Download presentation
Presentation is loading. Please wait.

1
Based on : 2010 American Heart Association Guidelines www.circ.ahajournals.org Elham Pishbin. M.D Assistant Professor of Emergency Medicine MUMS Management of Cardiac Arrest

2
ARREST Unresponsive patient C A B Chest Open Breathing Compression Air way No breathing and pulse No breathing and pulse

4
Start The patient Not monitored Monitored

5
Advanced Life Support A B C CHESTCOMp

6
Defibrillator attached C H E S T C O M p

7
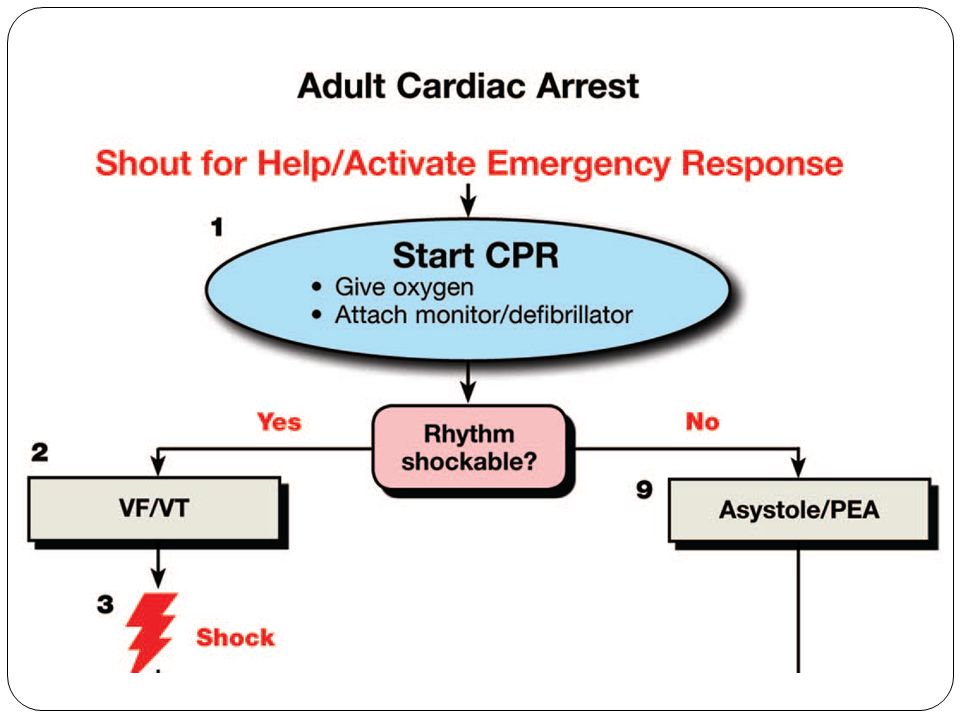
Check Rhythm VT, VF PEA, Asystole

10
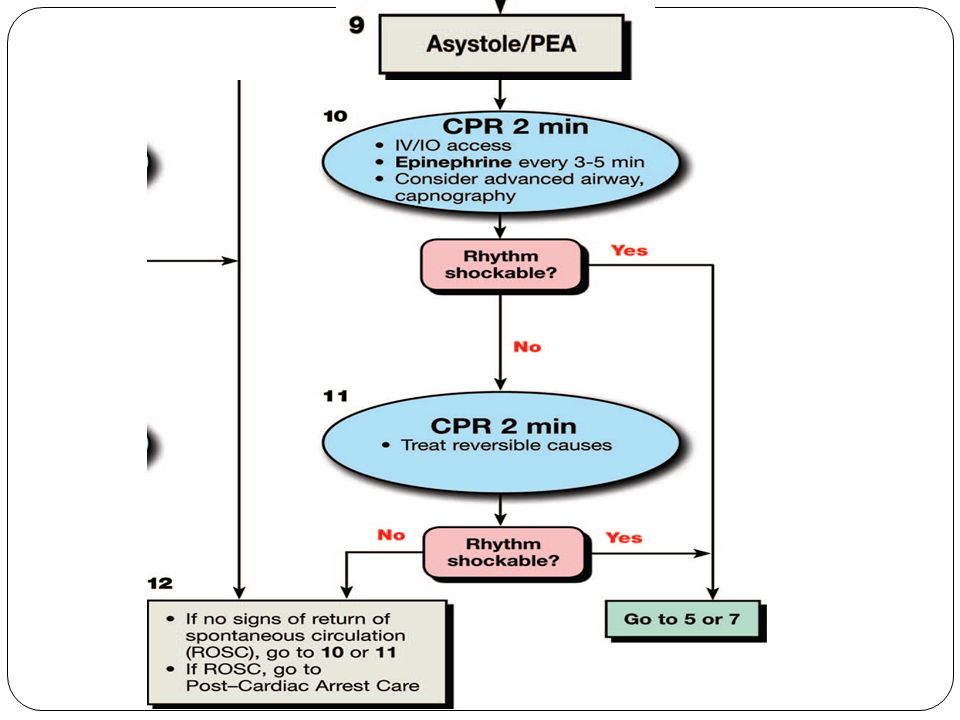
Asystole / PEA Asystole / PEA PEA PEA : a heterogeneous group of organized electric rhythms, with either absence of mechanical ventricular