Download presentation
Presentation is loading. Please wait.

1
Arterial Blood Gas Interpretation Dr. Shinjan Patra

2
OBJECTIVES ABG Sampling Interpretation of ABG Step wise approach to decode an ABG Acid Base status Electrolyte status

3
ABG – Procedure and Precautions Site-Ideally Radial Artery Brachial Artery Femoral Artery. Ideally - Pre-heparinised ABG syringes - Syringe should be FLUSHED with 0.5ml of 1:1000 Heparin solution and emptied.

4
Precautions DO NOT LEAVE EXCESSIVE HEPARIN IN THE SYRINGE HEPARIN DILUTIONAL HCO 3 EFFECT PCO 2 Only small 0.5ml Heparin for flushing and discard it Syringes must have > 50% blood. Use only 2ml or less syringe.

5
Precautions Ensure No Air Bubbles Contact with air bubbles- PO2 Pco2 ABG Syringe must be transported at the earliest to the laboratory for EARLY analysis via COLD CHAIN

6
Other Considerations – Any change in body temp at the time of sampling leads to alteration in values detected by the electrodes – ABG Analyser is controlled for Normal Body temperatures – ABG Sample should always be sent with relevant information regarding O 2, FiO 2 status and Temp.

7
Step Wise approach to Interpret the ABG At first we will go through the normal values-

8
ANALYTENormal ValueUnits pH7.35 - 7.45 PCO235 - 45mm Hg PO272 – 104mm Hg` [HCO3]22 – 30meq/L SaO295-100% Anion Gap12 + 4meq/L ∆HCO3+2 to -2meq/L
![ANALYTENormal ValueUnits pH PCO mm Hg PO272 – 104mm Hg` [HCO3]22 – 30meq/L SaO % Anion Gap12 + 4meq/L ∆HCO3+2 to -2meq/L](http://images.slideplayer.com/48/11783862/slides/slide_8.jpg "ANALYTENormal ValueUnits pH PCO mm Hg PO272 – 104mm Hg` [HCO3]22 – 30meq/L SaO % Anion Gap12 + 4meq/L ∆HCO3+2 to -2meq/L")
9
Steps Step 1- Is the ABG authentic? Step 2- Acidosis Or Alkalosis Step 3- Respiratory or Metabolic Step 4- If respiratory is it acute or chronic? Step 5- Is there any compensation or not? Step 6- Is the compensation adequate? Step 7- Anion-Gap calculations & implications

10
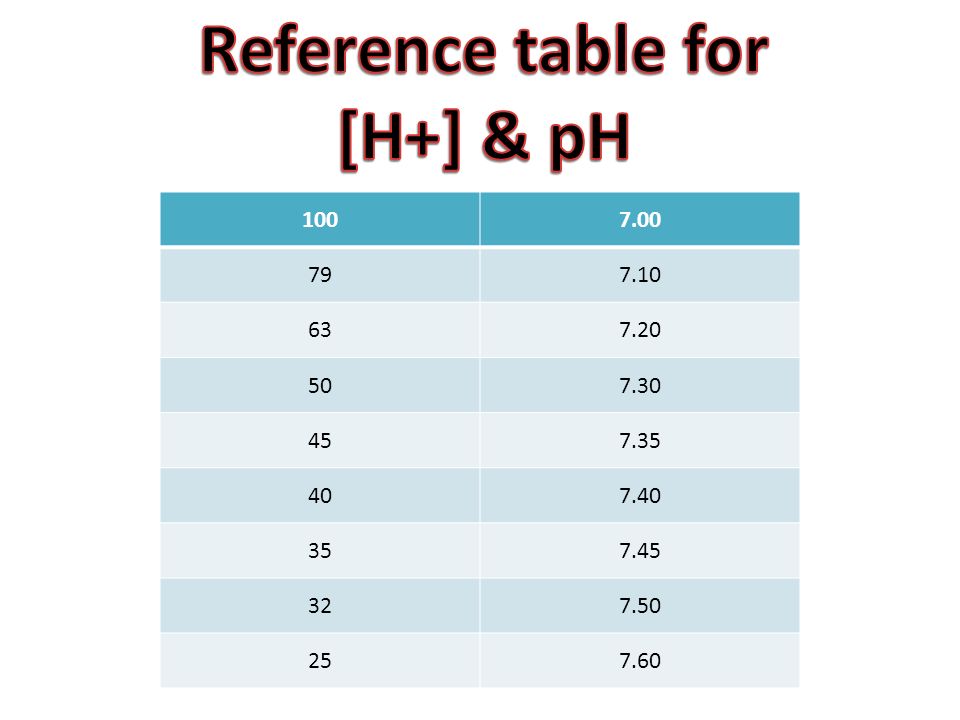
Is the ABG authentic? [ H+] neq/l = 24 X (PCO 2 / HCO 3 ) If this equation fulfills then it is authentic This equation derives from- Henderson-Hasselbalch equation pH = 6.1 + log HCO 3 - 0.03 x PCO 2
 If this equation fulfills then it is authentic This equation derives from- Henderson-Hasselbalch equation pH = log HCO x PCO 2.")
11
1007.00 797.10 637.20 507.30 457.35 407.40 357.45 327.50 257.60
12
Acidosis Or Alkalosis Look at pH <7.35 - acidemia >7.45 – alkalemia

13
Respiratory or Metabolic IS PRIMARY DISTURBANCE RESPIRATORY OR METABOLIC? pH PCO 2 or pH PCO 2 -METABOLIC pH PCO 2 or pH PCO 2 - RESPIRATORY There may be mixed acidosis or alkalosis also.

