Download presentation
Presentation is loading. Please wait.

1
Schistosomiasis (Bilharzia) Ass. Prof. Dr
Schistosomiasis (Bilharzia) Ass. Prof. Dr. Wijdan Akram FICMS Community Medicine
 Ass. Prof. Dr. Wijdan Akram FICMS Community Medicine.")
2
Definition: Schistosomiasis, also known as bilharzia, is a disease caused by parasitic worms, more than 200 million people are infected worldwide. In terms of impact this disease is second only to malaria as the most devastating parasitic disease. Schistosomiasis is considered one of the Neglected Tropical Diseases (NTDs)
")
3
The parasites that cause schistosomiasis live in certain types of freshwater snails. The infectious form of the parasite, known as cercariae, emerge from the snail, hence contaminating water. person can become infected when the skin comes in contact with contaminated freshwater. Most human infections are caused by Schistosoma mansoni, S. haematobium, or S. japonicum.

4
Schistosomiasis or bilharzia is a disease affecting many people in developing countries. In the form of 'acute' schistosomiasis it is sometimes referred to as snail fever and cutaneous schistosomiasis.

5
It is a blood fluke( trematode) infection with adult male and female worms living within mesenteric or vesical veins of the host over a life span of many years. Case definition in endemic areas are: For urinary schistosomiasis: visible hematuria or positive reagent strip for hematuria, or with egg of S. heamatobium in urine ( confirmed case),
,")
6
For intestinal schistosomiasis: : non specific abdominal symptoms, blood in stool. Hepato( spleno) megaly ( suspected case), or presence of eggs in stool( confirmed case).
 megaly ( suspected case), or presence of eggs in stool( confirmed case)..")
7
Although it has a low mortality rate, schistosomiasis can be very debilitating.
Bilharzia, or bilharziosis, is named after Theodor Bilharz, who first described the cause of urinary schistosomiasis in 1851.

8
Epidemiology & Risk Factors
Schistosomiasis is an important cause of disease in many parts of the world, most commonly in places with poor sanitation. School-age children who live in these areas are often most at risk because they tend to spend time swimming or bathing in water containing infectious cercariae.

9
live in, or travel to, areas where schistosomiasis is found and are exposed to contaminated freshwater, considered as a risk factor.

10
Areas where human schistosomiasis is found include:
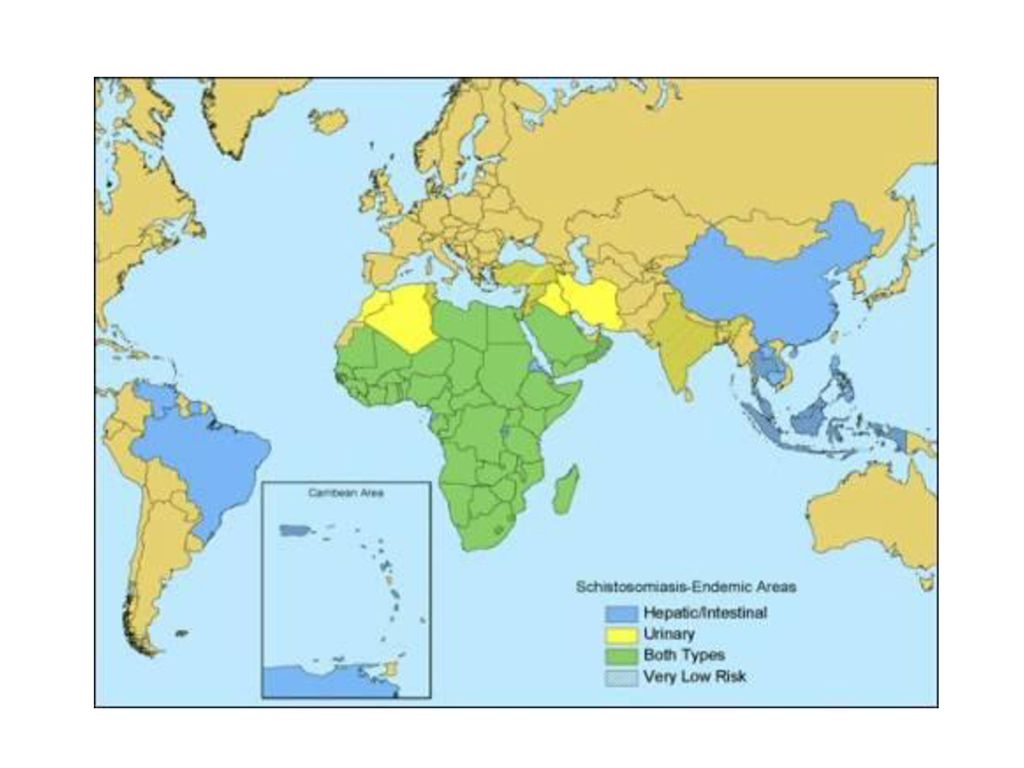
Schistosoma mansoni distributed throughout Africa: There is a risk of infection in freshwater in southern and sub-Saharan Africa–including the great lakes and rivers as well as smaller bodies of water. Transmission also occurs in the Nile River valley in Sudan and Egypt South America: including Brazil, Suriname, Venezuela Caribbean (risk is low): Dominican Republic, Guadeloupe, Martinique, and Saint Lucia.
: Dominican Republic, Guadeloupe, Martinique, and Saint Lucia.")
11
S. haematobium distributed throughout Africa: There is risk of infection in freshwater in southern and sub-Saharan Africa–including the great lakes and rivers as well as smaller bodies of water. Transmission also occurs in the Nile River valley in Egypt and the Mahgreb region of North Africa. found in areas of the Middle East