activity or mechanical ventricular activity that is insufficient to generate a clinically detectable pulse. Asystole Asystole : absence of detectable ventricular electric activity with or without atrial electric activity.

12
DON’T INTERRUPT CHEST COMPRESSION DON’T INTERRUPT CHEST COMPRESSION as brief as possible Periodic pauses in CPR should be as brief as possible and only as necessary to assess rhythm, shock VF/VT, perform a pulse check when an organized rhythm is detected, or place an advanced airway.

13
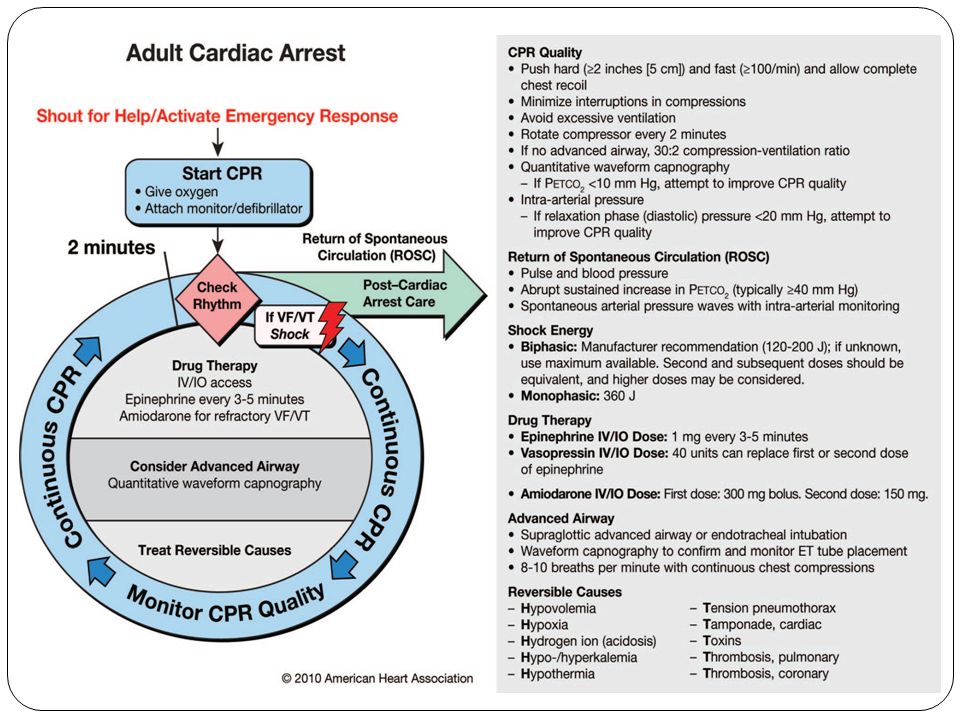
Chest comp. Rate = 100 Without interruption Change hand Q 2 min / max. 5sec delay Push hard, Push fast Allow to enough chest recoil Compress 3-5 cm in adult 1/3 to ½ depth of chest in childrenCHESTCOMp

