Download presentation
Presentation is loading. Please wait.

1
Chronic Myelocytic Leukemia Mark D. Browning, M.D. Oncology/Hematology Associates February 26, 2016

3
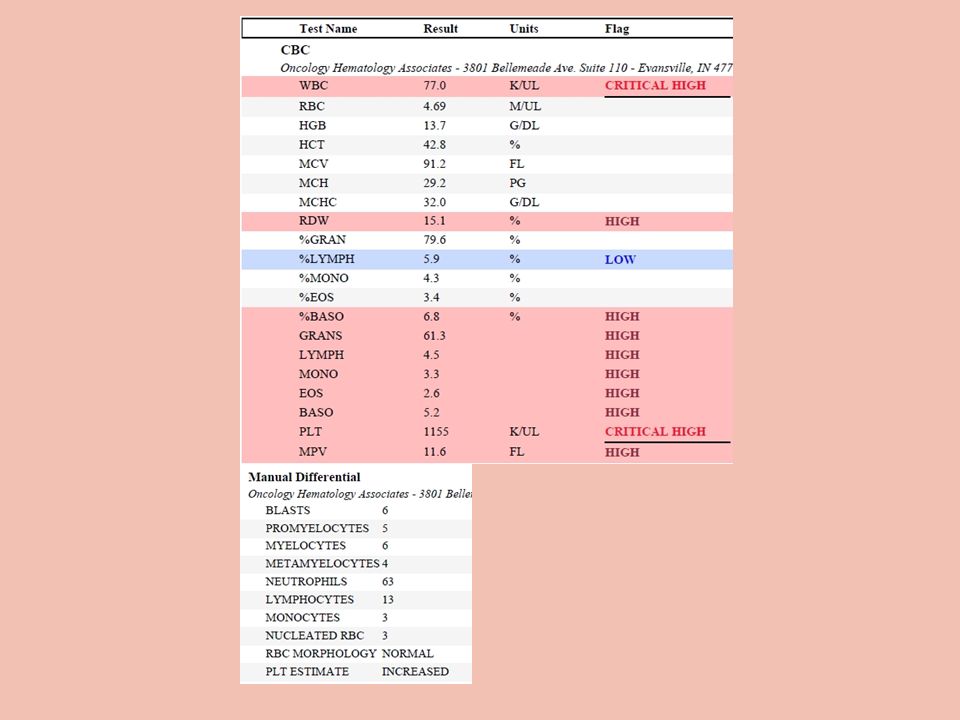
Case Study 43 yo male on routine PE by Internal Medicine Specialist noted to have WBC increased WBC 77,000, platelets 1.1 million, hgb 12.0 Immature WBCs noted in differential No fevers or recent infections No rheumatological problems 15 lb weight loss…intentional No history of cancer No Radiation Exposure

6
2 Bands and Metamyelocyte

7
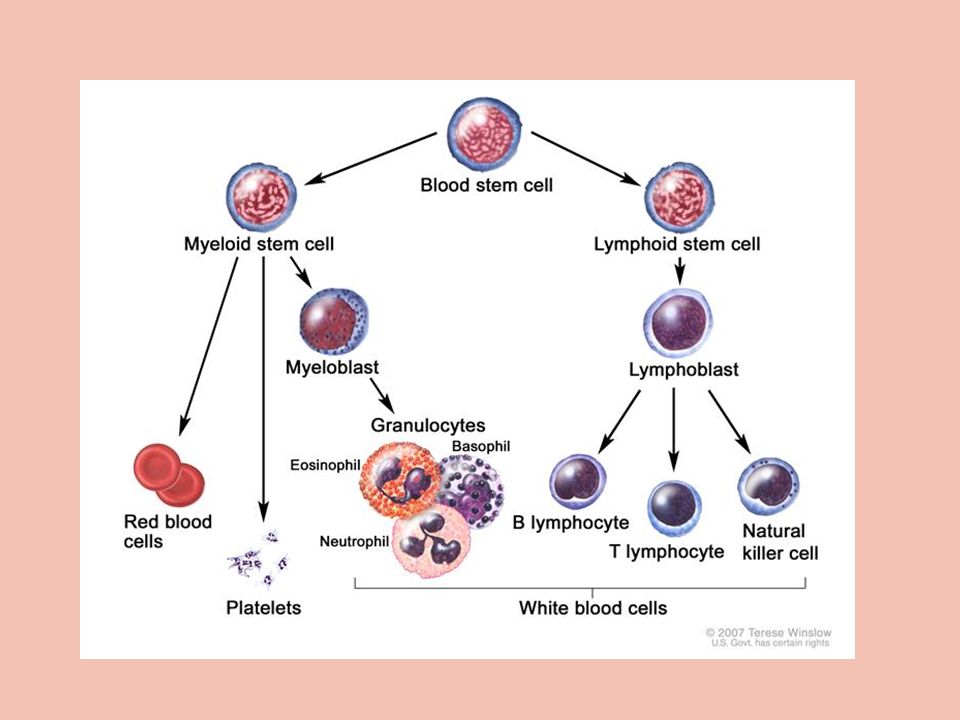
*Chronic Myelogenous Leukemia…Entire Spectrum of WBC Precursors