12
S. japonicum found in Indonesia and parts of China and Southeast Asia S. mekongi found in Cambodia and Laos S. intercalatum found in parts of Central and West Africa.

13
There are five species of flatworms that cause schistosomiasis
There are five species of flatworms that cause schistosomiasis. Each causes different symptoms. Schistosomiasis may travel to different parts of the body, and its localization determines the person's symptoms. Schistosoma mansoni and Schistosoma intercalatum cause intestinal schistosomiasis. Schistosoma haematobium causes urinary schistosomiasis. Schistosoma japonicum and Schistosoma mekongi cause Asian intestinal schistosomiasis.

14
Schistosomiasis map Worldwide 207 million people have the disease with 120 million being symptomatic. Urbanization, pollution, and / or consequent destruction of snail habitat has reduced exposure, with a subsequent decrease in new infections

15
The most common way of getting schistosomiasis in developing countries is by wading or swimming in lakes, ponds and other bodies of water which are infested with the snails (usually of the Biomphalaria Bulinus, or Oncomelania genus) that are the natural reservoirs of the Schistosoma pathogen
 that are the natural reservoirs of the Schistosoma pathogen")
17
Humans are the principle reservoir of S. hematobium,S
Humans are the principle reservoir of S.hematobium,S. intercalatum and S. mansoni although the latter has been reported to rodents. Humans, dogs,cats,pigs,cattle and wild rodenst are potential hosts for S. japonicum. Intermediate hosts: an appropriate snail.

18
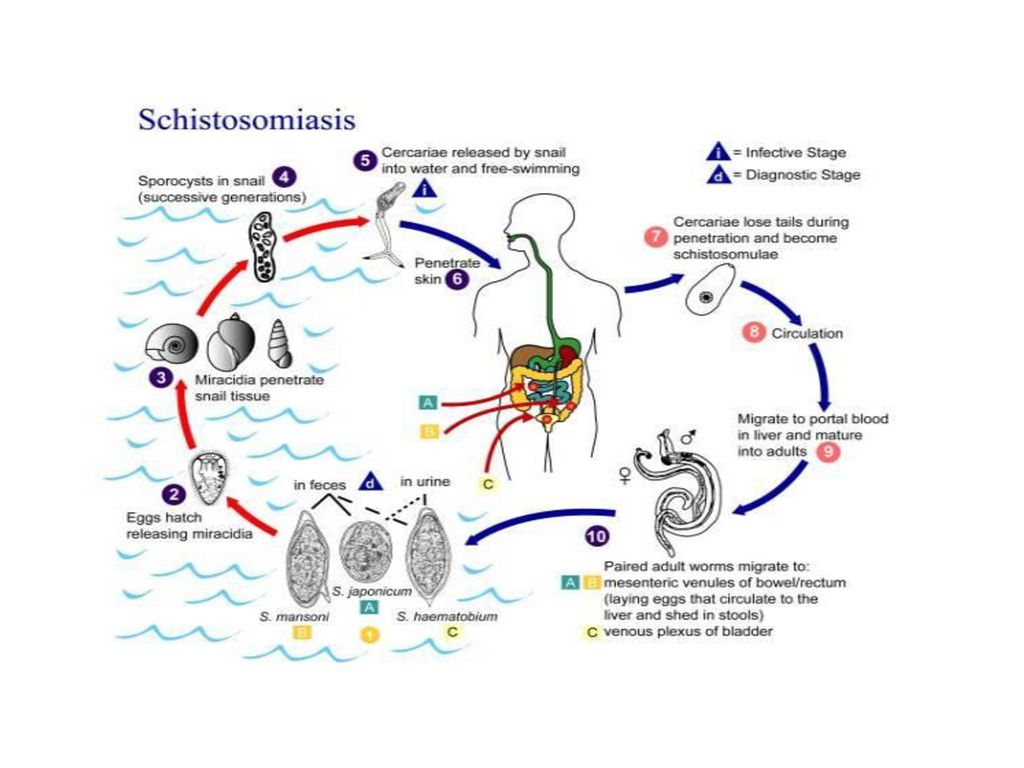
Schistosomiasis life cycle.
Schistosomes have a trematode vertebrate-invertebrate lifecycle (infecting both a vertebrate and invertebrate), with humans being the definitive host
, with humans being the definitive host.")
19
Disease Infection occurs when skin comes in contact with contaminated freshwater in which certain types of snails that carry the parasite are living. Freshwater becomes contaminated by Schistosoma eggs when infected people urinate or defecate in the water. The eggs hatch The eggs hatch on contact with fresh water to release the free-swimming miracidium

20
, and if the appropriate species of snails are present in the water, the parasites infect, develop and multiply inside the snails. The cercariae leaves the snail and enters the water where it can survive for about 48 hours.

