Download presentation
Presentation is loading. Please wait.

1
Adrenal Cortex Adrenal Gland -II

2
At the end of the lecture, students should be able to: Describe the mechanisms of action of glucocorticoid and aldosterone. Describe physiological functions & regulation of mineralocorticoid secretion. Describe physiologic actions of Glucocorticoid and their role during injury. Describe and integrate the interactions of adrenal medullary and cortical hormones in response to stress. Describe the main features of the diseases caused by excess or deficiency of cortisol and aldosterone Learning Outcomes

3
1. Cortisol first interact with intracellular receptors in target cells. 2. diffuse through the cell membrane & binds with its protein receptor in the cytoplasm, 3. Cortisol -receptor complex then interacts with specific regulatory DNA sequences, called glucocorticoid response elements, to induce or repress gene transcription. 4. Increase or decrease transcription of many genes --- alter synthesis of mRNA for the proteins that mediate their multiple physiologic effects. Mechanism of Action of Glucocorticoids

5
Mechanism of Action of Aldosterone 1. Aldosterone diffuses readily to the interior of the tubular epithelial cells 2. combines with cytoplasmic receptor protein. 3. Aldosterone -receptor complex diffuses into the nucleus, 4. Undergo alterations & induce specific portions of the DNA to form types of m RNA related to the process of Na+ and K+ transport. 5. mRNA diffuses back into the cytoplasm to form protein with ribosomes. 6. Proteins formed are a mixture of (1) one or more enzymes and (2) membrane transport proteins, all acting together, for sodium, potassium, and hydrogen transport through the cell membrane.
 one or more enzymes and (2) membrane transport proteins, all acting together, for sodium, potassium, and hydrogen transport through the cell membrane..")
6
Mechanism of Action of Aldosterone

7
Physiological function of Aldosterone increases tubular reabsorption of sodium and excretion of potassium ~ conserve the Na+ in ECF and excretes K+ in Urine. total lack of aldosterone causes loss of 20 g Na + / day. Increased secretion of aldosterone hypokalemia – decrease from 4.5 mmol/l (norm) to 1 - 2 mmol/l (muscle weakness) alkalosis (increased excretion of H + ) Decreased secretion of aldosterone increase plasma K + 60 - 100% above normal level - hyperkalemia (cardiac toxicity) acidosis (decreased excretion of H + )
 to mmol/l (muscle weakness) alkalosis (increased excretion of H + ) Decreased secretion of aldosterone increase plasma K % above normal level - hyperkalemia (cardiac toxicity) acidosis (decreased excretion of H + ).")
8
2) on extracellular fluid volume increase of ECF - absorption of Na + is followed by osmotic absorption of water, therefore Na + concentration in ECF is not changed 3) on blood pressure increase in ECF volume leads to an increase in arterial pressure 4) on sweat glands, salivary glands, intestinal increase absorption of sodium Physiological function of Aldosterone
 on extracellular fluid volume increase of ECF - absorption of Na + is followed by osmotic absorption of water, therefore Na + concentration in ECF is not changed 3) on blood pressure increase in ECF volume leads to an increase in arterial pressure 4) on sweat glands, salivary glands, intestinal increase absorption of sodium Physiological function of Aldosterone")
9
aldosterone secretion and regulation of BP, Blood volume, & electrolyte

10
Regulation of aldosterone secretion Four factors are known to play essential roles in the regulation of aldosterone. Increased potassium ion concentration in the extracellular fluid greatly increases aldosterone secretion. Increased activity of the renin-angiotensin system (increased levels of angiotensin II) also greatly increases aldosterone secretion. Increased sodium ion concentration in the extracellular fluid very slightly decreases aldosterone secretion. ACTH from the anterior pituitary gland is necessary for aldosterone secretion but has little effect in controlling the rate of secretion.
 also greatly increases aldosterone secretion. Increased sodium ion concentration in the extracellular fluid very slightly decreases aldosterone secretion. ACTH from the anterior pituitary gland is necessary for aldosterone secretion but has little effect in controlling the rate of secretion..")
11
Excess of hormones of Mineralocorticoids Mineralocorticoids – Conn’s syndrome hypokalemia – muscle weakness hypervolumia – hypertension alkalosis – increased neuromuscular excitability

