Download presentation
Presentation is loading. Please wait.

1
MANANGEMENT OF ROTATOR CUFF TEARS
DrT.K BYAKIKA Consultant Orthopaedic Surgeon and Adjunct Professor COHES, JKUAT

2
Dawn of an era

3
Introduction Rotator cuff repair has evolved greatly in last 10 years
Improved understanding of the anatomy and pathoanatomy “cover the hole” past thinking Concept of the RTc balancing the force couple about the glenohumeral joint

4
Introduction When faced with a rotator cuff tear the primary goal of surgery is to balance the force couples in both the transverse and coronal planes Suspension bridge analogy This contradicts the historical principle of covering the hole

5
Primary Goals Decrease pain Improve shoulder function
Limit cuff tendinopathy

6
Why? Arthroscopic The “ in thing” Better visualisation
Better diagnosis Access to the glenohumeral joint Subacromial bursa Acromioclavicular joint Better results? DR M Ferguson Centre for Sports medicine

7
Open vs arthroscopic Both give satisfactory outcomes but there are
Disadvantages of open repair: Persistent pain Longer rehabilitation Postoperative stiffness Unrecognized concomitant pathology Deltoid morbidity

8
Mini open Arthroscopic joint inspection Arthroscopic acromioplasty
Deltoid split Outcome equivalent or superior to open repair Baker & Liu, Levy, Paulos, Weber

9
Arthroscopy Patients like it Better visualisation
Better I.D. of tear size, configuration and mobility

10
outcomes SJ Snyder AANA speciality Day AAOS 1999 48 pts
Mean FU 3.5 yrs Minimum 2cm tear Outcomes 90% satisfied with pain relief 93% satisfied with function Improved UCLA ASES scores

11
Transition to arthroscopic repair
Absolute guidelines Be able to do an open repair Do your best operation Mini-open repair – goal for most of us can do acromioplasty under 15 mins > 50 cuff repairs / year NB Judged by outcome in the long run

12
biomechanics Balance force couples Single centre of rotation
Avoid tension mismatch

13
Steep learning curve ACJ reconst Cuff repair ASAD Instability Surgery
Debride Diagnosis DR M Ferguson Centre for Sports medicine

14
Classification Location of tear Partial – I to IV Complete I to IV
A- Articular B- bursal C- complete Partial – I to IV Complete I to IV

15
Tear patterns 4 major types Crescent shaped U-shaped
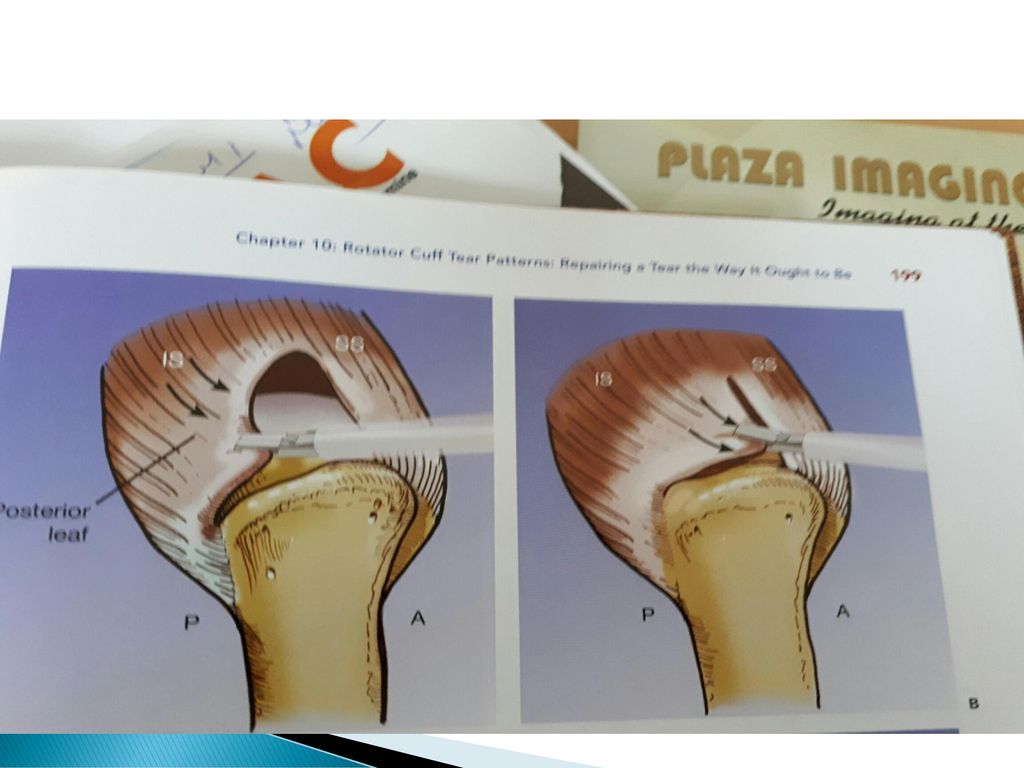
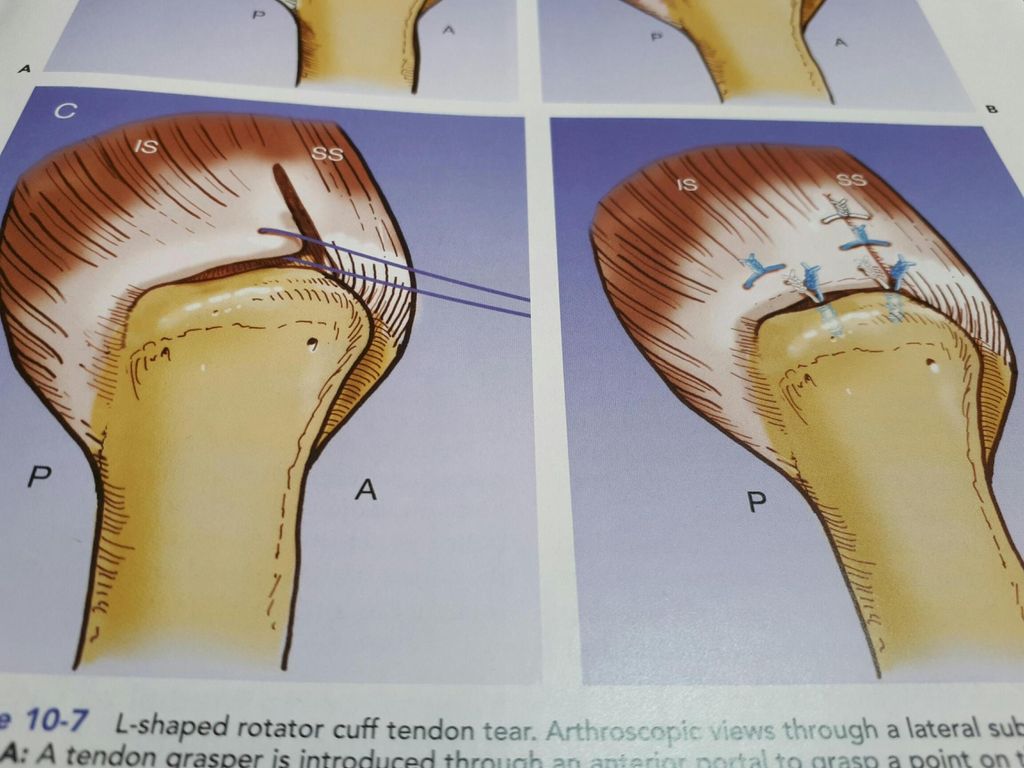
L-shaped & reverse L-shaped Massive contracted immobile tears

