Download presentation
Presentation is loading. Please wait.

1
Radial extracorporeal shockwave therapy Basic physics, biological effects, indications & integration with multidisciplinary practice The Swiss dolorclast method Dr.Haffed Gritly United Rings CEO

2
What are shock waves? A shock wave (also called shock front or simply "shock") is a type of propagating disturbance. Like an ordinary wave, it carries energy and can propagate through a medium (solid, liquid or gas) [...]. Shock waves are characterized by an abrupt, nearly discontinuous change in the characteristics of the medium. Across a shock there is always an extremely rapid rise in pressure, temperature and density of the flow. [...] A shock wave travels through most media at a higher speed than an ordinary wave..
 is a type of propagating disturbance. Like an ordinary wave, it carries energy and can propagate through a medium (solid, liquid or gas) [...]. Shock waves are characterized by an abrupt, nearly discontinuous change in the characteristics of the medium. Across a shock there is always an extremely rapid rise in pressure, temperature and density of the flow. [...] A shock wave travels through most media at a higher speed than an ordinary wave...")
3
Encyclopedia Britannica online: a „[...] strong pressure wave in any elastic medium such as air, water, or a solid substance, produced by supersonic aircraft, explosions, lightning, or other phenomena that create violent changes in pressure. Shock waves differ from sound waves in that the wave front, in which compression takes place, is a region of sudden and violent change in stress, density, and temperature. Because of this, shock waves propagate in a manner different from that of ordinary acoustic waves. In particular, shock waves travel faster than sound, and their speed increases as the amplitude is raised; but the intensity of a shock wave also decreases faster than does that of a sound wave, because some of the energy of the shock wave is expended to heat the medium in which it travels." What are shock waves?
![ Encyclopedia Britannica online: a „[...] strong pressure wave in any elastic medium such as air, water, or a solid substance, produced by supersonic aircraft, explosions, lightning, or other phenomena that create violent changes in pressure.](http://images.slideplayer.com/47/11717371/slides/slide_3.jpg "Shock waves differ from sound waves in that the wave front, in which compression takes place, is a region of sudden and violent change in stress, density, and temperature. Because of this, shock waves propagate in a manner different from that of ordinary acoustic waves. In particular, shock waves travel faster than sound, and their speed increases as the amplitude is raised; but the intensity of a shock wave also decreases faster than does that of a sound wave, because some of the energy of the shock wave is expended to heat the medium in which it travels. What are shock waves .")
4
Important characteristics of therapeutic extracorporeal shock waves Ogden et al., Clin Orthop Rel Res 2001;(387):8-17: Shrivastava and Kailash, J Biosci 2005;30:269-275:
:8-17: Shrivastava and Kailash, J Biosci 2005;30: :")
5
Generation of therapeutic shock waves 5 piezo-electric electro- hydraulic electro- magnetic pneumatic Ossatron Orbason Orthospec Epos Ultra Sonocur Swiss Dolorclast D-ACTOR Four principles to generate therapeutic shock waves

6
Mode of operation of radial shock wave devices (Swiss Dolorclast)
")
7
Therapeutic shock waves generated with the Dolorclast Ogden et al. (2001): “[...] a high peak pressure, sometimes more than 100 MPa (500 bar), but more often approximately 50 to 80 MPa, a fast initial rise in pressure during a period of less than 10 ns, a low tensile amplitude (up to 10 MPa), a short life cycle of approximately 10 µs, and [...].” 10 −6 (Source: Chitnis PV, Cleveland RO: Acoustic and cavitation fields of shock wave therapy devices. In: Clement GT, McDannold NJ, Hynynen K: CP829, Therapeutic Ultrasound: 5th international symposium on therapeutic ultrasound. 2006, American Institute of Physics.)
: [...] a high peak pressure, sometimes more than 100 MPa (500 bar), but more often approximately 50 to 80 MPa, a fast initial rise in pressure during a period of less than 10 ns, a low tensile amplitude (up to 10 MPa), a short life cycle of approximately 10 µs, and [...]. 10 −6 (Source: Chitnis PV, Cleveland RO: Acoustic and cavitation fields of shock wave therapy devices. In: Clement GT, McDannold NJ, Hynynen K: CP829, Therapeutic Ultrasound: 5th international symposium on therapeutic ultrasound. 2006, American Institute of Physics.).")
8
FOCUSED ESWT