9
xxxxxxxx

10
*Chronic Myelogenous Leukemia (CML) Disease of middle age Peak incidence is in the 5 th decade of life Observed in younger & older individuals Philadelphia chromosome marker can be found in children & adults with acute leukemia It is a leukemia that may be induced by environmental factors (increased incidence in atomic bomb survivors)
 Disease of middle age Peak incidence is in the 5 th decade of life Observed in younger & older individuals Philadelphia chromosome marker can be found in children & adults with acute leukemia It is a leukemia that may be induced by environmental factors (increased incidence in atomic bomb survivors)")
11
CML…Background CML is a rare disorder of hematopoietic system Approximately 4,800 new cases were diagnosed in USA in 2009 Annual rate of 1 case per 100,000 people Median age at presentation is 53 years Typical symptoms are fatigue and weight loss About 40% of patients are asymptomatic

12
*Chronic Myelogenous Leukemia First detected on routine CBC Frequently no complaints Nonspecific complaints –Weight loss –Fatigue –Night sweats –Abdominal fullness –Episodes of abdominal pain –Bleeding & infection is not common

13
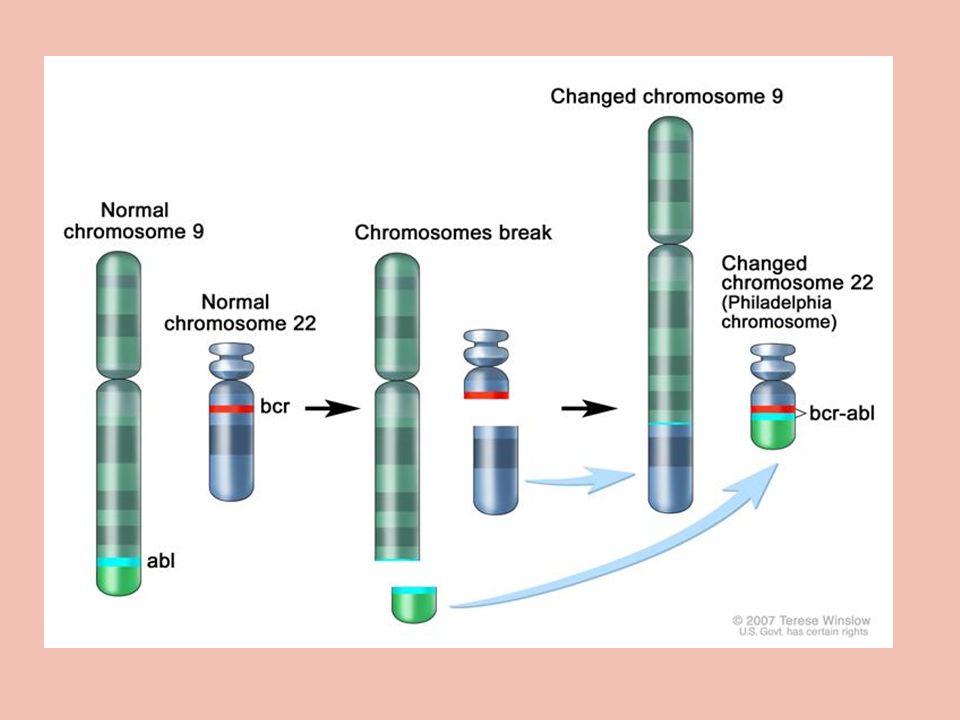
CML…Molecular Pathophysiology Diagnosis of CML based on detection of the Philadelphia (Ph+) chromosome(1962) –Translocation between chromosomes 9 and 22; referred to as t(9;22) Consequence of t(9;22) is the creation of the fusion protein, BCR-ABL The mutated BCR-ABL is a constitutively active tyrosine kinase, meaning it is always turned on.
 chromosome(1962) –Translocation between chromosomes 9 and 22; referred to as t(9;22) Consequence of t(9;22) is the creation of the fusion protein, BCR-ABL The mutated BCR-ABL is a constitutively active tyrosine kinase, meaning it is always turned on.")
14
*Philadelphia Chromosome…9/22

