Download presentation
Presentation is loading. Please wait.

1
Fluids, electrolytes and acid-base balance

2
Body Fluids - distribution

3
(1)Intracellular fluid : (1)Intracellular fluid : 40% of body mass(~2/3 of total water) 40% of body mass(~2/3 of total water) (2)Extracellular fluid : (2)Extracellular fluid : 20%body mass (~1/3 total water) 20%body mass (~1/3 total water)
Intracellular fluid : (1)Intracellular fluid : 40% of body mass(~2/3 of total water) 40% of body mass(~2/3 of total water) (2)Extracellular fluid : (2)Extracellular fluid : 20%body mass (~1/3 total water) 20%body mass (~1/3 total water)")
4
Body Fluids - distribution Extracellular fluid: Extracellular fluid: 1) plasma (20%) : 5% of body weight 1) plasma (20%) : 5% of body weight 2) interstitial fluid (80%) :15% of body weihgt 2) interstitial fluid (80%) :15% of body weihgt
 plasma (20%) : 5% of body weight 1) plasma (20%) : 5% of body weight 2) interstitial fluid (80%) :15% of body weihgt 2) interstitial fluid (80%) :15% of body weihgt")
5
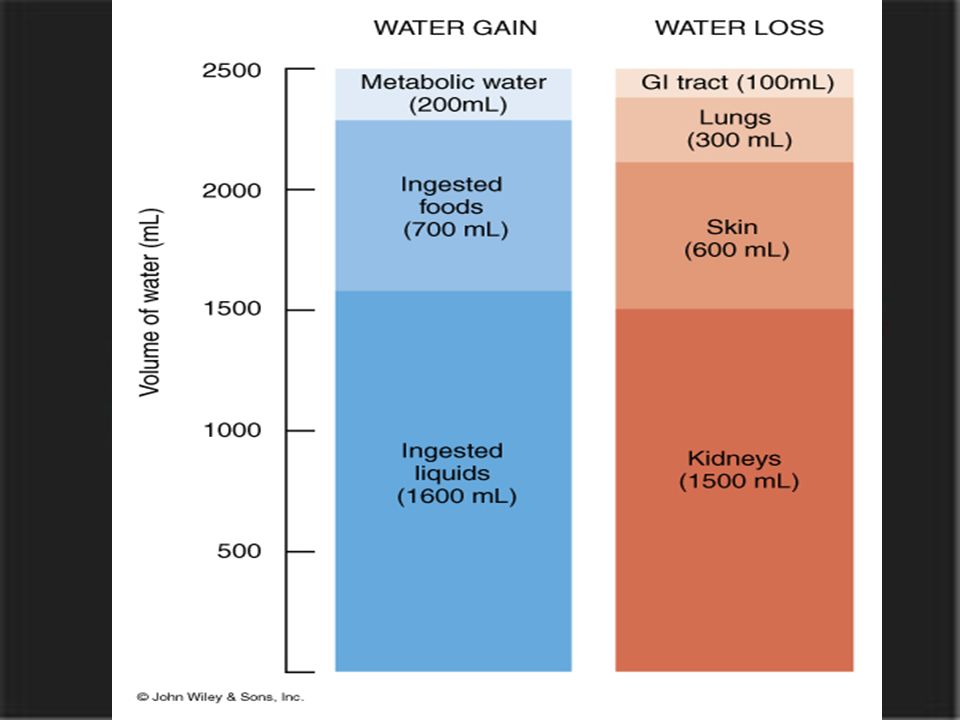
Normally body fluid volume remains constant Normally body fluid volume remains constant Fluid loss = fluid gain Fluid loss = fluid gain fluid gain: fluid gain: ~60% ingested liquids ~60% ingested liquids ~30% ingested in foods ~30% ingested in foods ~10% metabolic water (from oxidation) ~10% metabolic water (from oxidation)
 ~10% metabolic water (from oxidation)")
6
fluid loss: fluid loss: ~4% faeces ~4% faeces ~28% insensible water loss (skin & lungs) ~28% insensible water loss (skin & lungs) ~8% perspiration ~8% perspiration ~60% urine ~60% urine
 ~28% insensible water loss (skin & lungs) ~8% perspiration ~8% perspiration ~60% urine ~60% urine")
8
Water Intake and Output Figure 26.4

9
Fluid Exchanges Figure 27.3

10
Control of Fluid Balance Hypothalamus Hypothalamus Osmoreceptors Osmoreceptors ADH ( antidiuretic hormone) ADH ( antidiuretic hormone) Hormone (pituitary gland ) Hormone (pituitary gland ) Aldosterone Aldosterone Hormone Hormone
 ADH ( antidiuretic hormone) Hormone (pituitary gland ) Hormone (pituitary gland ) Aldosterone Aldosterone Hormone Hormone")
11
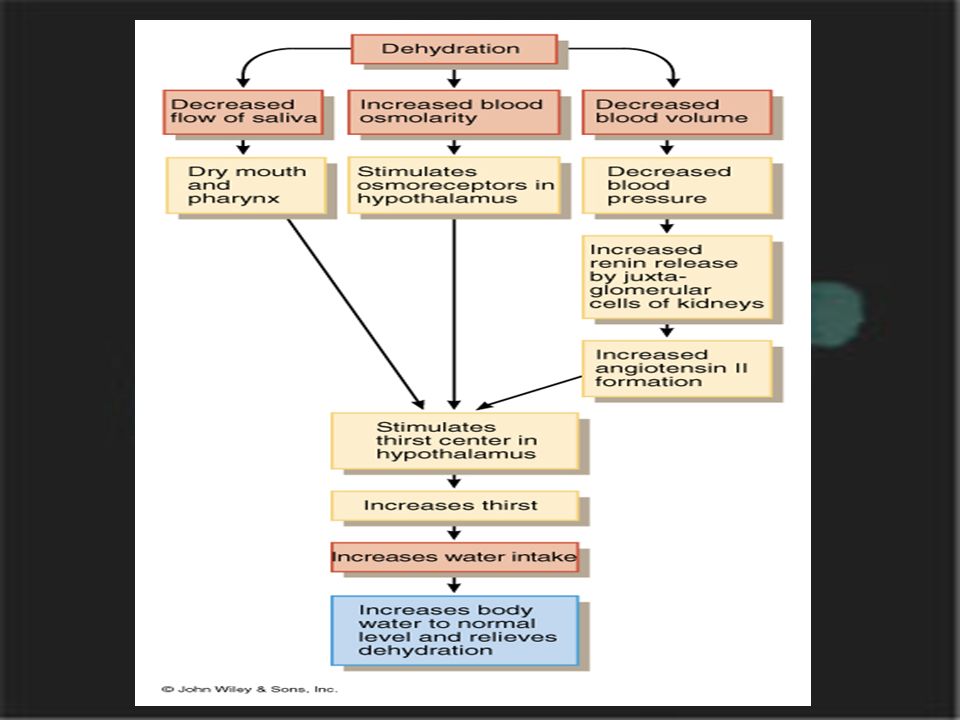
Regulation of body fluid gain and loss Thirst centre in hypothalamus governs urge to drink Thirst centre in hypothalamus governs urge to drink