14
High quality CPR Monitoring and optimizing quality of CPR on the basis of 1- Mechanical parameters: (rate & depth of compressions, relaxation, and minimization of pauses) 2- Physiologic parameters : (PETCO2, arterial pressure during the relaxation phase of chest compressions, or ScvO2 )
 2- Physiologic parameters : (PETCO2, arterial pressure during the relaxation phase of chest compressions, or ScvO2 )")
16
Asystole / PEA (cont…) The ability to achieve a good resuscitation outcome depends on: 1-Provide effective CPR 2-Identify and correct a cause of PEA / Asystole All resuscitation team members must simultaneously Conduct a search for a underlying and treatable cause of the PEA in addition to performing their assigned role.
 The ability to achieve a good resuscitation outcome depends on: 1-Provide effective CPR 2-Identify and correct a cause of PEA / Asystole All resuscitation team members must simultaneously Conduct a search for a underlying and treatable cause of the PEA in addition to performing their assigned role.")
17
Asystole / PEA (cont…)
")
18
Asystole : Asystole : It is should be confirm that: -Not another rhythm masquerading as a flat line -Not the result of an operator error that is creating a flat line Causes of an Isoelectric ECG: -Loose leads or leads not connected to the patient or defibrillator/monitor -No power -Signal gain too low

19
Drug Therapy in Asys / PEA A vasopressor can be given as soon as feasible with the primary goal of increasing myocardial and cerebral blood flow during CPR and achieving ROSC. Available evidence suggests that the routine use of atropine during PEA or asystole is unlikely to have a therapeutic benefit, SO Atropine has been removed from the cardiac arrest algorithm. the cardiac arrest algorithm.

21
V.F / Pulse-less V.T The foundation of successful ACLS is : high quality CPR, and, for VF/pulseless VT, attempted defibrillation within minutes of collapse. For victims of witnessed VF arrest, early CPR and rapid defibrillation can significantly increase the chance for survival to hospital discharge. In comparison, other ACLS therapies such as some medications and advanced airways, although associated with an increased rate of ROSC, have not been shown to increase the rate of survival to hospital discharge.

22
V.F / Pulse-less V.T In addition to high-quality CPR, the only rhythm-specific therapy proven to increase survival to hospital discharge is defibrillation of VF/pulseless VT. Other ACLS interventions during cardiac arrest may be associated with an increased rate of ROSC but have not yet been proven to increase survival to hospital discharge.

23
Therefore They are recommended as considerations and should be performed without compromising quality of CPR or timely defibrillation

24
V.F / Pulse-less V.T In other words : vascular access, drug delivery, and advanced airway should not cause significant interruptions in chest compression or delay defibrillation. There is insufficient evidence to recommend a specific timing or sequence (order) of drug administration and advanced airway placement during cardiac arrest.
 of drug administration and advanced airway placement during cardiac arrest..")
25
Chest comp

26
Rhythm Shockable Nonshockable VF Asystole Pulseless VT PEA

27
Shockable rhythm VF, Pulseless VT Witnessed, early mins LateCHESTCOMp

28
V.F / Pulse-less V.T When VF is present for more than a few minutes, myocardium is depleted of oxygen and metabolic substrates. A brief period of chest compressions can deliver oxygen and energy and “unload” the volume- overloaded R.V, increasing the likelihood of returning a perfusing rhythm after shock. Performing CPR while a defibrillator is readied for use is strongly recommended for all patients in cardiac arrest