16
*9/22 Translocation…Philadelphia Chromosome

17
Cytogenetic Analysis “Gold standard” for diagnosis if associated with the correct clinical scenario t(9;22) is diagnostic for CML –Normal karyotype: 46,XX [20] –CML karyotype: t(9;22)(q34;q11)[20] Early detection of disease acceleration Labor intensive and time-consuming Insufficient sensitivity to monitor residual disease
![Cytogenetic Analysis Gold standard for diagnosis if associated with the correct clinical scenario t(9;22) is diagnostic for CML –Normal karyotype: 46,XX [20] –CML karyotype: t(9;22)(q34;q11)[20] Early detection of disease acceleration Labor intensive and time-consuming Insufficient sensitivity to monitor residual disease](http://images.slideplayer.com/42/11571078/slides/slide_17.jpg "Cytogenetic Analysis Gold standard for diagnosis if associated with the correct clinical scenario t(9;22) is diagnostic for CML –Normal karyotype: 46,XX [20] –CML karyotype: t(9;22)(q34;q11)[20] Early detection of disease acceleration Labor intensive and time-consuming Insufficient sensitivity to monitor residual disease")
18
Chronic Myelogenous Leukemia Physical Examination Splenomegaly is common <1/3 have hepatomegaly Left Upper Quadrant pain –Splenic infarction –Splenic friction rub Chloromas –Soft tissue leukemic infiltrates

19
Chronic Myelogenous Leukemia Laboratory * CBC usually points to the diagnosis 50,000 to 200,000/ul or higher Mature granulocytes but the entire spectrum of WBC precursors that circulate –Metamyelocytes, myelocytes, promyelocytes & blasts Loss of leukocyte alkaline phosphatase activity Sometimes Eosinophilia

20
*Entire Spectrum of WBC Precursors

21
CML…Laboratory Features

23
Chronic Myelogenous Leukemia Laboratory Studies* 9-22 chromosome translocation (Philadelphia chromosome) is the hallmark of CML 9-22 chromosome translocation is found in 10% of adult leukemias and 5 % of childhood ALL DNA probes show typical BCR-ABL translocation, whereas truly negative patients are probably RAEB
 is the hallmark of CML 9-22 chromosome translocation is found in 10% of adult leukemias and 5 % of childhood ALL DNA probes show typical BCR-ABL translocation, whereas truly negative patients are probably RAEB")
24
FISH NormalAbnormal