13
the role of the renin-angiotensin system in regulating thirst

14
Electrolytes Sodium Sodium Potassium Potassium Chloride Chloride Phosphate Phosphate Magnesium Calcium Bicarbonate

15
Electrolytes are important for:. Maintaining fluid balance. Contributing to acid-base regulation. Facilitating enzyme reactions. Transmitting neuromuscular reactions

16
Extracellular : Extracellular : Sodium is the chief cation Sodium is the chief cation Chloride is the major anion Chloride is the major anion Intracellular : Intracellular : Potassium is the chief cation Potassium is the chief cation Phosphate is the chief anion Phosphate is the chief anion

17
Distribution of Solutes

18
Cations and Anions Figure 27.2

19
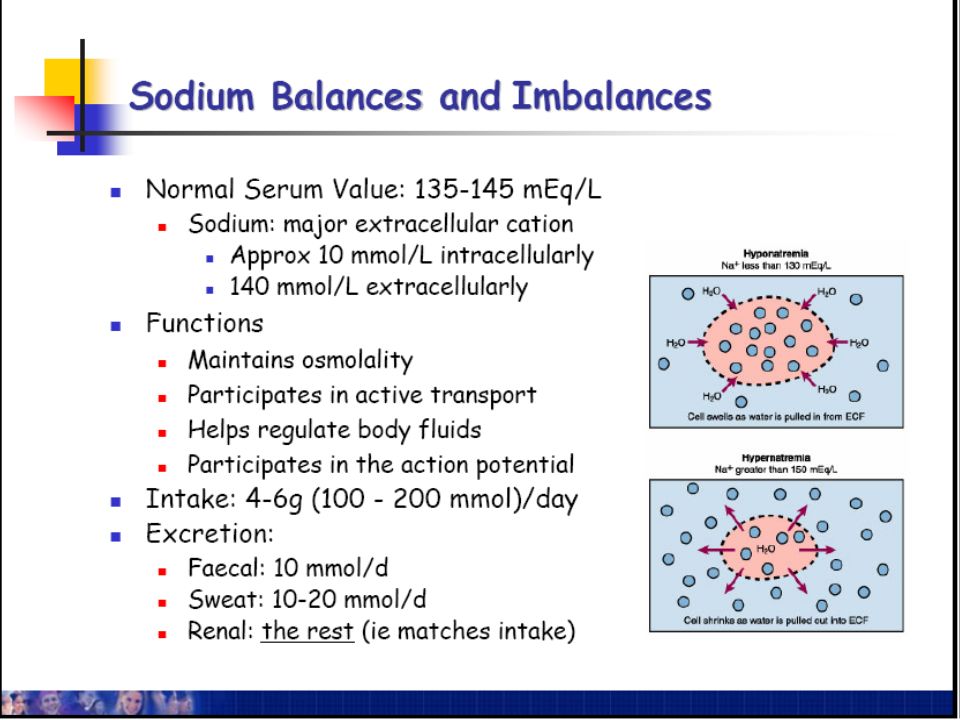
Electrolytes Sodium (Na + ) : 135-145 mmol/liter Sodium (Na + ) : 135-145 mmol/liter Most abundant cation Most abundant cation major ECF cation (90% of cations present) major ECF cation (90% of cations present) determines osmolarity of ECF determines osmolarity of ECF Homeostatic imbalances : Homeostatic imbalances : Hyponatremia - muscle weakness, coma Hyponatremia - muscle weakness, coma Hypernatremia - coma Hypernatremia - coma
 : mmol/liter Sodium (Na + ) : mmol/liter Most abundant cation Most abundant cation major ECF cation (90% of cations present) major ECF cation (90% of cations present) determines osmolarity of ECF determines osmolarity of ECF Homeostatic imbalances : Homeostatic imbalances : Hyponatremia - muscle weakness, coma Hyponatremia - muscle weakness, coma Hypernatremia - coma Hypernatremia - coma")
21
Regulation of sodium balance Na + balance regulated by kidneys Na + balance regulated by kidneys angiotensin II increases Na + absorption angiotensin II increases Na + absorption aldosterone increases Na + absorption in collecting ducts aldosterone increases Na + absorption in collecting ducts

22
Fluid Deficit--Dehydration Insufficient body fluid resulting either from inadequate intake or excessive loss Insufficient body fluid resulting either from inadequate intake or excessive loss Hypertonic(Hypernatremia) Hypertonic(Hypernatremia) Hypotonic (Hyponatremia) Hypotonic (Hyponatremia) Isotonic Isotonic
 Hypertonic(Hypernatremia) Hypotonic (Hyponatremia) Hypotonic (Hyponatremia) Isotonic Isotonic")
23
Disorders of Water and sodium Balance : hyperosmotic dehydration ( Hypernatremia) Sodium (Na + ) >150 mmol/L, osmolarity >310 Sodium (Na + ) >150 mmol/L, osmolarity >310 Water loss exceeds water intake and the body is in negative fluid balance Water loss exceeds water intake and the body is in negative fluid balance
 Sodium (Na + ) >150 mmol/L, osmolarity >310 Sodium (Na + ) >150 mmol/L, osmolarity >310 Water loss exceeds water intake and the body is in negative fluid balance Water loss exceeds water intake and the body is in negative fluid balance")
24
Causes include: hemorrhage, severe burns, prolonged vomiting or diarrhea, profuse sweating, water deprivation, and diuretic abuse Causes include: hemorrhage, severe burns, prolonged vomiting or diarrhea, profuse sweating, water deprivation, and diuretic abuse Diagnosis :blood test for Sodium (Na + ) : >150 mmol/L Diagnosis :blood test for Sodium (Na + ) : >150 mmol/L Madical management : plain water or Hypotonic IV Madical management : plain water or Hypotonic IV
 : >150 mmol/L Diagnosis :blood test for Sodium (Na + ) : >150 mmol/L Madical management : plain water or Hypotonic IV Madical management : plain water or Hypotonic IV")
25
Signs and symptoms: cottonmouth, thirst, dry flushed skin, and oliguria Signs and symptoms: cottonmouth, thirst, dry flushed skin, and oliguria Prolonged dehydration may lead to weight loss, fever, and mental confusion Prolonged dehydration may lead to weight loss, fever, and mental confusion Other consequences include hypovolemic shock and loss of electrolytes Other consequences include hypovolemic shock and loss of electrolytes