21
Cercareae can penetrate the skin of persons (during penetration lose their tail and become schistosomulae) who come in contact with contaminated freshwater, typically when swimming, bathing, or washing. Over several weeks, the parasites migrate through host tissue and develop into adult worms inside the blood vessels of the body.

22
Once mature, the worms mate, and females produce eggs
Once mature, the worms mate, and females produce eggs. Some of these eggs travel to the bladder or intestine and are passed into the urine or stool.

23
Symptoms of schistosomiasis are caused not by the worms themselves but by the body’s reaction to the eggs. Eggs shed by the adult worms that do not pass out of the body can become lodged in the intestine or bladder, causing inflammation or scarring. Children who are repeatedly infected can develop anemia, malnutrition, and learning difficulties. After years of infection, the parasite can also damage the liver, intestine, spleen, lungs, and bladder.

25
Incubation period: acute systemic manifestations may occur in primary infections 2-6 weeks after exposure immediately preceding and during initial egg deposition. Acute systemic manifestations are uncommon, but can occur with S. hematobium infection. Period of communicability:not communicable from person to person. Persons with infection may spread the infection by discharge the eggs in urine and or feces . Susceptibility: is universal, any immunity developing as a result of infection is variable and not fully investigated

26
Pathology Schistosomiasis is a chronic disease.
Pathology of S. mansoni and S. japonicum includes: Katayama fever, hepatic perisinusoidal egg granulomas, portal hypertension, and occasional embolic egg granulomas in the brain or spinal cord.

27
Pathology of S. haematobium includes: hematuria, scarring, calcification, squamous cell carcinoma, and occasional embolic egg granulomas in the brain or spinal cord. Bladder Cancer diagnosis and mortality are generally elevated in affected areas

28
Clinical features Many infections are subclinically symptomatic, with mild anemia and malnutrition being common in endemic areas. Symptoms depend on where the eggs are: Continuing infection may cause granulomatous reactions and fibrosis in the affected organs, which may result in manifestations that include:

29
Colonic polyposis with bloody diarrhea (Schistosoma mansoni mostly);
Portal hypertension with hematemesis and splenomegaly (S. mansoni, S. japonicum; Cystitis and ureteritis (S. haematobium) with hematuria, which can progress to bladder cancer; Pulmonary hypertension (S. mansoni, S. japonicum, more rarely S. haematobium); Glomerulonephritis; and central nervous system lesions.
 with hematuria, which can progress to bladder cancer; Pulmonary hypertension (S. mansoni, S. japonicum, more rarely S. haematobium); Glomerulonephritis; and central nervous system lesions.")
30
Occasionally central nervous system lesions occur: cerebral granulomatous disease may be caused by ectopic S. japonicum eggs in the brain, and granulomatous lesions around ectopic eggs in the spinal cord fromS. mansoni and S. haematobium infections may result in a transverse myelitis with flaccid paraplegia. Katayama Fever Acute schistosomiasis (Katayama's fever) may occur weeks after the initial infection, especially by S.mansoni and S. japonicum.
 may occur weeks after the initial infection, especially by S.mansoni and S. japonicum.")
31
Manifestations include:
Abdominal pain Cough Diarrhea Eosinophilia-extremely high eosinophil granulocyte count. Fever Fatigue Hepatosplenomegaly-the enlargement of both the liver and the spleen.

32
Laboratory diagnosis Microscopic identification of eggs in stool or urine is the most practical method for diagnosis Tissue biopsy (rectal biopsy for all species and biopsy of the bladder for S. haematobium) Antibody detection can be useful in both clinical management (eg, recent infections) and for epidemiologic surveys
 Antibody detection can be useful in both clinical management (eg, recent infections) and for epidemiologic surveys.")
33
Treatment Schistosomiasis is readily treated using a single oral dose of the drug Praziquantel

34
Prevention through good design
The main focus of prevention is eliminating the water-borne snails which are natural reservoirs for the disease This is usually done by identifying bodies of water, such as lakes, ponds, etc., Which are infested, forbidding or warning against swimming and adding niclosamide, acrolein, copper sulfate, etc., to the water in order to kill the snails.

35
Irrigations schemes can be designed to make it hard for the snails to colonize the water, and to reduce the contact with the local population.

Similar presentations

>")










 Doç.Dr.Hrisi BAHAR.>")