25
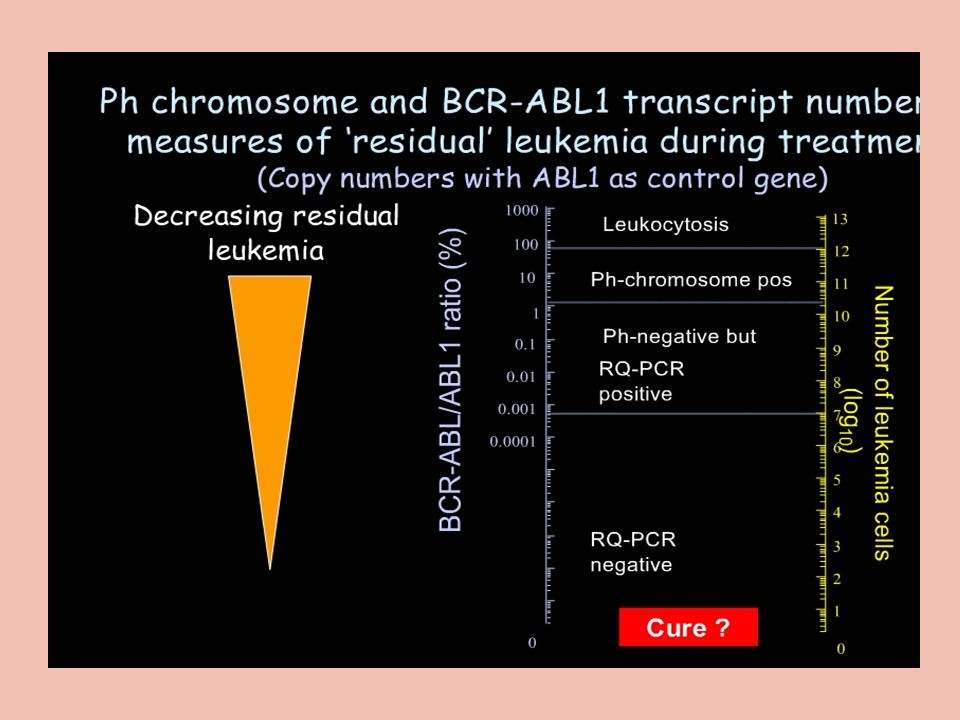
*PCR Molecular technique that can be used to produce millions of copies of a specific strand of DNA or RNA Qualitative PCR indicates that BCR-ABL is present or absent Quantitative PCR used to determine the amount of BCR-ABL and monitor progress

26
*Chronic Myelogenous Leukemia 3 Phases Chronic –<10% of cells in blood and marrow are blasts Accelerated Phase –10-19% of cells in blood and marrow are blasts Blastic Phase –>20% cells in blood and marrow are blasts –Fatigue, fever, enlarged speen and bone pain –Blast crisis

27
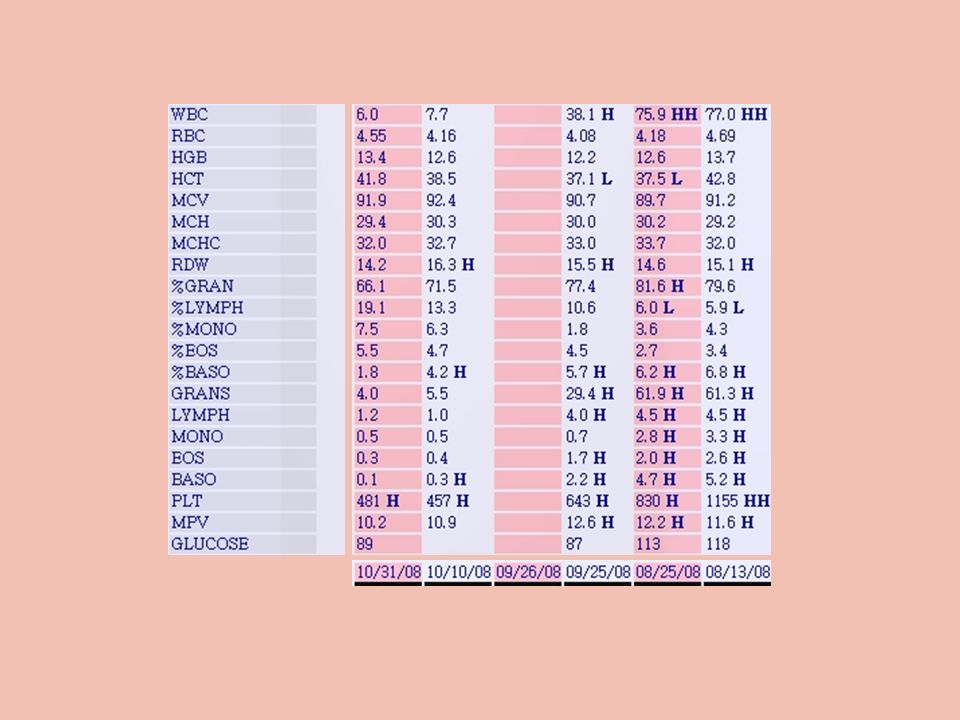
*CML Chronic Phase 3 years (before symptoms of accelerated phase) During chronic phase WBC can vary considerably but as the phase progresses, the WBCs & platelets are more difficult to control
 During chronic phase WBC can vary considerably but as the phase progresses, the WBCs & platelets are more difficult to control")
28
2 Bands and Metamyelocyte