26
Figure 26.7a Disorders of Water Balance: Dehydration Excessive loss of H 2 O from ECF 1 2 3 ECF osmotic pressure rises Cells lose H 2 O to ECF by osmosis; cells shrink (a) Mechanism of dehydration
 Mechanism of dehydration")
27
Renal insufficiency or an extraordinary amount of water ingested quickly can lead to cellular overhydration, or water intoxication Renal insufficiency or an extraordinary amount of water ingested quickly can lead to cellular overhydration, or water intoxication ECF is diluted – sodium content is normal but excess water is present ECF is diluted – sodium content is normal but excess water is present Plasma osmolarity : less than 280 mOsm Plasma osmolarity : less than 280 mOsm Disorders of Water Balance: Hypotonic Dehydration ( Hyponatremia)
")
28
Causes include: Diaphoresis, excessive intake plain water, profuse diuresis,GI loss Causes include: Diaphoresis, excessive intake plain water, profuse diuresis,GI loss Clinical symptoms :Mental confusion, muscle weakness,restless, elevated temp Clinical symptoms :Mental confusion, muscle weakness,restless, elevated temp Diagnosis : blood test for Sodium (Na + ) : <120 mmol/L Diagnosis : blood test for Sodium (Na + ) : <120 mmol/L Medical management : increase sodium PO or IV Medical management : increase sodium PO or IV
 : <120 mmol/L Diagnosis : blood test for Sodium (Na + ) : <120 mmol/L Medical management : increase sodium PO or IV Medical management : increase sodium PO or IV")
29
Figure 26.7b Disorders of Water Balance: Hypotonic Dehydration Excessive H 2 O enters the ECF 1 2 ECF osmotic pressure falls 3 H 2 O moves into cells by osmosis; cells swell (b) Mechanism of hypotonic hydration
 Mechanism of hypotonic hydration")
30
Disorders of Water Balance: isotonic dehydration Call it acute dehydration, lost water and sodium equally, blood serum Sodium (Na + ) and osmolarity of ECF are normal Call it acute dehydration, lost water and sodium equally, blood serum Sodium (Na + ) and osmolarity of ECF are normal Causes include GI loss, infection, intestinal obstruction, skin burning(empyrosis ) Causes include GI loss, infection, intestinal obstruction, skin burning(empyrosis )
 and osmolarity of ECF are normal Call it acute dehydration, lost water and sodium equally, blood serum Sodium (Na + ) and osmolarity of ECF are normal Causes include GI loss, infection, intestinal obstruction, skin burning(empyrosis ) Causes include GI loss, infection, intestinal obstruction, skin burning(empyrosis )")
31
Clinical symptoms : oliguria, loss of appetite,nausea, debilitation,shock Clinical symptoms : oliguria, loss of appetite,nausea, debilitation,shock Diagnosis : depend on clinical history Diagnosis : depend on clinical history Treatment : isotonic saline solution or balanced salt solution(BSS) injection 3000ml/6okg Treatment : isotonic saline solution or balanced salt solution(BSS) injection 3000ml/6okg
 injection 3000ml/6okg Treatment : isotonic saline solution or balanced salt solution(BSS) injection 3000ml/6okg")
32
Water and Sodium 3 NS contains 154 mmol of sodium ions per litre. 500ml will satisfy the daily need of a uncomplicated patient. 3 NS contains 154 mmol of sodium ions per litre. 500ml will satisfy the daily need of a uncomplicated patient. 4 5% Glucose 2-2.5 litres will provide the additional water requirement.

33
Samples of daily Prescription for 24 hours.(each bag to be given over 4 hours)--- 1 Samples of daily Prescription for 24 hours.(each bag to be given over 4 hours)--- 1 500ml 0.9% sodium chloride +20mmol kcl 500ml 0.9% sodium chloride +20mmol kcl 500ml 5% dextrose 500ml 5% dextrose 500ml 5% dextrose+20mmol kcl 500ml 5% dextrose+20mmol kcl 500ml 5% dextrose 500ml 5% dextrose
--- 1 Samples of daily Prescription for 24 hours.(each bag to be given over 4 hours) ml 0.9% sodium chloride +20mmol kcl 500ml 0.9% sodium chloride +20mmol kcl 500ml 5% dextrose 500ml 5% dextrose 500ml 5% dextrose+20mmol kcl 500ml 5% dextrose+20mmol kcl 500ml 5% dextrose 500ml 5% dextrose")
34
Regulation of potassium balance Potassium Potassium Most abundant cation(98% of the K + ) in intracellular fluid Most abundant cation(98% of the K + ) in intracellular fluid balance regulated by changing amount secreted by kidney tubules balance regulated by changing amount secreted by kidney tubules When plasma K + high aldosterone secreted and stimulates principal cells of collecting ducts to secrete K + into filtrate When plasma K + high aldosterone secreted and stimulates principal cells of collecting ducts to secrete K + into filtrate
 in intracellular fluid Most abundant cation(98% of the K + ) in intracellular fluid balance regulated by changing amount secreted by kidney tubules balance regulated by changing amount secreted by kidney tubules When plasma K + high aldosterone secreted and stimulates principal cells of collecting ducts to secrete K + into filtrate When plasma K + high aldosterone secreted and stimulates principal cells of collecting ducts to secrete K + into filtrate")
35
70% of the K + are in the muscle, 10% are in the skin and subcutaneous tissue,others are in the internal organs 70% of the K + are in the muscle, 10% are in the skin and subcutaneous tissue,others are in the internal organs come from daily food come from daily food maily eliminated by kidny(90%) maily eliminated by kidny(90%) Important: Important: Nerve conduction and muscle contraction Nerve conduction and muscle contraction Regulates ICF vol and metabolic processes Regulates ICF vol and metabolic processes
 maily eliminated by kidny(90%) Important: Important: Nerve conduction and muscle contraction Nerve conduction and muscle contraction Regulates ICF vol and metabolic processes Regulates ICF vol and metabolic processes")
36
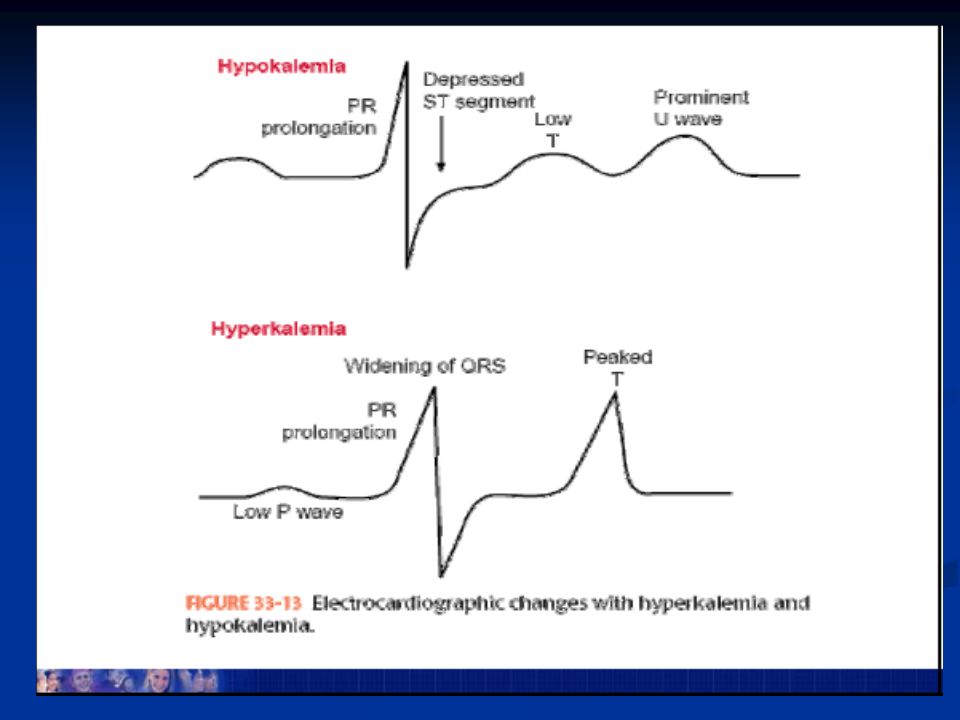
POTASSIUM IMBALANCES POTASSIUM IMBALANCES 3.5-5.5 mmol/L normal value 3.5-5.5 mmol/L normal value HYPOKALEMIA < 3.5 mmol/L HYPOKALEMIA < 3.5 mmol/L

