from the device on an average of four times per month. A total of 194,006 patients were included in the survival analysis. 69,556 patients followed up via remote monitoring and 124,450 were followed up in clinic only.

11
Altitude results Survival at one year was 92% for ICD & 88% for CRTD pts. Patients followed on Latitude had 50% relative reduction in the risk of death compared to patients followed in clinic only. Heart failure patients who transmitted weight & BP data via Latitude experienced an additional 10% reduction in the risk of death compared to other networked CRTD patients followed on Latitude.

12
The Lumos-T Safely Reduces Routine Office Device Follow-up (TRUST) Trial Sponsored by Biotronik TRUST trial tested the hypothesis that remote home monitoring can safely reduce in-office follow-ups, while enabling rapid physician evaluation of significant events. 1339 patients across 102 US sites were randomized to HM or conventional F/U. F/U checks occurred at 3,6,9,12 & 15 months after implantation. Conventional patients were evaluated with office visits only. Scheduled office visits & unscheduled evaluations, incidence of morbidity & time elapsed from first event occurrence in each patient to physician evaluation were tracked for each group.

13
TRUST Results HM reduced total in-hospital device evaluations by 45% without effecting morbidity. In the HM group, 85.8% of all 6, 9, & 12 month follow-ups were performed remotely only, indicating that HM provided sufficient assessment in the majority. Median time to evaluation was <2 days in the the HM group compared with 36 days in the conventional group for all arrhythmic events.

14
The Evolution of Management Strategies of Heart Failure Patients With Implantable Defibrillators ( EVOLVO) Study Supported by Italian Ministry of health, technical support from Medtronic Multicentre randomized trial involving 200 patients compared remote monitoring with standard patient management consisting of scheduled visits and patient response to audible ICD alerts. Study was designed to test the hypothesis that remote monitoring can reduce emergency healthcare use in HF patients compared with standard management consisting of scheduled in-office visits. Patients randomized to remote transmission on or remote transmission off. The primary end point was the rate of emergency department or urgent in-office visits for heart failure, arrhythmias or ICD related events.

15
EVOLVO results Remotely followed HF patients experienced reduced A&E & urgent in office visits by 35% over 18 months when compared to in-office follow- up.

16
New Cross Hospital Carelink express pilot study Clinic's full of patients who may not be suitable for Carelink at home. Designed to assess the feasibility of an "express lane" for device follow-up. Does every patient need to sit in front of a programmer?

17
Carelink express pilot study Objective - The patient only saw the programmer if it was strictly necessary. How - Device interrogation was performed when the patient checked in through Carelink express.

18
Majority of patients arrived to their appointment early Observations from conventional pacemaker clinic

19
95% of appts are for routine device follow-up. - Of these checks; 82% require no programming. - 18% of device checks require reprogramming - 4% of these are first follow-up.

20
Opportunity & Observations Appointments booked every 30 min. Patient in consultation room on average 17 mins. Patients spends on average 40 mins in the dept. Is there opportunity for time gain if clinics more predictable?? Clinic efficiency can sometimes be threatened with problem patients meaning clinic can at times be drawn to a halt until problem solved. Clinics already running daily with device implants growing each year & no more CP resource meaning we are asked to do more with less!

21
Productivity Analysis

22
High level observations Opportunities: Pt waiting time reduction Management of urgent patients / pre-discharge checks Carelink Express in clinic solution - will we save time by not seeing every patient in the clinic room for a full check? Can the benefits and efficiencies seen with remote translate to the "in clinic" setting?

23
Carelink express in clinic Most patients arrive early so can use the Express monitor immediatley. Patient acceptance was good once explained. ATO was available for support.

24
In clinic checks Clinic time reduced due to prior warning of what the patients needs are.

25
Time spent in clinic Some waiting time includes Express transmission time. Improved efficiency from 2 pts/FTE to 3.1pts/FTE.

26
Express European Pilot The pilot-projects were carried out in 2012 - 2013. 8 centres in 5 countries completed the pilot, the assessment of the overall results are based on a total of 485 patients. The pilot demonstrated a significant improvement of all performance indicators in all participating hospitals.

27
European Pilot Results Summary Pt waiting time - From an average of 41 mins to an average of 22 mins. Average reduction of 46%. Consultation duration FU - From an average of 17 mins to an average 10 mins. Average reduction of 41% Efficiency FU process - From average of 1.9 pts/FTE hr to average 3.1 pts / FTE hr. Average improvement of 65%

28
The next stage for Carelink express Currently two express monitors in trust located in A&E & AMU Helping to streamline the experience for the patient and increase the speed of diagnosis in acute medical settings Good response from medical staff Third monitor on its way!