29
V.F / Pulse-less V.T The shorter the time interval between the last chest compression and shock delivery, the more likely the shock will be successful. A reduction of even a few seconds in the interval from pausing compressions to shock delivery can increase the probability of shock success

30
V.F / Pulse-less V.T The value of intentionally delaying defibrillation to perform CPR is less clear. At this time the benefit of delaying defibrillation to perform CPR before defibrillation is unclear

31
Shock ? Monophasic 360 J / at beginning Biphasic 120 J / then 200 J Children first 2 J/kg then 4 J/kgCHESTCOMp

32
Drug Therapy in V.F / Pulse-less V.T When VF/pulseless VT persists after at least 1 shock and a 2-minute CPR period, a vasopressor can be given with the primary goal of increasing myocardial blood flow during CPR and achieving ROSC. If a shock fails to generate a perfusing rhythm, then giving a vasopressor soon after the shock will optimize the potential impact of increased myocardial blood flow before the next shock.

33
Drug Therapy in V.F / Pulse-less V.T Amiodarone is the first-line antiarrhythmic agent given during cardiac arrest because it has been clinically demonstrated to improve the rate of ROSC and hospital admission in adults with refractory VF/pulseless VT. Amiodarone considered when VF/VT is unresponsive to CPR, defibrillation, and vasopressor therapy. If amiodarone is unavailable, lidocaine may be considered. Magnesium sulfate should be considered only for torsades de point.

34
As A Rule : All drugs in CPR are given I.V Push. All drugs in CPR are given I.V Push. and then 20 cc N.S. and then 20 cc N.S.

35
During cardiac arrest, provision of high-quality CPR and rapid defibrillation are of primary importance and drug administration is of secondary importance. After beginning CPR and attempting defibrillation for identified VF or pulseless VT, providers can establish IV or IO access. This should be performed without interrupting chest compressions.

36
If IV or IO access cannot be established, epinephrine, vasopressin, and lidocaine may be administered by the endotracheal route during cardiac arrest. The optimal endotracheal dose of most drugs is unknown, but typically the dose is 2 to 21⁄2 times of the recommended IV dose.

38
0- shock chest comp check rhythm 2- shock chest comp. 1 mg Epinephrine check rhythm 4- shock chest comp, Amiodarone 300 mg check rhythm 6- shock chest comp, EpiCHESTCOMp

39
Do not check pulse until The rhythm changedCHESTCOMp

40
8- shock chest comp. check rhythm 10- shock chest comp, Epi check rhythm 12- shock chest comp. check rhythm 14- shock chest comp. Epi check rhythmCHESTCOMp

41
16- shock chest comp, Amiodarone 150 mg check rhythm 18- shock chest comp, Epi check rhythm 20- shock chest comp. : : :CHESTCOMp

42
Drugs Antiarrhythmic: Amiodarone : 300 mg first dose if needed after 15-20 min, 150 mg max, 450 m g Lidocaine : 1.5 mg/kg first dose if needed Q 10 min--- 0.75 mg/kg for 2 doses max. 3 mg/kg

43
Vasopressors Epinephrine hydrochloride: S & NS rhythms 1 mg- IV, IO, ET Q 3-5 min/ cont to END Atropine: Forget about it …!

44
Drug rout As a law: Drugs injections in CPR must be: PUSH ETT administration: 2 - 2.5 times as IV doses plus 5-10 ml distilled water As a law: Drugs injections in CPR must be: PUSH ETT administration: 2 - 2.5 times as IV doses plus 5-10 ml distilled waterCHESTCOMp

45
Prolonged CPR Hypothermia Toxicity DrowningCHESTCOMpCHESTCOMp

Similar presentations



















 Advanced Life Support (ALS) Dr. Yasser Mostafa Prof. of Chest Diseases Ain Shams University.>")


: Rockefeller Oteng (University of Michigan),>")
>")