9
Therapeutic shock waves generated with the Ossatron (Source: Chitnis PV, Cleveland RO: Acoustic and cavitation fields of shock wave therapy devices. In: Clement GT, McDannold NJ, Hynynen K: CP829, Therapeutic Ultrasound: 5th international symposium on therapeutic ultrasound. 2006, American Institute of Physics.)
.")
10
Measuring the rise time and pulse duration of the shock waveform oscilloscope sampling rate increased to 100 Msmp/s

11
Therapeutic relevant part of shock waves A significant tissue effect is cavitation consequent to the negative phase of the wave propagation." (Ogden et al., 2001)
")
12
Cavitations created by Radial shockwave therapy

13
Cavitations created by Focused shockwave therapy

14
Swiss Dolorclast Is a FDA Class I approved device for treatment of orthopedic conditions in podiatry, physiotherapy, sports medicine and rehabilitation. EMS/Dolorclast was first to develop Lithtripsy. Since 1990 (ESWT) has been used for a variety of orthopaedic applications. More recently it is used for treating wound ulcers, lymphodema, burns and cellulite.
 has been used for a variety of orthopaedic applications. More recently it is used for treating wound ulcers, lymphodema, burns and cellulite..")
15
SWISS DOLORCLAST EVO BLUE

16
HIGH-SPEED PHOTOGRAPhY WITH SEVERAL MILLION frames PER SECOND

17
Mechanism philosophy The Radial ESWT procedure accelerates the body’s own healing by: 1.Generating impulses of high energy, high pressure sound waves that travel through skin to stimulate healing. 2.It is effectively changing a chronic condition to an acute condition.

18
SHOCK WAVES act on musculoskeletal tissue through variousEffects 1 Maier et al., 2003. 2 Zhang et al., 2011. 3 Application of shock waves usually results in reddening of the skin, which indicates increased blood supply. 4 Hofmann et al., J Trauma 2008. 5 Radial ESWT: Gollwitzer et al., 2013; focused ESWT: Tischer et al., 2008, among many others.

19
19 RSWT ® : mechanisms of action Prolonged activation of pain and heat sensing neurons (unmyelinated C fibers) by capsaicin depletes presynaptic substance P, one of the body's neurotransmitters for pain and heat. The result appears to be that capsaicin mimics a burning sensation, the nerves are overwhelmed by the influx, and are unable to report pain for an extended period of time. With chronic exposure to capsaicin, neurons are depleted of neurotransmitters and it leads to reduction in sensation of pain and blockade of neurogenic inflammation. If capsaicin is removed, the neurons recover. RSWT ® : mechanism of short-term action

20
RSWT ® : Basic physics - cavitation A significant tissue effect is cavitation consequent to the negative phase of the wave propagation