29
Express clinics in OPD Third monitor to be located in atrium of H&L centre. Patients allowed a window of 1 week to attend a express download. H&L pt entrance open 6am - 10pm. Free parking for upto 20 mins. Health questionnairre to be sent with every appointment letter. Low threshold for reviewing patient in clinic.

30
Case study 1 84yr old female Ischaemic heart disease Severe LV systolic impairment Previous MI CRTD implanted 2007 CRTD box change 2013 Non-compliant with F/U

31
Alert transmission received

32
Pt contacted Recent increase in symptoms - SOB Weight gain Reduced exercise capacity Patient called to clinic

33
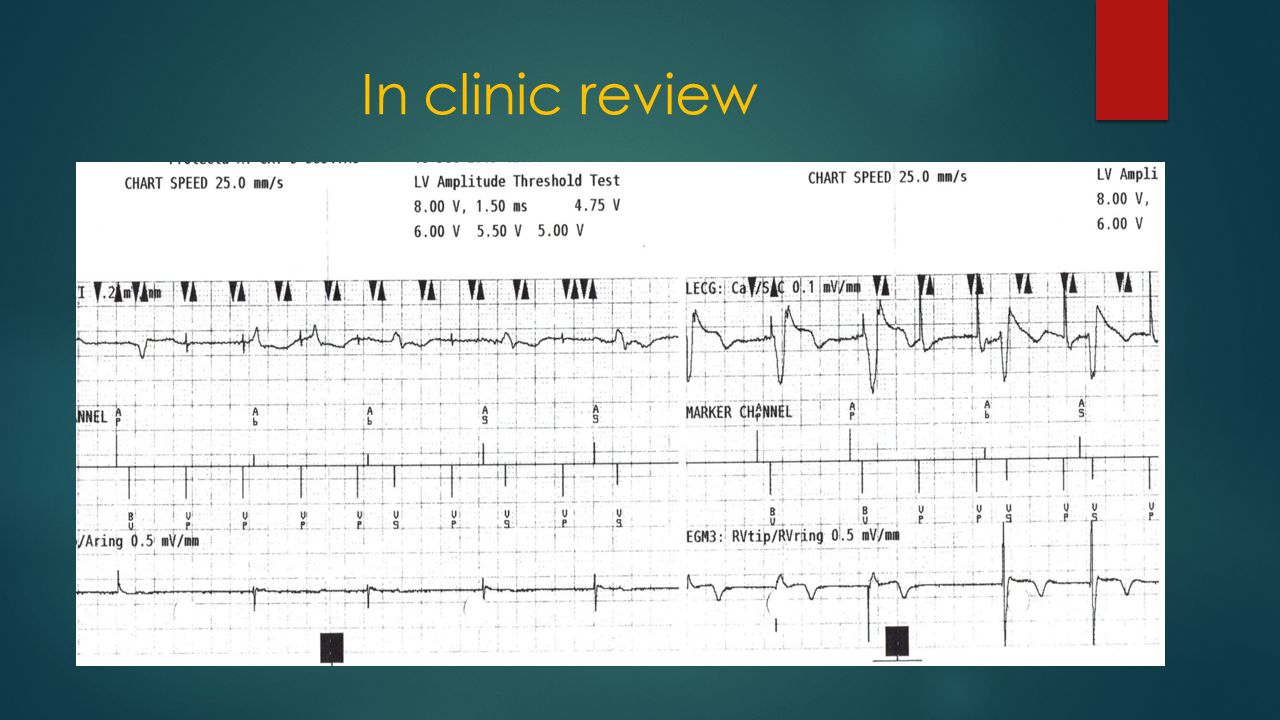
In clinic review

35
Out come LV lead displaced - no capture at 8v Patient & meds reviewed by SpR Patient discharged home Plan to reposition LV lead as OPD

36
Case study 2 70 yr old female Previous MI - 2012 Symptomatic AV block ECG - RBBB, LAD, normal PR interval ECHO - EF 30%, akinesia involving IVS, anterior wall & apex Single coil ICD lead inserted with PPM Upgraded to CRTD

37
In clinic

38
Latitude alert received

39
Information received

41
Patient called to clinic

42
Outcome Therapies turned off Patient admitted to cardiology ward New ICD lead implanted

43
Summary Remote monitoring - Reduces patient travel times and costs Reduces routine follow-up time Reduces number of OPD in clinic appointments without reducing amount of follow- ups Allows increased patient reviews if indicated without impacting on patients life Allows for earlier detection of device malfunction Allows earlier detection of patient disease status, therefore reducing the need for urgent hospital admissions Improves patient QOL and enhances the care that is already provided

44
Thank you Any questions?

Similar presentations

 Trial The Value of Remote Monitoring George H. Crossley, MD.>")

 , or>")













 Trial The Value of Remote Monitoring George H. Crossley, MD.>")