18
Double row repair

19
U shaped

20
U shaped

21
Reverse L Shaped

22
Massive adhesed contracted immobile RTC

23
Partial thickness rotator cuff tears
Twice as common as full thickness RTc tears 3 types Articular surface Bursal surface Intrasubstance(interstitial tears) Controversy as to how to measure depth of the tear and which partial thickness tears should be repaired Weber recommends that > 50% tendon thickness should be repaired
 Controversy as to how to measure depth of the tear and which partial thickness tears should be repaired. Weber recommends that > 50% tendon thickness should be repaired.")
24
Operative strategy Beach chair position Or lateral decubituus
Artrhoscopy tower Arthropump Radiofrequency Shavers Operative instruments Cannulae Suture anchors

25
Intraoperative approach
Usually 3 portals, posterior, lateral and anterior glenohumeral joint arthroscopic inspection, LHB, SSC tendon, assess the rotator cuff, intra-articular tears, Osteoarthritis Sub acromial space Bursectomy, Determine type of tear Acromioplasty(+/-) Cuff mobilisation(critical, coracohumeral lig, coracoid
 Cuff mobilisation(critical, coracohumeral lig, coracoid.")
26
Surgical procedure ctd
Repair site preparation Mobility of the cuff Anchor placement Knotted or knotless Single or double row repair/ pros and cons Deadmans angle

27
Results 2014-2017 NO Average age Range Male 17 54 40-81 female 21 51
40-79 total 38 52.3

28
Operative time Year Average 2014 2.5hrs 2015 2hrs 2016 1.5hrs

29
Cases per year YEAR CASES 2014 7 2015 9 2016 11 2017

30
Tear patterns Cresecent 30 U shaped 2 Lshaped Reverse L Massive Total
38

31
Discussion Rotator cuff tears occur in the middle age and above as evidenced by our results which is in keeping with worldwide data Arthroscopic rotator cuff surgery affords you the opportunity to classify the tears The crescent tears are the commonest type of tears Using operative time as a measure of skill,less intraoperative time shows skills improving The instrumentation and also the use of knotless anchors has siginficantly influenced the ease with which perform surgery

32
Conclusions Arthroscopic rotator cuff surgery is doable and affords superior diagnostic capability of tears In my experience has a relatively long and steep learning curve Suggest that those interested should follow the algorithm as advised There are many patients with cuff problems as evidenced by rising numbers in my practice, “word of mouth” Predictable good outcomes

33
Thank you for your attention

Similar presentations