21
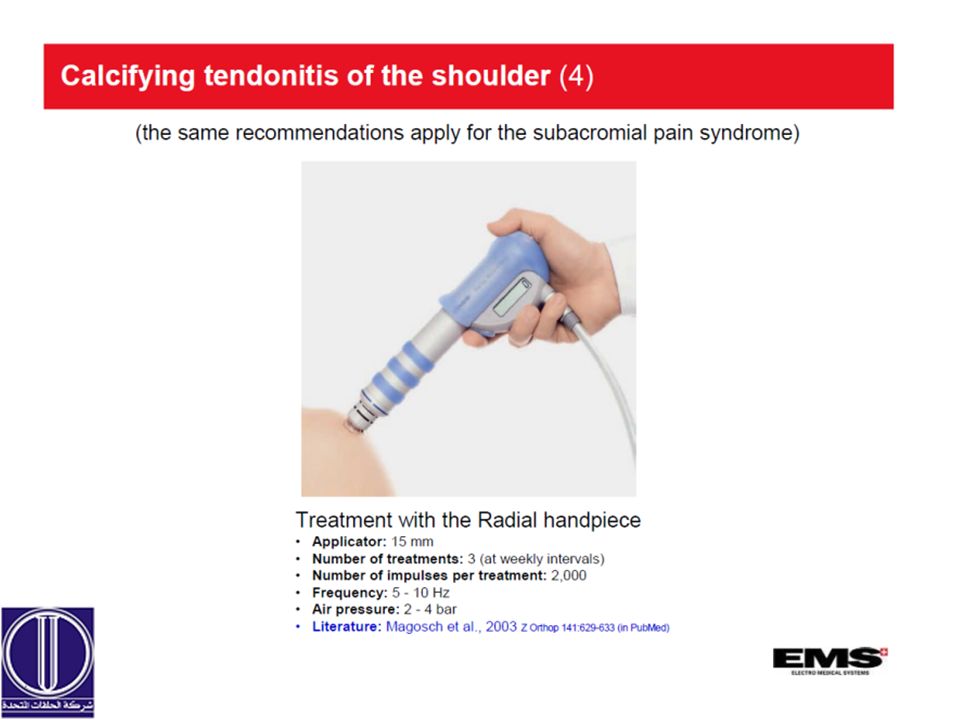
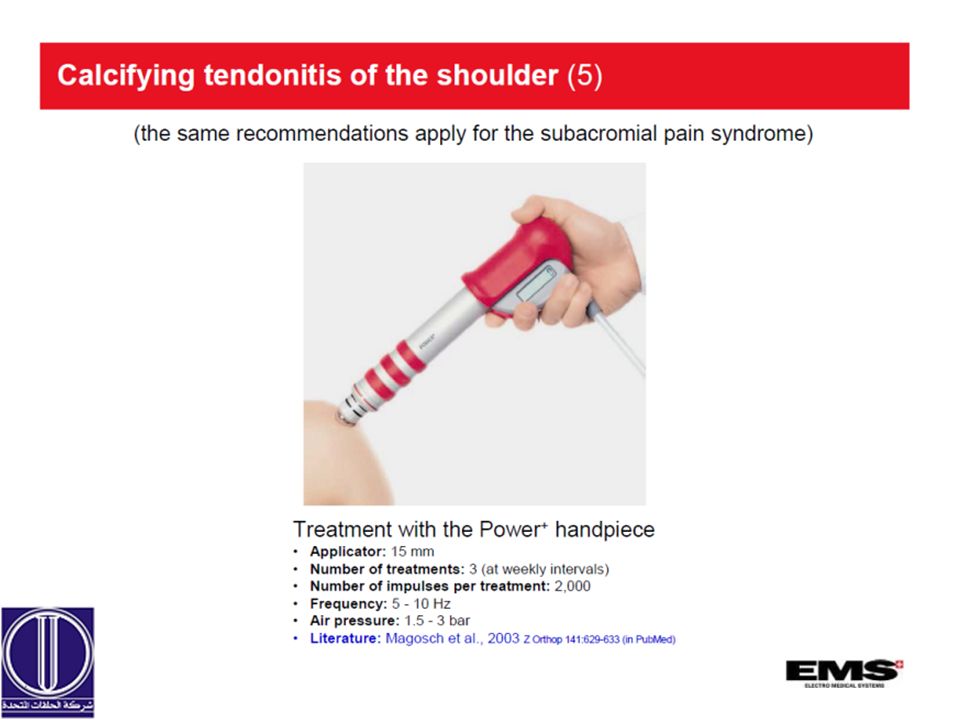
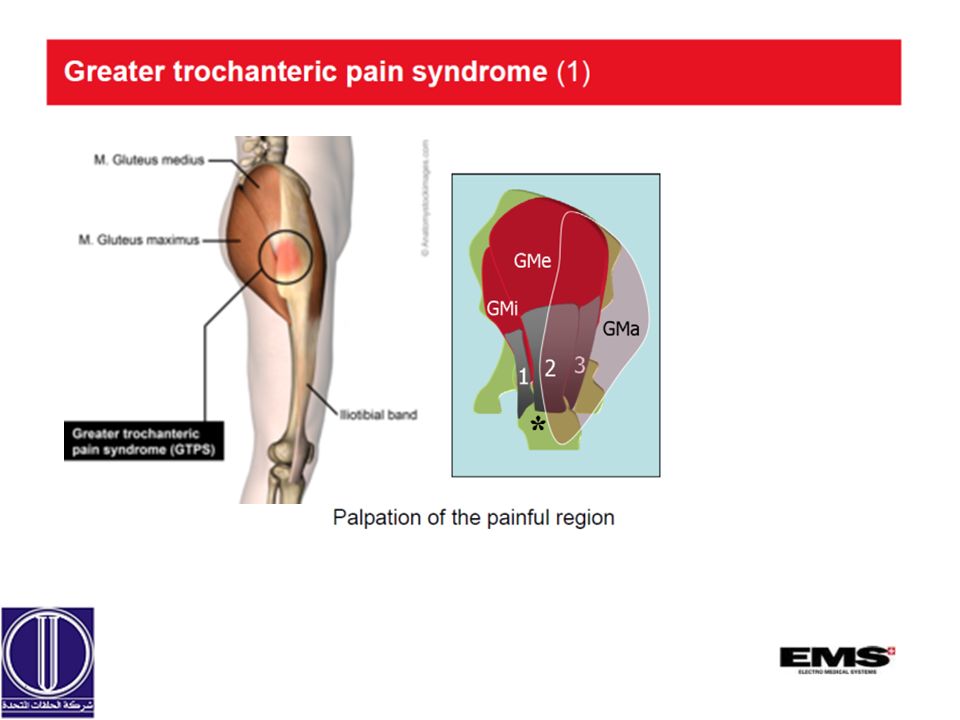
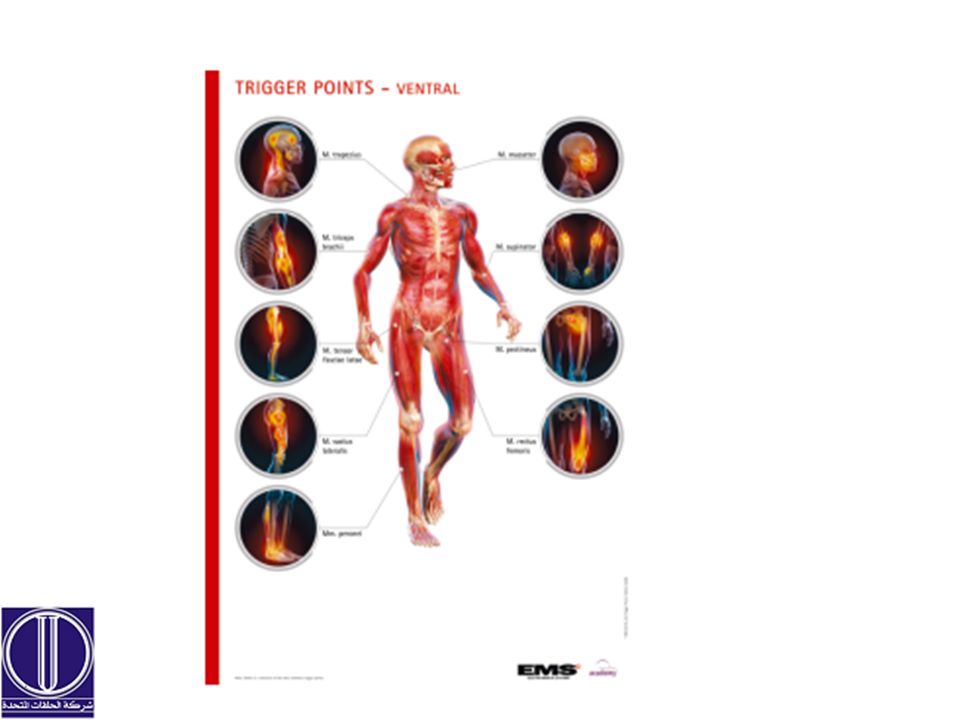
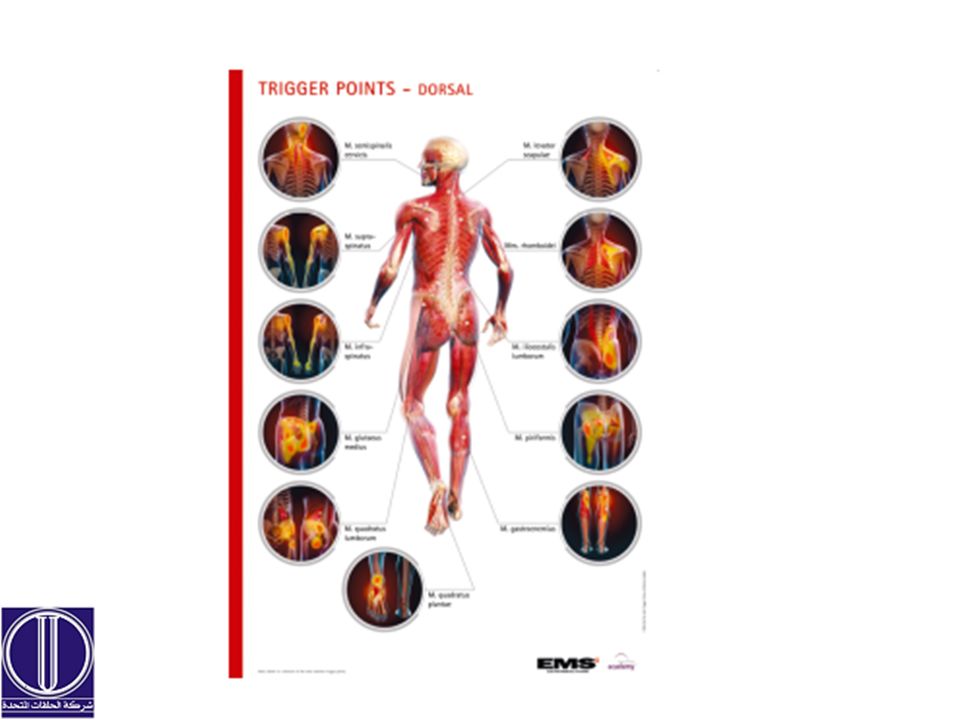
Focused vs. radial shock waves – what, when? Preference for radial shock waves: Superficial indications: – Plantar fasciopathy, Achilles tendinopathy, medial tibial stress syndrome, greater trochanteric pain syndrome Preference for focused shock waves: Deep indications: – Calcifying tendinosis of the shoulder (Vavken et al., 2009; Rompe, 2009) – Pseudarthroses – Avascular necrosis of the femoral head Recommendation for both radial or focused shock waves: Trigger point treatment – Treatment with radial shock waves: ATRAD – Treatment with focused shock waves: Müller-Ehrenberg, 2009 Preference to offer both radial and focused shock waves: Method switch in non-responders 21
 – Pseudarthroses – Avascular necrosis of the femoral head Recommendation for both radial or focused shock waves: Trigger point treatment – Treatment with radial shock waves: ATRAD – Treatment with focused shock waves: Müller-Ehrenberg, 2009 Preference to offer both radial and focused shock waves: Method switch in non-responders 21.")
22
Extracoropreal radial shockwave therapy by swiss dolorclast →15 OUT OF THE 20 CLINICAL RSWT STUDIES LISTED IN THE PEDro DATABASE WERE PERFORMED WITH THE SWISS DOLORCLAST®

