Download presentation
Presentation is loading. Please wait.

2
CSCCN Central South Coast Cancer Network Southampton & West Charlie Besley Northeast Charlotte Hutchings Portsmouth & Southeastern Meryl Deane Isle of Wight David Issacs Network Leadership/coordination Richard Roope

3
Objectives 2012-13 (QIPP friendly) Improving outcomes through awareness, early diagnosis and primary care Implementation RT strategy (IMRT) Tumour site pathway reviews and service development program Further develop systemic anti-cancer therapy strategy (AOS, AOT) Rollout of ERP Enhanced intelligence – staging data
 Improving outcomes through awareness, early diagnosis and primary care Implementation RT strategy (IMRT) Tumour site pathway reviews and service development program Further develop systemic anti-cancer therapy strategy (AOS, AOT) Rollout of ERP Enhanced intelligence – staging data")
4
CSCCN Renal Cancer Update Matthew Hayes Medical Director CSCCN Consultant Urological Surgeon UHS

6
How to get from this…

7
…to this?

8
How big is the problem? Kidney cancer is the sixth most common cancer among men in the UK (2009), accounting for more than 3% of all new cases of cancer in males. It is the ninth most common cancer among women in the UK (2009), responsible for more than 2% of all new cases of cancer in females. In 2009, there were 9,286 new cases of kidney cancer in the UK 5,706 (61%) in men and 3,580 (39%) in women, giving a male:female ratio of 16:10. 1 new case per GP every 4 years (41000 GPs in UK) 4000 UK deaths per annum
, accounting for more than 3% of all new cases of cancer in males. It is the ninth most common cancer among women in the UK (2009), responsible for more than 2% of all new cases of cancer in females. In 2009, there were 9,286 new cases of kidney cancer in the UK 5,706 (61%) in men and 3,580 (39%) in women, giving a male:female ratio of 16:10. 1 new case per GP every 4 years (41000 GPs in UK) 4000 UK deaths per annum.")
9
How big is the problem?

10
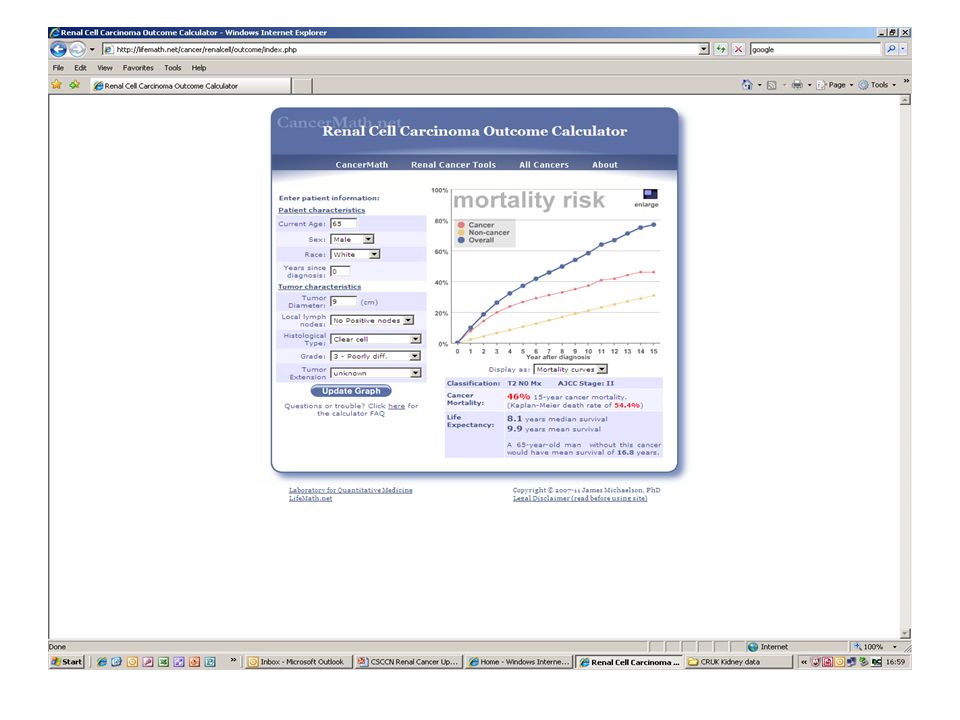
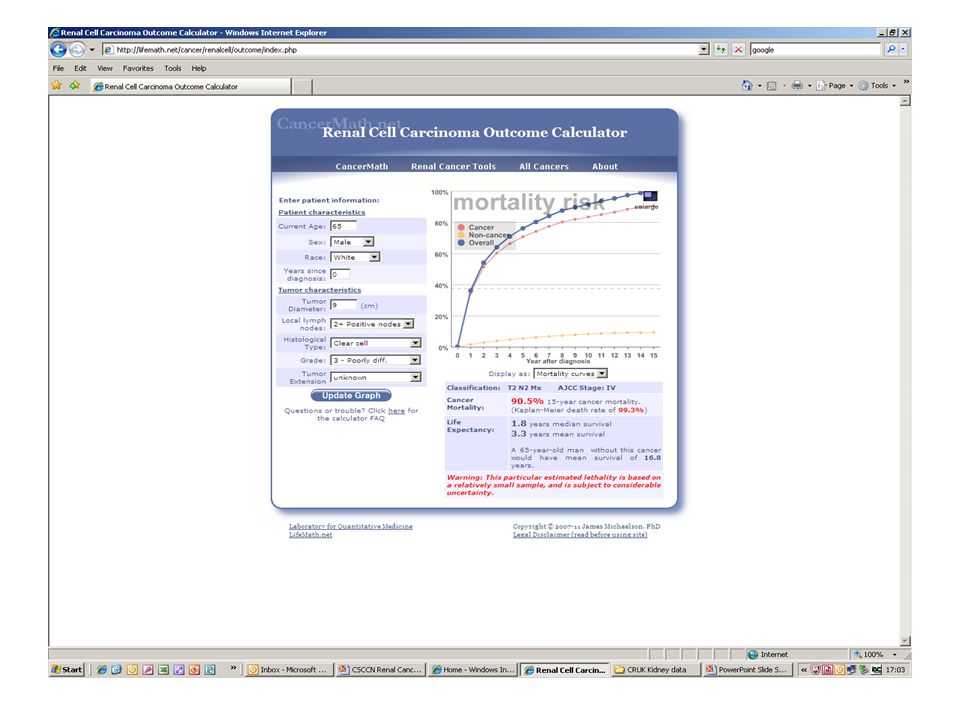
CRUK survival data