12
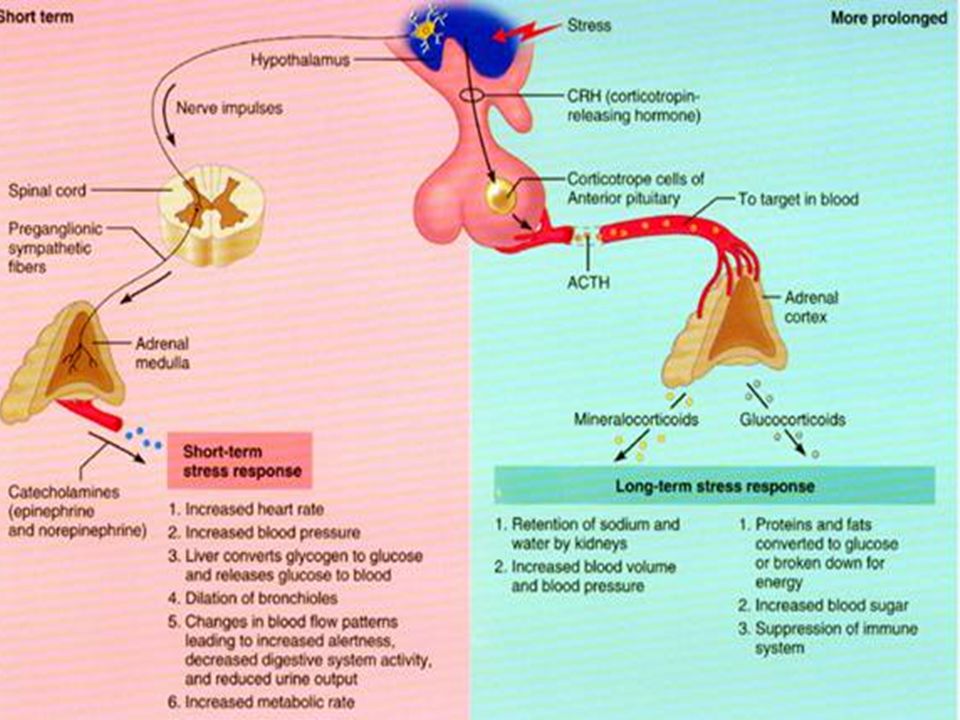
Lack of hormones of adrenal cortex Glucocorticoides and mineralocorticoides – Addison’s dissease consequences of lack of aldosterone decreased Na + reabsorption, decreased ECF volume hypercalemia, mild acidosis rise of hematocrit – decrease of cardiac output consequences of lack of cortisol depressed gluconeogenesis reduced fat and protein metabolism high level of ACTH - pigmentation Addisonian crisis - during stress (trauma, surgical operations) – extra need for glucocorticoids
 – extra need for glucocorticoids")
13
Physiologic actions of Glucocorticoid

14
Cortisol Increased lipolysis in fat cells Increased mobilisation of glycerol and fatty acids Increased gluconeogenesis, glycogenesis, glycogen storage and enzyme activity (e.g. glucose- 6-phosphate) in the liver Increased mobilisation of amino acids in skeletal tissue and muscles Stress response – maintenance of vascular tone Immunosuppressive and anti-inflammatory actions Physiologic actions of Glucocorticoid
 in the liver Increased mobilisation of amino acids in skeletal tissue and muscles Stress response – maintenance of vascular tone Immunosuppressive and anti-inflammatory actions Physiologic actions of Glucocorticoid.")
15
Action on Carbohydrate Metabolism stimulation of gluconeogenesis by the liver (rate increases 6 to 10 fold) enzymes required to convert amino acids into glucose are increased (activation of DNA transcription) mobilization of amino acids from extra- hepatal tissues (muscles) increase in glycogen storage in liver cells Decreased glucose utilization by the cells
 enzymes required to convert amino acids into glucose are increased (activation of DNA transcription) mobilization of amino acids from extra- hepatal tissues (muscles) increase in glycogen storage in liver cells Decreased glucose utilization by the cells")
16
mobilization of amino acids from non-hepatic tissues proteokatabolic effect in all body cells except of the liver decreased protein synthesis decreased amino acids transport into extrahepatic tissues (muscles, lymphatic tissues) Proteoanabolic effect in the liver enhanced liver proteins increased plasma proteins Action on protein metabolism
 Proteoanabolic effect in the liver enhanced liver proteins increased plasma proteins Action on protein metabolism")
17
Mobilization of fatty acids from adipose tissue Moderately enhance the oxidation of fatty acids (lower glucose utilization stimulates the cells to utilize energy from fatty acids ) Action on Lipid Metabolism
 Action on Lipid Metabolism")
18
Anti -inflammatory Action Release from damage tissues: proteolytic enzyme, histamine, bradykinin cortisol stabilizes lysosomal membrane increase the blood flow in inflamed area - vasodilatation cortisol reduces degree of vasodilatation leakage of plasma into damage area - clotting cortisol decreases permeability of capillaries, prevents loss of plasma infiltration by leukocytes cortisol decreases migration of white blood cells suppresses immune system: reduction of T- lymphocyte