37
Causes of Hypokalemia Long time fasting, loss of appetite (anorexy ) Long time fasting, loss of appetite (anorexy ) Excessive losses from body (diarrhea) Excessive losses from body (diarrhea) Diuretics Diuretics Excessive aldosterone or glucocorticoids Excessive aldosterone or glucocorticoids Low dietary intake Low dietary intake Treatment of diabetic ketoacidosis with insulin Treatment of diabetic ketoacidosis with insulin
 Long time fasting, loss of appetite (anorexy ) Excessive losses from body (diarrhea) Excessive losses from body (diarrhea) Diuretics Diuretics Excessive aldosterone or glucocorticoids Excessive aldosterone or glucocorticoids Low dietary intake Low dietary intake Treatment of diabetic ketoacidosis with insulin Treatment of diabetic ketoacidosis with insulin")
38
Effects of Hypokalemia Cardiac dysrhythmias Cardiac dysrhythmias Interferes with neuromuscular (debilitation ) Interferes with neuromuscular (debilitation ) Paresthesias Paresthesias Low digestive tract motility Low digestive tract motility Weak respiratory muscles Weak respiratory muscles Impaired renal function Impaired renal function
 Interferes with neuromuscular (debilitation ) Paresthesias Paresthesias Low digestive tract motility Low digestive tract motility Weak respiratory muscles Weak respiratory muscles Impaired renal function Impaired renal function")
39
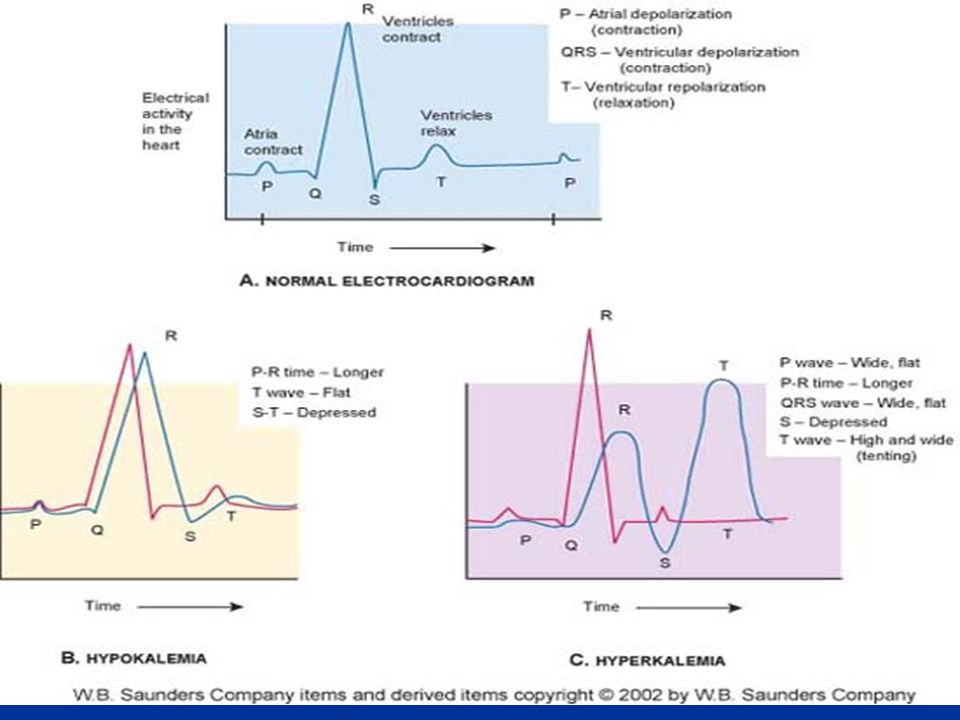
Cardiac Dysrhythmias

40
Medical management- increase oral K, IV Potassium Medical management- increase oral K, IV Potassium IV Potassium : IV Potassium : 0.9% sodium chloride 500ml + 10% kcl 15mmol 0.9% sodium chloride 500ml + 10% kcl 15mmol < 40mmol/L < 40mmol/L Condition : urine 30~40ml/h Condition : urine 30~40ml/h

41
HYPERKALEMIA > 5.5 mmol/L HYPERKALEMIA > 5.5 mmol/L Severe renal failure, burns, potassium-sparing diuretics, K supplements Severe renal failure, burns, potassium-sparing diuretics, K supplements Diarrhea, nausea, muscle weakness, cardiac dysrhythmias Diarrhea, nausea, muscle weakness, cardiac dysrhythmias Medical management- decrease K, dialysis Medical management- decrease K, dialysis

42
Causes of Hyperkalemia Renal failure Renal failure Aldosterone deficit Aldosterone deficit Use of “ K + sparing ” diuretics Use of “ K + sparing ” diuretics Leakage of K + from ICF to ECF Leakage of K + from ICF to ECF Displacement of K + from cells(injury of the tissue) Displacement of K + from cells(injury of the tissue) Prolonged severe acidosis Prolonged severe acidosis
 Displacement of K + from cells(injury of the tissue) Prolonged severe acidosis Prolonged severe acidosis")
43
Effects of Hyperkalemia Cardiac dysrhythmias Cardiac dysrhythmias Muscle weakness Muscle weakness Fatigue, nausea, paresthesias Fatigue, nausea, paresthesias cardiac arrhythmia,slow heartbeat, cardiac arrest cardiac arrhythmia,slow heartbeat, cardiac arrest