29
*CML…Prognosis

31
*CML with Imatinib Therapy

32
*CML Accelerated Phase Lymphadenopathy Chloromas (nodular tumors of the skin) Widespread tissue infiltration of the WBCs Progressive fibrosis of the marrow Extramedullary hematopoiesis & tissue infiltrates
 Widespread tissue infiltration of the WBCs Progressive fibrosis of the marrow Extramedullary hematopoiesis & tissue infiltrates")
33
*CML Accelerated Phase # of Blasts in marrow & peripheral blood continue to increase < 1 year in accelerated phase, most patients evolve to an acute leukemia, referred to as blast crisis Once patient demonstrates other manifestations of leukemia … final phase occurs

34
*CML Blast Phase Worsening anemia Thrombocytopenia Loss of granulocytes to place patient at risk for infection Bone pain Poor performance status

35
CML Blast Phase 70+% terminal leukemia involves the myeloid lineage 30% involve the lymphoid lineage Phenotype the blasts to characterize their lineage Chromosomal studies show persistence of Ph chromosome but other chromosome abnormalities appear & indicates advancing stage

37
CML -- Therapy…Chronic Phase Imatinib mesylate (Gleevec) XXX (1 st gen) Dasatinib (Sprycel)(2 nd gen) Nilotinib (Tasigna)(2 nd gen) Bosutinib…(2 nd gen) XXX major change noted in late 1990s Hydroxyurea Interferon alpha Transplant Chemotherapy
 XXX (1 st gen) Dasatinib (Sprycel)(2 nd gen) Nilotinib (Tasigna)(2 nd gen) Bosutinib…(2 nd gen) XXX major change noted in late 1990s Hydroxyurea Interferon alpha Transplant Chemotherapy")
40
*What Does Response Mean? Complete hematologic response(CHR) –Complete normalization of peripheral blood counts with leukocyte count <10 109/L –Platelet count <450 109/L –No immature cells in peripheral blood –No signs and symptoms of disease with disappearance of palpable splenomegaly
 –Complete normalization of peripheral blood counts with leukocyte count <10 109/L –Platelet count <450 109/L –No immature cells in peripheral blood –No signs and symptoms of disease with disappearance of palpable splenomegaly.")
41
*What Does Response Mean? Partial hematologic response is same as complete HR except for (PHR) –Presence of immature cells –Platelet count 450 109/L –Persistent splenomegaly, but <50% of the pretreatment extent Cytogenetic response(CCR,PCR,MCR) –Complete: No Ph+ metaphases –Partial: 1% to 34% Ph+ metaphases –Minor: 35% to 90% Ph+ metaphases
 –Presence of immature cells –Platelet count 450 109/L –Persistent splenomegaly, but <50% of the pretreatment extent Cytogenetic response(CCR,PCR,MCR) –Complete: No Ph+ metaphases –Partial: 1% to 34% Ph+ metaphases –Minor: 35% to 90% Ph+ metaphases.")
42
*Response to Imatinib (Gleevec) CHRONIC PHASE –79% complete cytogenetic response (CCR) in newly diagnosed patients –90% CCR with high-dose treatment (800 mg); –63% molecular response rate (MRR) ACCELERATED PHASE –Hematologic response (HR) in 80% of patients in the accelerated phase –Major cytogenetic response in 24% of patients –Complete HR in 30% of patients in blast crisis
 CHRONIC PHASE –79% complete cytogenetic response (CCR) in newly diagnosed patients –90% CCR with high-dose treatment (800 mg); –63% molecular response rate (MRR) ACCELERATED PHASE –Hematologic response (HR) in 80% of patients in the accelerated phase –Major cytogenetic response in 24% of patients –Complete HR in 30% of patients in blast crisis")
43
Cytogenetic Response