19
1. Most of the proteolytic enzymes released by damaged cells to cause inflammation, are released in greatly decreased quantity by stabilizing the lysosomal membrane. 2. Decreases the permeability of the capillaries & prevents loss of plasma into the tissues. 3. Decreases both migration of white blood cells into the inflamed area and phagocytosis of the damaged cells by diminishes the formation of prostaglandins and leukotrienes Anti -inflammatory Role

20
Suppresses the immune system, causing lymphocyte reproduction to decrease markedly. Attenuates Attenuates fever mainly because it reduces the release of interleukin-1 from the WBCs. Causes Resolution of Inflammation by increasing rate of healing. Anti -inflammatory Role

21
Regulation of Cortisol Secretion

22
lower part of the hypothalamus connected to the anterior pituitary by the pituitary stalk or infundibulum. neurones There are many populations of neurones in the hypothalamus, some of which terminate close to the blood capillaries in the hypothalamus, but there is NO direct neural connection between the hypothalamus and the anterior pituitary gland. A network of blood capillaries in the hypothalamus drain into larger portal blood vessels, which link the hypothalamus to the anterior pituitary. Connections between the hypothalamus and the anterior pituitary gland

23
Let’s now look at how the hypothalamic and anterior pituitary hormones control the secretion of glucocorticoids….

24
ACTH adrenal cortex Corticotrophin releasing hormone (CRH) from the hypothalamus stimulates the anterior pituitary gland to secrete adrenocorticotrophic hormone (ACTH). CRH Hypothalamus Anterior pituitary + AVP ACTH

25
Secretion of cortisol is controlled entirely by ACTH secreted by the anterior pituitary gland. Also enhances the production of adrenal androgens. adrenal cortex CRH Hypothalamus Anterior pituitary Cortisol ACTH

26
10/2/2016 ACTH adrenal cortex ACTH also stimulates secretion of adrenal androgens (mainly androstenedione and dehydroepiandrosterone (DHEA)). ACTH only plays a minor part in stimulating secretion of mineralocorticoids (e.g. aldosterone). Hypothalamus Anterior pituitary Androgens (Aldosterone) CRH Aldosterone secretion is stimulated mainly by angiotensin II and increased plasma potassium levels. Cortisol
. Hypothalamus Anterior pituitary Androgens (Aldosterone) CRH Aldosterone secretion is stimulated mainly by angiotensin II and increased plasma potassium levels. Cortisol.")
27
ACTH adrenal cortex CRH Hypothalamus Anterior pituitary Cortisol has a negative feedback effect mainly on the anterior pituitary and to a lesser extent on the hypothalamus. High levels of cortisol suppress ACTH secretion as well as CRH secretion by the hypothalamus. Cortisol ACTH The third important control mechanism of ACTH and cortisol secretion is by negative feedback effects. Cortisol

28
So adrenal cortex hormone secretion is controlled by ACTH from the anterior pituitary. A primary control of ACTH secretion is by the circadian or diurnal rhythm of daylight and darkness…. But how ACTH secretion is controlled?

29
Clock time Cortisol (n moles/L) Light Dark Both ACTH and cortisol secretion show a circadian rhythm (diurnal rhythm). Cortisol secretion is low at night Cortisol levels fall at night as a direct result of a fall in ACTH levels. Cortisol secretion is lowest around midnight. Cortisol levels begin to rise between 1 and 4 am as a result of rising ACTH levels. This leads to a peak in cortisol secretion in the early morning. Cortisol secretion peaks early in the morning

30
The circadian rhythm of ACTH and cortisol secretion is controlled by the light/dark cycle. adrenal cortex Anterior pituitary ACTH Hypothalamus Suprachiasmatic nuclei Information about the light/dark cycle is conveyed via the retina of the eye to the paired suprachiasmatic nuclei in the hypothalamus.

31
ACTH adrenal cortex Anterior pituitary Hypothalamus Suprachiasmatic nuclei The light/dark cycle has overlying control of ACTH secretion. The circadian rhythms of individuals can vary considerably, although the circadian rhythm in the same individual can be quite consistent.