25
MSK Sonography of supraspinatus tendon Supraspinatus Tendinopathy

26
MSK Sonography of supraspinatus Tendon Full rupture of supraspinatus with retraction

33
MSK Sonography of Common Extensor tendon

38
MSK Sonography of Patella Tip syndrome

45
MSK Sonography of Achilles Tensdon insertion

48
MSK Sonography of Achilles Tendon Midbody

51
MSK Sonography of Plantar fascia

53
Static Pedobarography Fore feet valgus. Hind-feet valgus. Low Esp Right medial longitudinal arch

54
Dynamic Pedobarography

58
Functional spinal assessment with spinal mouse

59
TENSION TYPE HEADACHE EVOBLUE Handpeice. 4000 – 6000 pulses. At 20HZ. 5 mins.

66
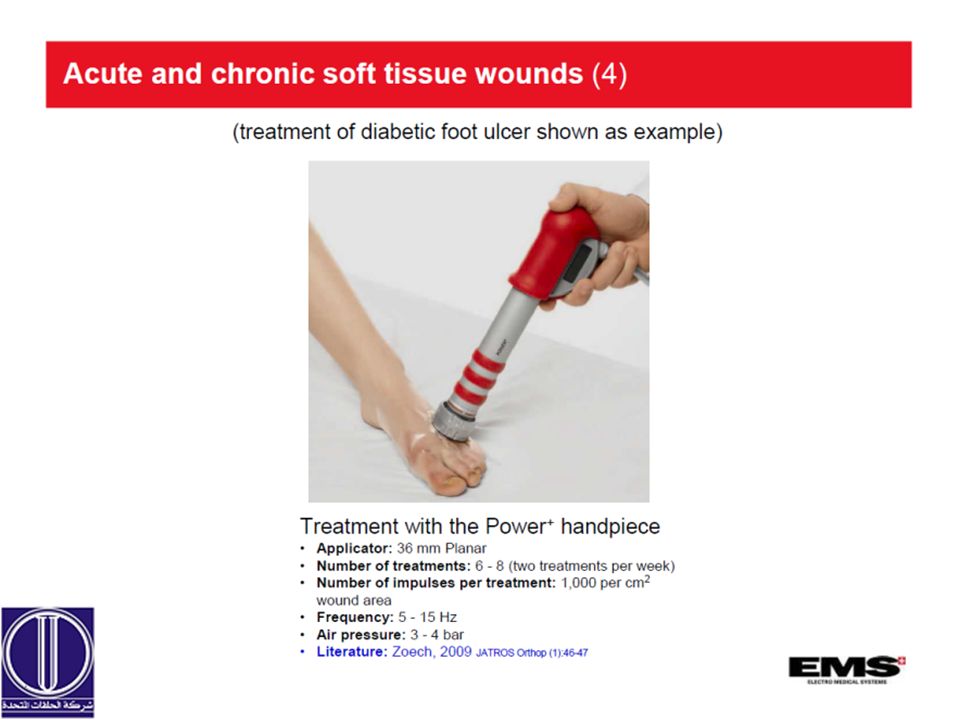
Case study Reluctant large Diabetic foot ulceration at Hairmyres Hospial in Scotland. Patient had surgical debridement and lavage therapy and not responding to treatment with high chance of lower limb amputation. Patient was treated with ESWT over 6Months with full healing with an average of one session every 2.5 weeks.

72
Thank you

84
DiaCaRe The new frontier of the tecartherapy

85
DiaCaRe WHAT IS TECARTHERAPY? Tecartherapy is an acronym of Capacitive and Resistive Energy Transfer (the principle of the therapy).
..")
86
DiaCaRe TECARTHERAPY is an ENDOGENOUS THERAPY which uses the HEAT generated INSIDE the human body. For this reason, TECARTHERAPY is also known as DIATHERMY.

87
DiaCaRe Thermotherapy has been known and used for many years to treat painful articular and muscle pathologies. However, with the EXOGENOUS techniques used so far (infrared, ultrasound, laser), the HEAT CAN PENETRATE DEEPLY only using high power.
, the HEAT CAN PENETRATE DEEPLY only using high power..")
88
DiaCaRe In the majority of cases, the EXOGENOUS heat (coming from outside) drops to the BASELINE VALUE of 37° after few millimeters from the surface, thus losing its therapeutic effectiveness.
 drops to the BASELINE VALUE of 37° after few millimeters from the surface, thus losing its therapeutic effectiveness.")
89
DiaCaRe TECARTHERAPY can generate heat in a homogeneous and diffused way, penetrating deep inside the human tissues and giving a comfortable sensation.

90
DiaCaRe This new technology, which generates heat inside the tissues, is more effective and gives better results.

91
DiaCaRe PRINCIPLE OF ACTION of TECARTHERAPY The heating of tissues obtained by means of high frequency currents has been known since 1897. Back in 1902 it was named DIATHERMY. TECARTHERAPY uses a SINUSOIDAL current with high frequency (500 KHz) that is applied to the human body.
 that is applied to the human body..")
92
DiaCaRe The sinusoidal current imply a very fast alternation of electric charges through the tissues. This very fast movement brings about an INCREASE IN TEMPERATURE, due to the Joule effect.