11
Survival

14
Curative treatment options Nephron sparing always where possible Ablation (percutaneous, cryo/RFA) Excision (partial vs radical nephrectomy) Laparoscopic vs open (robotic?) ERP, reduced LOS, reduced cost, reduced morbidity
 Excision (partial vs radical nephrectomy) Laparoscopic vs open (robotic ) ERP, reduced LOS, reduced cost, reduced morbidity")
15
How could outcomes be improved? Prevention - smoking, obesity (25%), alcohol Educational initiatives Early detection Earlier definitive treatment
, alcohol Educational initiatives Early detection Earlier definitive treatment.")
16
How could GPs improve early diagnosis? Haematuria 2WW referrals (visible and invisible) US screening - VHL, Birt-Hogg-Dube, tuberose sclerosis, hereditary renal cancer family history x2 risk, hepatitis C infection x2 risk, dialysis
 US screening - VHL, Birt-Hogg-Dube, tuberose sclerosis, hereditary renal cancer family history x2 risk, hepatitis C infection x2 risk, dialysis.")
17
What are the presenting symptoms and signs? Haematuria Loin pain (late) Weight loss and malaise Night sweats Varicocoele (usu left) Anaemia Hypercalcaemia Hypertension
 Weight loss and malaise Night sweats Varicocoele (usu left) Anaemia Hypercalcaemia Hypertension.")
18
What are the appropriate GP investigations? Dipstick urinalysis (rpt) 2ww referral USS (only if rapid access available as 2ww) FBC, renal function, bone and liver function CSCCN urgent referral guidelines for suspected renal cancer (2 week rule) · Of any age with painless macroscopic haematuria · Aged 40 years and older who present with recurrent or persistent urinary tract infection associated with macroscopic haematuria · With an abdominal mass identified clinically or on imaging that is thought to arise from the urinary tract · Aged 50 years and older who present with unexplained microscopic haematuria on urine microscopy without infection
 2ww referral USS (only if rapid access available as 2ww) FBC, renal function, bone and liver function CSCCN urgent referral guidelines for suspected renal cancer (2 week rule) · Of any age with painless macroscopic haematuria · Aged 40 years and older who present with recurrent or persistent urinary tract infection associated with macroscopic haematuria · With an abdominal mass identified clinically or on imaging that is thought to arise from the urinary tract · Aged 50 years and older who present with unexplained microscopic haematuria on urine microscopy without infection.")
19
Further information Kidney Cancer UK Secure Hold Business Centre, Studley Road, Redditch, Worc. B98 7LG Tel: 0844 870 7054 Web: www.kcuk.org Provides information and support to kidney cancer patients and their carers.www.kcuk.org Macmillan Cancer Support 3 Bath Place, Rivington Street, London, EC2A 3JR Tel: 0808 800 1234 Web: www.macmillan.org.uk Provides information and support to anyone affected by cancer.www.macmillan.org.uk CancerHelp UK Web: http://cancerhelp.cancerresearchuk.org/ provides facts about cancer, including treatment choices.http://cancerhelp.cancerresearchuk.org/

20
Over to you? What action plan does a practice need to put in place to change the outcomes for this particular cancer?

Similar presentations






Fabian Lee, Foundation Year 2. (2) Gbolahan.>")









 Public Health.>")