44
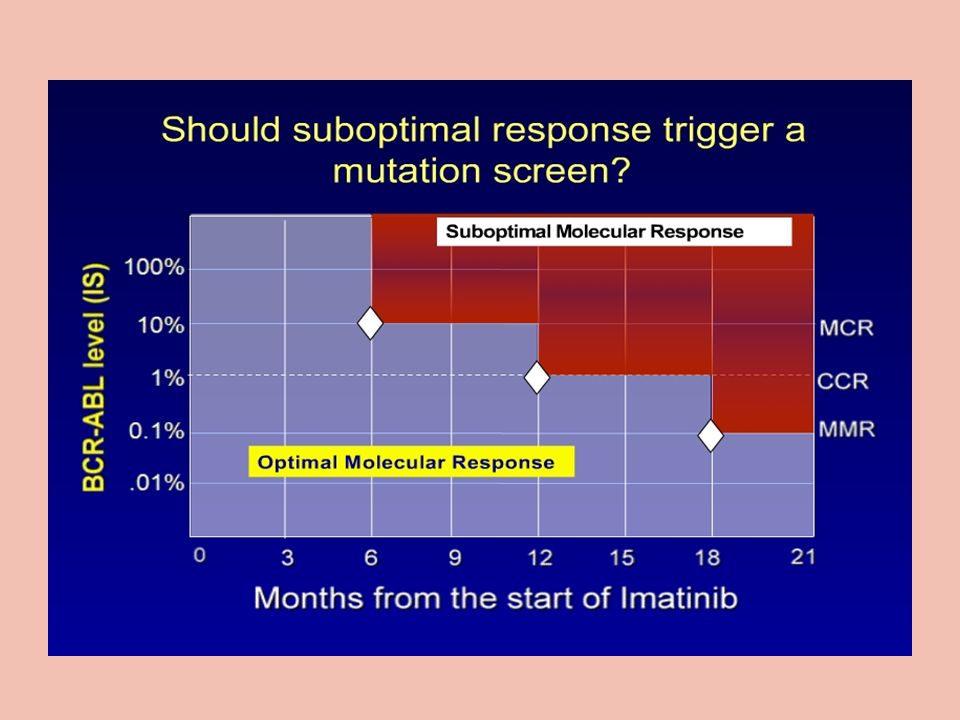
Imatinib (Gleevec) Resistance Failure to achieve a complete hematologic response in 3 to 6 months of Imatinib Rx Failure to achieve a major cytogenetic response by month 12 Progression of disease after previous cytogenetic or hematologic response
 Resistance Failure to achieve a complete hematologic response in 3 to 6 months of Imatinib Rx Failure to achieve a major cytogenetic response by month 12 Progression of disease after previous cytogenetic or hematologic response")
46
Fertility with Imatinib

47
Re-Challenge…Imatinib

48
CML Therapy in 2016

49
Chronic Myelocytic Leukemia Tyrosine Kinase Inhibitors

Similar presentations




1 CHILDHOOD LEUKAEMIA. TA OGUNLESI (FWACP)2 LEUKAEMIA Heterogenous group of malignant disorders Characterised by uncontrolled clonal.>")











:>")
 leukemia Is characterized by an unregulated proliferation of myeloid elements in the bone marrow,>")