93
DiaCaRe EFFECTS ON TISSUES Temperature rise → it opens the capillary and pre- capillary circuit (100,000 capillaries per cm3) → it increases blood volume → it increases the oxygen and nutrient supply to the cells → it increases the metabolic reaction speed → it has a biostimulant effect
 → it increases blood volume → it increases the oxygen and nutrient supply to the cells → it increases the metabolic reaction speed → it has a biostimulant effect")
94
DiaCaRe EFFECTS ON THE LYMPHATIC SYSTEM Temperature rise → it stimulates the lymphatic system → it opens up lymphatic vessels → lymphatic drainage

95
DiaCaRe EFFECTS ON THE CELL The electric charge flow → modifies the permeability of the cell wall → modifies the osmotic flow and the distribution of the flow between cells and the interstitial space → favours the drainage of effusions and edemas

96
DiaCaRe EFFECTS ON PAIN Temperature rise → it inhibits pain receptors → it stimulates the release of endorphins → it has a direct pain sedative action on the pain zone

97
DiaCaRe SELECTIVE AND FOCUSED THERAPEUTIC ACTION Thanks to TECARTHERAPY, its treatment modes and the different energy levels used, the action can be focused on the points where the therapeutic action is needed.

98
DiaCaRe TECARTHERAPY TREATMENT MODES Tecartherapy uses 2 different treatment modes: CAPACITIVE Mode RESISTIVE Mode What is the difference?

99
DiaCaRe CAPACITIVE MODE It uses an insulated active electrode and a counter-electrode (a metal plate). Specific action to treat tissues with low resistance to electric current passage: Cutaneous tissue Connective tissue Muscle tissue Lymphatic system Circulatory system The therapeutic action concentrates on the soft tissues under the active electrode.

100
DiaCaRe RESISTIVE MODE It uses non-insulated electrodes. It is recommended for tissues with greater resistance to electric current passage: Bone tissue Cartilage tissue Tendons and ligaments Aponeurotic band Fibrotic tissue The therapeutic action takes place between the electrodes (even in depth).
..")
101
DiaCaRe RESISTIVE MODE OF DIACARE DiaCaRe uses non-insulated active electrodes with different configurations. A – Active handpiece and metal plate counter-electrode (DUAL-TRODE) B – One handpiece (MONO-TRODE) with 2 concentric electrodes (one electrode and one counter-electrode).
 B – One handpiece (MONO-TRODE) with 2 concentric electrodes (one electrode and one counter-electrode)..")
102
DiaCaRe DUALTRODE MONOTRODE

103
DiaCaRe Depending on the pathologies to treat and their location, TECARTHERAPY can use the two modes (capacitive and resistive) even in sequence. Resistive mode is the most used because it can penetrate in depth and bring energy to the articulations.

104
DiaCaRe Regardless the selected mode, INCREASING the POWER in the device generates a GREATER ENERGY TRANSFER that BRINGS ABOUT DIFFERENT THERAPEUTIC EFFECTS.

105
DiaCaRe Muscle pathologies - Contracture - Strain and Sprain - Contusion - Edema Pathologies of the spinal column - Low back pain - Dorsalgia - Cervicalgia Shoulder Pathologies - Tendinitis and tenosynovitis - Insertional tendinopathy - Adhesive capsulitis Elbow pathologies - Epicondylitis - Medial epicondylitis

106
DiaCaRe Wrist and hand pathologies - Tendinitis and tenosynovitis - Rhizarthrosis Hip pathologies - Coxarthrosis - Bursitis - Osteitis pubis Knee pathologies - Patellar chondropathy - Gonarthrosis - Consequences of ALC/PLC injuries - Sprains Ankle and foot pathologies - Consequences of bone fractures - Sprains - Plantar fasciitis - Achille’s tendinitis

107
Physiotherapy evidence database PEDro pedro.org.au CEBP in 1999 +32K RCT, practice guidelines & clinical trials PEDro scale: 1.eligibility criteria were specified 2.subjects were randomly allocated to groups (in a crossover study, subjects were randomly allocated an order in which treatments were received)
")
108
PEDro scale (Continue) 3. Allocation was concealed 4. The groups were similar at baseline regarding the most important prognostic indicators 5. There was blinding of all subjects 6. There was blinding of all therapists who administered the therapy 7. there was blinding of all assessors who measured at least one key outcome

109
PEDro scale (Continue) 8. measures of at least one key outcome were obtained from more than 85% of the subjects initially allocated to groups. 9. all subjects for whom outcome measures were available received the treatment or control condition as allocated or, where this was not the case, data for at least one key outcome was analysed by “intention to treat”. 10. the results of between-group statistical comparisons are reported for at least one key outcome

110
PEDro scale (Continue) 11. the study provides both point measures and measures of variability for at least one key outcome.

Similar presentations










































>")