46
Medical management- decrease K, dialysis Medical management- decrease K, dialysis 1 ) stop intaking KCI 1 ) stop intaking KCI 2)actively prevent from cardiac arrhythmia 2)actively prevent from cardiac arrhythmia 3)Control the the primary disease 3)Control the the primary disease 4)reduce serum K + 4)reduce serum K +
 stop intaking KCI 1 ) stop intaking KCI 2)actively prevent from cardiac arrhythmia 2)actively prevent from cardiac arrhythmia 3)Control the the primary disease 3)Control the the primary disease 4)reduce serum K + 4)reduce serum K +")
47
Medication : Medication : 1)5%Sodium Bicarbonate (NaHCO 3 )50~100ml 1)5%Sodium Bicarbonate (NaHCO 3 )50~100ml 2)25% dextrose 250ml +insuline20u 2)25% dextrose 250ml +insuline20u 3) 10%Calcium Gluconate 10ml + 25% dextrose + insuline30u + 11.2 % Sodium Lactate Solution 50ml ( in 24 hours 6 drops/minute) 3) 10%Calcium Gluconate 10ml + 25% dextrose + insuline30u + 11.2 % Sodium Lactate Solution 50ml ( in 24 hours 6 drops/minute) Dialysis Dialysis
5%Sodium Bicarbonate (NaHCO 3 )50~100ml 1)5%Sodium Bicarbonate (NaHCO 3 )50~100ml 2)25% dextrose 250ml +insuline20u 2)25% dextrose 250ml +insuline20u 3) 10%Calcium Gluconate 10ml + 25% dextrose + insuline30u + 11.2 % Sodium Lactate Solution 50ml ( in 24 hours 6 drops/minute) 3) 10%Calcium Gluconate 10ml + 25% dextrose + insuline30u + 11.2 % Sodium Lactate Solution 50ml ( in 24 hours 6 drops/minute) Dialysis Dialysis")
48
Review of Calcium Ion Excreted in urine and feces Excreted in urine and feces Balance controlled by: Balance controlled by: PTH PTH Calcitonin Calcitonin Influenced by vitamin D and phosphate levels Influenced by vitamin D and phosphate levels Important functions: Important functions: Structural strength essential for bones and teeth Structural strength essential for bones and teeth Maintains stability of nerve membranes Maintains stability of nerve membranes Required for muscle contraction Required for muscle contraction Necessary for many metabolic processes and enzyme reactions Necessary for many metabolic processes and enzyme reactions

49
CALCIUM IMBALANCES- Parathyroid regulates 2.2-2.7 mmol/L CALCIUM IMBALANCES- Parathyroid regulates 2.2-2.7 mmol/L HYPOCALCEMIA < 2.2mmol/L HYPOCALCEMIA < 2.2mmol/L Vit D deficiency, hypoparathyroidism, burns, acute pancreatitis, blood transfusions, accidental removal of parathyroid gland Vit D deficiency, hypoparathyroidism, burns, acute pancreatitis, blood transfusions, accidental removal of parathyroid gland Circumoral paresthesia, Trousseau ’ s sign(Figure 22-11), Chovestek ’ s sign(Figure 22-120,tetany, bleeding, cardiac dysrhythmias Circumoral paresthesia, Trousseau ’ s sign(Figure 22-11), Chovestek ’ s sign(Figure 22-120,tetany, bleeding, cardiac dysrhythmias Medical management- Oral calcium & vit D, IV calcium salt Medical management- Oral calcium & vit D, IV calcium salt HYPERCALCEMIA> 2.7mmol/L HYPERCALCEMIA> 2.7mmol/L Deep bone pain, constipation, N&V, polyuria, thirst, pathological fx, mental changes Deep bone pain, constipation, N&V, polyuria, thirst, pathological fx, mental changes Medical management- oral or IV sodium chloride & Lasix Medical management- oral or IV sodium chloride & Lasix
, Chovestek ’ s sign(Figure ,tetany, bleeding, cardiac dysrhythmias Circumoral paresthesia, Trousseau ’ s sign(Figure 22-11), Chovestek ’ s sign(Figure ,tetany, bleeding, cardiac dysrhythmias Medical management- Oral calcium & vit D, IV calcium salt Medical management- Oral calcium & vit D, IV calcium salt HYPERCALCEMIA> 2.7mmol/L HYPERCALCEMIA> 2.7mmol/L Deep bone pain, constipation, N&V, polyuria, thirst, pathological fx, mental changes Deep bone pain, constipation, N&V, polyuria, thirst, pathological fx, mental changes Medical management- oral or IV sodium chloride & Lasix Medical management- oral or IV sodium chloride & Lasix")
50
Nursing Management for Calcium Imbalances Nursing Management for Calcium Imbalances Monitor neurologic manifestations Monitor neurologic manifestations Bedrest Bedrest Signs of bleeding Signs of bleeding Increase oral intake & limit calcium Increase oral intake & limit calcium

51
Causes of Hypocalcemia Hypoparathyroidism Hypoparathyroidism Malabsorption Malabsorption Deficient serum albumin Deficient serum albumin Increased serum pH Increased serum pH Renal failure Renal failure

52
Effects of Hypocalcemia Spasms Spasms Weak heart contractions Weak heart contractions

53
Causes of Hypercalcemia Neoplasms Neoplasms Hyperthyroidism Hyperthyroidism Immobility Immobility Increased intake of calcium ion Increased intake of calcium ion Milk-akali syndrome Milk-akali syndrome

54
Effects of Hypercalcemia Depresses neuromuscular activity Depresses neuromuscular activity Interferes with ADH in kidneys Interferes with ADH in kidneys Strong heart contractions Strong heart contractions Effects bone Effects bone