32
ACTH adrenal cortex Anterior pituitary Hypothalamus Suprachiasmatic nuclei The rhythm of cortisol secretion is therefore affected by changes in the light/dark cycle. 1. Stress 2. Negative feedback controls 3. Depression 4. Old age 5. Food 6. Weight are all able to alter the rhythm of cortisol secretion. But it is also influenced by other factors: Cortisol

34
ACTH then stimulates cortisol secretion (stress also causes secretion of adrenaline and noradrenaline from the adrenal medulla). Stress is a very important stimulus for ACTH secretion. A stressful stimulus initially causes an increase in CRH secretion from the hypothalamus. Hypothalamus Pituitar y STRESS ! adrenal cortex CRH + Cortisol CRH stimulates increased ACTH secretion by the anterior pituitary. + ACTH CRH ACTH Cortisol

35
Cortisol attenuates the responses of immune and inflammatory cells to stress (such as injury and infection), which might otherwise threaten survival. Cortisol has widespread actions in the body, which together restore homeostasis after stress. Hypothalamus Pituitary STRESS ! adrenal cortex CRH + Cortisol Cortisol acts as a physiological antagonist to insulin by promoting the breakdown of carbohydrates, lipids and protein (thus mobilising energy reserves.) + ACTH CRH ACTH
 + ACTH CRH ACTH.")
36
But prolonged stress causes continued cortisol secretion, which can result in muscle wastage, immune and inflammatory responses and hyperglycaemia. Hypothalamus Pituitary STRESS ! adrenal cortex CRH + Cortisol + ACTH Similar problems can occur after long-term treatment with glucocorticoid drugs.

39
Cortisol is essential for life! (bilateral adrenalectomy causes death within days). It is important both in maintaining the body’s metabolic balance and it’s response to stress.

40
Many of these physiological effects of glucocorticoids can be seen clearly in a condition called Cushing’s Syndrome. People suffering from Cushing’s Syndrome have an overproduction of glucocorticoids. What causes the overproduction of hormones seen in Cushing's syndrome? This can be due to a number of problems: e.g. An overproduction of ACTH and other peptides by the pituitary gland (often due to an adenoma), which stimulates the adrenal cortex to produce corticosteroids. Certain lung cancers and other tumours outside the pituitary gland may produce ACTH. Other causes include benign or cancerous tumours on the adrenal glands. The overproduction of glucocorticoids, which occurs in Cushing’s Syndrom, causes a variety of symptoms.
, which stimulates the adrenal cortex to produce corticosteroids. Certain lung cancers and other tumours outside the pituitary gland may produce ACTH. Other causes include benign or cancerous tumours on the adrenal glands. The overproduction of glucocorticoids, which occurs in Cushing’s Syndrom, causes a variety of symptoms..")
41
The most common sign of hypercortisolism is centripetal obesity, particularly across the shoulders and around the middle - due to increased fat metabolism Skeletal muscle wasting and weakness (thin arms and legs) can be so severe that the patient cannot stand up from a squatting position - due to increased protein metabolism Bruising and slow wound healing - due to collagen breakdown and a suppressed immune system Stretch marks (striae) - due to effects on connective tissues and increased fat metabolism A round ‘moon-face’ is also a sign of increased fat deposition Mild facial hirsutism is often seen in women as well as oily skin and acne - due to excess adrenal androgens
 can be so severe that the patient cannot stand up from a squatting position - due to increased protein metabolism Bruising and slow wound healing - due to collagen breakdown and a suppressed immune system Stretch marks (striae) - due to effects on connective tissues and increased fat metabolism A round ‘moon-face’ is also a sign of increased fat deposition Mild facial hirsutism is often seen in women as well as oily skin and acne - due to excess adrenal androgens")
42
Other effects of hypercortisolism, which are also symptoms of Cushing’s Syndrome, are not visible externally: Diabetes (may occur) - high blood sugar due to changed glucose metabolism Infections - suppression of the immune system by decreasing peripheral lymphocytes, inhibiting neutrophil accumulation and suppressing histamine and prostaglandin synthesis High blood pressure (hypertension) - due to salt and water retention and expansion of extracellular fluid volume Osteoporosis - increased calcium mobilisation from bone, inhibition of osteoblast function, enhanced osteoclast binding and decreased calcium absorption
 - high blood sugar due to changed glucose metabolism Infections - suppression of the immune system by decreasing peripheral lymphocytes, inhibiting neutrophil accumulation and suppressing histamine and prostaglandin synthesis High blood pressure (hypertension) - due to salt and water retention and expansion of extracellular fluid volume Osteoporosis - increased calcium mobilisation from bone, inhibition of osteoblast function, enhanced osteoclast binding and decreased calcium absorption")
Similar presentations













 Hormones are chemical.>")