14
If respiratory is it acute or chronic? We will determine it by evaluating the value of x from this equation- ppH= x x ∆Pco 2 /10 If this value of x is close to 0.08 then it is acute If this value of x is close to 0.03 then it is chronic

15
Is there any compensation or not? If respiratory acidosis or alkalosis-then [HCO3] increased or decreased respectively. If metabolic acidosis or alkalosis- then Pco2 decreased or increased respectively.

16
Is the compensation adequate? Respiratory compensation(in underlying metabolic disorder) Pco2 will decrease by 1.25 mm Hg per mmol/l decrease in [HCO3](metabolic acidosis) Pco2 will increase by 0.75 mm Hg per mmol/l increase in [HCO3](metabolic alkalosis)
 Pco2 will decrease by 1.25 mm Hg per mmol/l decrease in [HCO3](metabolic acidosis) Pco2 will increase by 0.75 mm Hg per mmol/l increase in [HCO3](metabolic alkalosis).")
17
Metabolic Compensation(in underlying Respiratory disorder) -For every 10mm Hg change in Pco2 [Hco3] will increase 1meq/l(acute resp. acidosis) [Hco3] will increase 4meq/l(chr. resp. acidosis) [Hco3] will decrease 2meq/l(acute resp. alkalosis [Hco3] will decrease 5meq/l(chr. resp. alkalosis)
![Metabolic Compensation(in underlying Respiratory disorder) -For every 10mm Hg change in Pco2 [Hco3] will increase 1meq/l(acute resp.](http://images.slideplayer.com/48/11783862/slides/slide_17.jpg "acidosis) [Hco3] will increase 4meq/l(chr. resp. acidosis) [Hco3] will decrease 2meq/l(acute resp. alkalosis [Hco3] will decrease 5meq/l(chr. resp. alkalosis).")
18
Anion-Gap Calculations AG= [Na+] – {[Cl-]+[HCO3-]} Normal Value= 10-12 meq/l It mostly includes the unmeasured anions such as- Albumin, phosphates, sulfate & organic anions.
![Anion-Gap Calculations AG= [Na+] – {[Cl-]+[HCO3-]} Normal Value= meq/l It mostly includes the unmeasured anions such as- Albumin, phosphates, sulfate & organic anions.](http://images.slideplayer.com/48/11783862/slides/slide_18.jpg "Anion-Gap Calculations AG= [Na+] – {[Cl-]+[HCO3-]} Normal Value= meq/l It mostly includes the unmeasured anions such as- Albumin, phosphates, sulfate & organic anions.")
19
AG variation in Acidosis High anion gap acidosis- Lactic acidosis, Ketoacidosis, Toxins ingestion, Renal failure(acute & chronic) Normal anion gap acidosis- GI bicarbonate loss(diarrhea, external pancreatic drainage), Renal acidosis(RTA)
 Normal anion gap acidosis- GI bicarbonate loss(diarrhea, external pancreatic drainage), Renal acidosis(RTA)")
20
Relationship Between ∆AG & ∆[Hco3] If there is increased AG present then we should see the ∆AG/ ∆[Hco3] value to assess the cause. If it is <1= Concurrent non-anion gap metabolic acidosis also present. If it is 1-2= Uncomplicated anion-gap metabolic acidosis present If it is >2= Associated Metabolic Alkalosis also present
![Relationship Between ∆AG & ∆[Hco3] If there is increased AG present then we should see the ∆AG/ ∆[Hco3] value to assess the cause.](http://images.slideplayer.com/48/11783862/slides/slide_20.jpg "If it is <1= Concurrent non-anion gap metabolic acidosis also present. If it is 1-2= Uncomplicated anion-gap metabolic acidosis present If it is >2= Associated Metabolic Alkalosis also present.")
21
Case scenarios & interpretation

Similar presentations



 Blood Gas Analysis Dr. Prakash Mohanasundaram Department of Emergency & Critical Care medicine Vinayaka Missions University.>")








. He developed sever.>")






![Acid-Base balance Prof. Jan Hanacek. pH and Hydrogen ion concentration pH [H+] nanomol/l 6.0 1000 7.0 100 8.0 10 9.0 1.](/21/6241563/big_thumb.jpg "Acid-Base balance Prof. Jan Hanacek. pH and Hydrogen ion concentration pH [H+] nanomol/l 6.0 1000 7.0 100 8.0 10 9.0 1.>")