55
Electrolytes Calcium (Ca 2+ ) Calcium (Ca 2+ ) Most abundant ion in body Most abundant ion in body plasma 4.6-5.5 mEq/liter plasma 4.6-5.5 mEq/liter most stored in bone (98%) most stored in bone (98%) Regulation: Regulation: Parathyroid Hormone (PTH) - blood Ca 2+ Parathyroid Hormone (PTH) - blood Ca 2+ Calcitonin (CT) - blood Ca 2+ Calcitonin (CT) - blood Ca 2+ Homeostatic imbalances: Homeostatic imbalances: Hypocalcemia - muscle cramps, convulsions Hypocalcemia - muscle cramps, convulsions Hypercalcemia - vomiting, cardiovascular symptoms, coma; prolonged abnormal calcium deposition, e.g., stone formation Hypercalcemia - vomiting, cardiovascular symptoms, coma; prolonged abnormal calcium deposition, e.g., stone formation
 Calcium (Ca 2+ ) Most abundant ion in body Most abundant ion in body plasma mEq/liter plasma mEq/liter most stored in bone (98%) most stored in bone (98%) Regulation: Regulation: Parathyroid Hormone (PTH) - blood Ca 2+ Parathyroid Hormone (PTH) - blood Ca 2+ Calcitonin (CT) - blood Ca 2+ Calcitonin (CT) - blood Ca 2+ Homeostatic imbalances: Homeostatic imbalances: Hypocalcemia - muscle cramps, convulsions Hypocalcemia - muscle cramps, convulsions Hypercalcemia - vomiting, cardiovascular symptoms, coma; prolonged abnormal calcium deposition, e.g., stone formation Hypercalcemia - vomiting, cardiovascular symptoms, coma; prolonged abnormal calcium deposition, e.g., stone formation")
56
Electrolytes Phosphate (H 2 PO 4 -, HPO 4 2-, PO 4 3- ) Phosphate (H 2 PO 4 -, HPO 4 2-, PO 4 3- ) Important ICF anions; plasma 1.7-2.6 mEq/liter Important ICF anions; plasma 1.7-2.6 mEq/liter most (85%) is stored in bone as calcium salts most (85%) is stored in bone as calcium salts also combined with lipids, proteins, carbohydrates, nucleic acids (DNA and RNA), and high energy phosphate transport compound also combined with lipids, proteins, carbohydrates, nucleic acids (DNA and RNA), and high energy phosphate transport compound important acid-base buffer in body fluids important acid-base buffer in body fluids Regulation - regulated in an inverse relationship with Ca 2+ by PTH and calcitonin Regulation - regulated in an inverse relationship with Ca 2+ by PTH and calcitonin Homeostatic imbalances Homeostatic imbalances Phosphate concentrations shift oppositely from calcium concentrations and symptoms are usually due to the related calcium excess or deficit Phosphate concentrations shift oppositely from calcium concentrations and symptoms are usually due to the related calcium excess or deficit
 Phosphate (H 2 PO 4 -, HPO 4 2-, PO 4 3- ) Important ICF anions; plasma mEq/liter Important ICF anions; plasma mEq/liter most (85%) is stored in bone as calcium salts most (85%) is stored in bone as calcium salts also combined with lipids, proteins, carbohydrates, nucleic acids (DNA and RNA), and high energy phosphate transport compound also combined with lipids, proteins, carbohydrates, nucleic acids (DNA and RNA), and high energy phosphate transport compound important acid-base buffer in body fluids important acid-base buffer in body fluids Regulation - regulated in an inverse relationship with Ca 2+ by PTH and calcitonin Regulation - regulated in an inverse relationship with Ca 2+ by PTH and calcitonin Homeostatic imbalances Homeostatic imbalances Phosphate concentrations shift oppositely from calcium concentrations and symptoms are usually due to the related calcium excess or deficit Phosphate concentrations shift oppositely from calcium concentrations and symptoms are usually due to the related calcium excess or deficit")
57
MAGNESIUM IMBALANCES – Normal range 1.3-2.1 mEq/L MAGNESIUM IMBALANCES – Normal range 1.3-2.1 mEq/L HYPOMAGNESEMIA < 1.3 mEq/L HYPOMAGNESEMIA < 1.3 mEq/L Chronic alcoholism,DKA, renal disease, burns, malnutrition, toxemia of pregnancy, diuresis, hyperaldosteronism, prolonged gastric suction Chronic alcoholism,DKA, renal disease, burns, malnutrition, toxemia of pregnancy, diuresis, hyperaldosteronism, prolonged gastric suction Tachycardia, leg & foot cramps, Chvostek ’ s & Trousseau ’ s signs,dysphagias, seizures Tachycardia, leg & foot cramps, Chvostek ’ s & Trousseau ’ s signs,dysphagias, seizures Medical management- oral or IV supplement Medical management- oral or IV supplement HYPERMAGNESEMIA- > 2.1 mEq/L HYPERMAGNESEMIA- > 2.1 mEq/L Renal failure, Addison ’ s Disease, excessive antacids or laxatives,hyperparathyroidism Renal failure, Addison ’ s Disease, excessive antacids or laxatives,hyperparathyroidism Flushing, hypotension, lethargy, bradycardia, depressed resp Flushing, hypotension, lethargy, bradycardia, depressed resp Medical management- decrease oral magnesium intake, dialysis, mechanical ven Medical management- decrease oral magnesium intake, dialysis, mechanical ven NURSING MANAGEMENT FOR MAGNESIUM IMBALANCES NURSING MANAGEMENT FOR MAGNESIUM IMBALANCES Antidote: Calcium Gluconate Antidote: Calcium Gluconate

58
Electrolytes Magnesium (Mg 2+ ) Magnesium (Mg 2+ ) 2 nd most abundant intracellular electrolyte, 1.3-2.1 mEq/liter in plasma 2 nd most abundant intracellular electrolyte, 1.3-2.1 mEq/liter in plasma more than half is stored in bone, most of the rest in ICF (cytoplasm) more than half is stored in bone, most of the rest in ICF (cytoplasm) important enzyme cofactor; involved in neuromuscular activity, nerve transmission in CNS, and myocardial functioning important enzyme cofactor; involved in neuromuscular activity, nerve transmission in CNS, and myocardial functioning Excretion of Mg 2+ caused by hypercalcemia, hypermagnesemia Excretion of Mg 2+ caused by hypercalcemia, hypermagnesemia Homeostatic imbalance Homeostatic imbalance Hypomagnesemia - vomiting, cardiac arrhythmias Hypomagnesemia - vomiting, cardiac arrhythmias Hypermagnesemia - nausea, vomiting Hypermagnesemia - nausea, vomiting
 Magnesium (Mg 2+ ) 2 nd most abundant intracellular electrolyte, mEq/liter in plasma 2 nd most abundant intracellular electrolyte, mEq/liter in plasma more than half is stored in bone, most of the rest in ICF (cytoplasm) more than half is stored in bone, most of the rest in ICF (cytoplasm) important enzyme cofactor; involved in neuromuscular activity, nerve transmission in CNS, and myocardial functioning important enzyme cofactor; involved in neuromuscular activity, nerve transmission in CNS, and myocardial functioning Excretion of Mg 2+ caused by hypercalcemia, hypermagnesemia Excretion of Mg 2+ caused by hypercalcemia, hypermagnesemia Homeostatic imbalance Homeostatic imbalance Hypomagnesemia - vomiting, cardiac arrhythmias Hypomagnesemia - vomiting, cardiac arrhythmias Hypermagnesemia - nausea, vomiting Hypermagnesemia - nausea, vomiting")
59
Acid-Base Balance Very important to maintain normal metabolism Very important to maintain normal metabolism pH 7.35-7.45 pH 7.35-7.45 H + HCO 3 - CO 2 H + HCO 3 - CO 2 Acidosis Acidosis Alkalosis Alkalosis Why a tendency towards lower pH? Why a tendency towards lower pH? Normal metabolism produces H + (acidity) Normal metabolism produces H + (acidity)
 Normal metabolism produces H + (acidity).")
60
H and pH

61
Acid-base balance pH of tissues regulated by: pH of tissues regulated by: chemical buffers (very rapid) chemical buffers (very rapid) Bicarbonate : very important buffer system Bicarbonate : very important buffer system Phosphate buffers Phosphate buffers Protein buffers Protein buffers respiratory compensation respiratory compensation Elimination of volatile acid (carbonic acid) by exhalation of CO 2 Elimination of volatile acid (carbonic acid) by exhalation of CO 2 renal compensation renal compensation Excretion of non-volatile acids (cannot be eliminated by exhaling CO 2 ) Excretion of non-volatile acids (cannot be eliminated by exhaling CO 2 )
 chemical buffers (very rapid) Bicarbonate : very important buffer system Bicarbonate : very important buffer system Phosphate buffers Phosphate buffers Protein buffers Protein buffers respiratory compensation respiratory compensation Elimination of volatile acid (carbonic acid) by exhalation of CO 2 Elimination of volatile acid (carbonic acid) by exhalation of CO 2 renal compensation renal compensation Excretion of non-volatile acids (cannot be eliminated by exhaling CO 2 ) Excretion of non-volatile acids (cannot be eliminated by exhaling CO 2 )")
62
Carbonic Acid - Bicarbonate Buffer Carbonic Acid - Bicarbonate Buffer A weak base H + + HCO 3 - H 2 CO 3 H 2 O + CO 2 A weak base H + + HCO 3 - H 2 CO 3 H 2 O + CO 2 Phosphate Buffer Phosphate Buffer NaOH + NaH 2 PO 4 H 2 O + Na 2 HPO 4 HCl + Na 2 HPO 4 NaCl + NaH 2 PO 4 Protein Buffer (esp. hemoglobin & albumin) Protein Buffer (esp. hemoglobin & albumin) Most abundant buffer in body cells and plasma Most abundant buffer in body cells and plasma Amino acids have amine group (proton acceptor = weak base) and a carboxyl group (proton donor = weak acid) Amino acids have amine group (proton acceptor = weak base) and a carboxyl group (proton donor = weak acid)
 Protein Buffer (esp. hemoglobin & albumin) Most abundant buffer in body cells and plasma Most abundant buffer in body cells and plasma Amino acids have amine group (proton acceptor = weak base) and a carboxyl group (proton donor = weak acid) Amino acids have amine group (proton acceptor = weak base) and a carboxyl group (proton donor = weak acid).")
63
Chemical buffer systems - proteins Most abundant buffers in ICF and blood plasma Most abundant buffers in ICF and blood plasma Carboxyl groups can act as an acid Carboxyl groups can act as an acid R-COOH R-COO - + H + R-COOH R-COO - + H + Amino group can act as a base: Amino group can act as a base: R-NH 2 + H + R-NH 3 + R-NH 2 + H + R-NH 3 + Side chains on some amino acids can also buffer Side chains on some amino acids can also buffer

64
Chemical buffer systems - bicarbonate Bicarbonate – major ECF buffer Bicarbonate – major ECF buffer H + + HCO 3 - H 2 CO 3 H + + HCO 3 - H 2 CO 3

65
Chemical buffer systems - phosphate Important in urine and ICF Important in urine and ICF Phosphate buffer system consists of: Phosphate buffer system consists of: dihydrogen phosphate (H 2 PO 4 - ) – weak acid dihydrogen phosphate (H 2 PO 4 - ) – weak acid OH - + H 2 PO 4 - H 2 O + HPO 4 2- OH - + H 2 PO 4 - H 2 O + HPO 4 2- monohydrogen phosphate (HPO 4 2- ) – weak base monohydrogen phosphate (HPO 4 2- ) – weak base H + + HPO 4 2- H 2 PO 4 - H + + HPO 4 2- H 2 PO 4 -
 – weak acid dihydrogen phosphate (H 2 PO 4 - ) – weak acid OH - + H 2 PO 4 - H 2 O + HPO 4 2- OH - + H 2 PO 4 - H 2 O + HPO 4 2- monohydrogen phosphate (HPO 4 2- ) – weak base monohydrogen phosphate (HPO 4 2- ) – weak base H + + HPO 4 2- H 2 PO 4 - H + + HPO 4 2- H 2 PO 4 -")
66
Acid-Base Imbalances Acidosis Acidosis High blood [H + ] High blood [H + ] Low blood pH, <7.35 Low blood pH, <7.35 Alkalosis Alkalosis Low blood [H + ] Low blood [H + ] High blood pH, >7.45 High blood pH, >7.45
![Acid-Base Imbalances Acidosis Acidosis High blood [H + ] High blood [H + ] Low blood pH, <7.35 Low blood pH, <7.35 Alkalosis Alkalosis Low blood [H + ] Low blood [H + ] High blood pH, >7.45 High blood pH, >7.45](http://images.slideplayer.com/47/11732757/slides/slide_66.jpg "Acid-Base Imbalances Acidosis Acidosis High blood [H + ] High blood [H + ] Low blood pH, <7.35 Low blood pH, <7.35 Alkalosis Alkalosis Low blood [H + ] Low blood [H + ] High blood pH, >7.45 High blood pH, >7.45")
67
Acid-base imbalances Arterial blood pH normally 7.4 Arterial blood pH normally 7.4 Acidosis – pH below 7.35 Acidosis – pH below 7.35 Alkalosis – pH above 7.45 Alkalosis – pH above 7.45 Acidosis Acidosis Depression of CNS activity through depression of synaptic transmission Depression of CNS activity through depression of synaptic transmission Alkalosis Alkalosis Overexcitability of CNS and peripheral nerves Overexcitability of CNS and peripheral nerves

68
Acid-Base imbalances may be due to problems with ventilation or due to a variety of metabolic problems Acid-Base imbalances may be due to problems with ventilation or due to a variety of metabolic problems Respiratory Acidosis (pCO 2 > 45 mm Hg) Respiratory Acidosis (pCO 2 > 45 mm Hg) Respiratory Alkalosis (pCO 2 < 35 mm Hg) Respiratory Alkalosis (pCO 2 < 35 mm Hg) Metabolic Acidosis (HCO 3 - < 23 mEq/l) Metabolic Acidosis (HCO 3 - < 23 mEq/l) Metabolic Alkalosis (HCO 3 - > 26 mEq/l) Metabolic Alkalosis (HCO 3 - > 26 mEq/l) Compensation: the physiological response to an acid-base imbalance begins with adjustments by the system less involved Compensation: the physiological response to an acid-base imbalance begins with adjustments by the system less involved
 Respiratory Acidosis (pCO 2 > 45 mm Hg) Respiratory Alkalosis (pCO 2 < 35 mm Hg) Respiratory Alkalosis (pCO 2 < 35 mm Hg) Metabolic Acidosis (HCO 3 - < 23 mEq/l) Metabolic Acidosis (HCO 3 - < 23 mEq/l) Metabolic Alkalosis (HCO 3 - > 26 mEq/l) Metabolic Alkalosis (HCO 3 - > 26 mEq/l) Compensation: the physiological response to an acid-base imbalance begins with adjustments by the system less involved Compensation: the physiological response to an acid-base imbalance begins with adjustments by the system less involved")
69
Acid base imbalances Respiratory acidosis and alkalosis Respiratory acidosis and alkalosis Disorders resulting from changes in partial pressure of CO 2 in arterial blood Disorders resulting from changes in partial pressure of CO 2 in arterial blood Metabolic acidosis and alkalosis Metabolic acidosis and alkalosis Disorders resulting from changes in HCO 3 - concentration in arterial blood Disorders resulting from changes in HCO 3 - concentration in arterial blood

70
Respiratory compensation Can compensate for metabolic acidosis/alkalosis Can compensate for metabolic acidosis/alkalosis H + buffered by bicarbonate to form CO 2 (or vice versa) H + buffered by bicarbonate to form CO 2 (or vice versa) H + + HCO 3 - H 2 CO 3 CO 2 + H 2 O H + + HCO 3 - H 2 CO 3 CO 2 + H 2 O
 H + buffered by bicarbonate to form CO 2 (or vice versa) H + + HCO 3 - H 2 CO 3 CO 2 + H 2 O H + + HCO 3 - H 2 CO 3 CO 2 + H 2 O")
71
Rising or falling H + from changes in metabolic acid production stimulate peripheral chemoreceptors increases or decreases ventilation to eliminate more or less CO 2 Rising or falling H + from changes in metabolic acid production stimulate peripheral chemoreceptors increases or decreases ventilation to eliminate more or less CO 2 Can achieve compensation in minutes to hours Can achieve compensation in minutes to hours

72
Renal compensation Can compensate for respiratory acidosis/alkalosis Can compensate for respiratory acidosis/alkalosis Also only means of eliminating nonvolatile acids (ie acids that cannot be converted to CO 2 ) Also only means of eliminating nonvolatile acids (ie acids that cannot be converted to CO 2 ) Can achieve compensation in days to weeks Can achieve compensation in days to weeks
 Also only means of eliminating nonvolatile acids (ie acids that cannot be converted to CO 2 ) Can achieve compensation in days to weeks Can achieve compensation in days to weeks")
73
Collecting duct (most important): Collecting duct (most important): One type of intercalated cell reduces blood acid load One type of intercalated cell reduces blood acid load secretes H + into tubular fluid against concentration gradient using proton pumps (H + ATPases) secretes H + into tubular fluid against concentration gradient using proton pumps (H + ATPases) H + in urine can be 1000 times higher than blood H + in urine can be 1000 times higher than blood Second type of intercalated cell increases blood acid load Second type of intercalated cell increases blood acid load secretes HCO 3 - into tubular fluid and reabsorbs H + secretes HCO 3 - into tubular fluid and reabsorbs H +
: Collecting duct (most important): One type of intercalated cell reduces blood acid load One type of intercalated cell reduces blood acid load secretes H + into tubular fluid against concentration gradient using proton pumps (H + ATPases) secretes H + into tubular fluid against concentration gradient using proton pumps (H + ATPases) H + in urine can be 1000 times higher than blood H + in urine can be 1000 times higher than blood Second type of intercalated cell increases blood acid load Second type of intercalated cell increases blood acid load secretes HCO 3 - into tubular fluid and reabsorbs H + secretes HCO 3 - into tubular fluid and reabsorbs H +")
74
Causes of Acid-Base Imbalances Respiratory Acidosis Respiratory Acidosis Chronic Obstructive Pulmonary Diseases e.g., emphysema, pulmonary fibrosis Chronic Obstructive Pulmonary Diseases e.g., emphysema, pulmonary fibrosis Pneumonia Pneumonia Respiratory Alkalosis Respiratory Alkalosis Hysteria Hysteria Fever Fever Asthma Asthma

75
Causes of Acid-Base Imbalances Metabolic Acidosis Metabolic Acidosis Diabetic ketoacidosis, Lactic acidosis Diabetic ketoacidosis, Lactic acidosis Salicylate poisoning (children) Salicylate poisoning (children) Methanol, ethylene glycol poisoning Methanol, ethylene glycol poisoning Renal failure Renal failure Diarrhea Diarrhea Metabolic Alkalosis Metabolic Alkalosis Prolonged vomiting Prolonged vomiting Diuretic therapy Diuretic therapy Hyperadrenocortical disease Hyperadrenocortical disease Exogenous base (antacids, bicarbonate IV, citrate toxicity after massive blood transfusions) Exogenous base (antacids, bicarbonate IV, citrate toxicity after massive blood transfusions)
 Salicylate poisoning (children) Methanol, ethylene glycol poisoning Methanol, ethylene glycol poisoning Renal failure Renal failure Diarrhea Diarrhea Metabolic Alkalosis Metabolic Alkalosis Prolonged vomiting Prolonged vomiting Diuretic therapy Diuretic therapy Hyperadrenocortical disease Hyperadrenocortical disease Exogenous base (antacids, bicarbonate IV, citrate toxicity after massive blood transfusions) Exogenous base (antacids, bicarbonate IV, citrate toxicity after massive blood transfusions)")
76
Effects of Acidosis Direct Direct Headache, lethargy, weakness, confusion Headache, lethargy, weakness, confusion

77
Effects of Alkalosis Restlessness, muscle twitching, tingling, numbness Restlessness, muscle twitching, tingling, numbness

78
Medication : Medication : 1) Metabolic Acidosis : 1) Metabolic Acidosis : 2) Respiratory Alkalosis: 2) Respiratory Alkalosis: 3) Respiratory Acidosis: 3) Respiratory Acidosis: 4) Respiratory Alkalosis: 4) Respiratory Alkalosis:
 Metabolic Acidosis : 1) Metabolic Acidosis : 2) Respiratory Alkalosis: 2) Respiratory Alkalosis: 3) Respiratory Acidosis: 3) Respiratory Acidosis: 4) Respiratory Alkalosis: 4) Respiratory Alkalosis:")
Similar presentations















![1 Acid and Base Balance and Imbalance. 2 pH Review pH = - log [H + ] H + is really a proton Range is from 0 - 14 If [H + ] is high, the solution is acidic;](/14/4450368/big_thumb.jpg "1 Acid and Base Balance and Imbalance. 2 pH Review pH = - log [H + ] H + is really a proton Range is from 0 - 14 If [H + ] is high, the solution is acidic;>")
 Early embryo = 97% water B) Newborn infant = 77% water C) Adult.>")
 Assistant Prof. in Pathology Al Maarefa College.>")
![1. pH = - log [H + ] H + is really a proton Range is from 0 - 14 If [H + ] is high, the solution is acidic; pH < 7 If [H + ] is low, the solution.](/15/4651316/big_thumb.jpg "1. pH = - log [H + ] H + is really a proton Range is from 0 - 14 If [H + ] is high, the solution is acidic; pH < 7 If [H + ] is low, the solution.>")
