Download presentation
Presentation is loading. Please wait.

3
Objectives At the end of this lecture the student should be able to Name the common disorders of pulmonary circulation (embolism, vasculitis, alveolar haemorrhage and pulmonary hypertension). Describe pulmonary embolism (PE) and discuss it as follows: o Definition. o Substances other than thrombus that can embolize into the pulmonary circulation. o Pathogenesis and risk factors. Compare and contrast the clinical features of: o Small/medium pulmonary embolism. o Massive pulmonary embolism. o Multiple, recurrent pulmonary emboli. Clinical prediction score. List the usual laboratory and radiological investigations
 and discuss it as follows: o Definition. o Substances other than thrombus that can embolize into the pulmonary circulation. o Pathogenesis and risk factors. Compare and contrast the clinical features of: o Small/medium pulmonary embolism. o Massive pulmonary embolism. o Multiple, recurrent pulmonary emboli. Clinical prediction score. List the usual laboratory and radiological investigations.")
4
Normal Pulmonary Circulation

5
Pulmonary Circulation disorders Diseases that might affect pulmonary vasculature may include: Autimmune diseases ( vasculitides, anti-basement membrane antibodies) Infection (schistosomaisis) Congenital Neoplastic (hemangiomas) Pulmonary embolism Pulmonary hypertension
 Infection (schistosomaisis) Congenital Neoplastic (hemangiomas) Pulmonary embolism Pulmonary hypertension")
6
Pulmonary embolism Definition: Abrupt blockage of a pulmonary artery or one of its branches – most commonly = embolus from deep veins of the lower limbs Pulmonary embolism + DVT = venous thromboembolism VTE Stasis Hyper coagulobility Endothelial injury

7
Epidemiology 300.000-650,00 patients each year Annual incidence of VTE is 1in 1000 persons. Incidence increases with age Male = female (recurrent VTE commoner in males) - US data
 - US data.")
8
Causes and Risk Factors Prothrombotic factors Virchow triad Antithrombotic factors

9
Causes and Risk Factors Should be considered in history Hereditary factors Deficiency of natural anticoagulants (ATIII, protein C & S Resistant to inhibitors factor V Leiden Increased coagulation factors e. g VIII, XI etc Defect in fibrinolytic pathway dysfirinogenemia Acquired factors Immobilization Major surgery/ trauma Central venous catheter Obesity Malignancy Pregnancy Advanced age Medical illness e.g. SLE mixed hyperhomocysteinemia Elevated level of Lpa Low level of TFP inhibitors

10
Causes and Risk Factors

11
Clinical Presentation Can be difficult to diagnose (no specific signs and symptoms). There are 3 clinical syndromes associated with pulmonary embolism: 1.Small/ Medium sized emboli 2.Large (massive) emboli 3.Recurrent small embli
 emboli 3.Recurrent small embli.")
12
Clinical Presentation 1-Small/ medium pulmonary embolism: (Embolus in terminal P vessel) Chest pain Breathlessness Haemoptysis O/E Tachypnoea Pleural rub Crackles Pleural effusion May be fever Cardiovascular examination is normal
 Chest pain Breathlessness Haemoptysis O/E Tachypnoea Pleural rub Crackles Pleural effusion May be fever Cardiovascular examination is normal")
13
Clinical Presentation 2-Massive pulmonary embolism (obstruction of R V outflow) Rare Sudden collapse Severe chest pain Shock (pale, sweaty) Syncope
 Rare Sudden collapse Severe chest pain Shock (pale, sweaty) Syncope")
14
Clinical Presentation O/E mainly cardiac signs Tachypnoea Tachycardia Hypotension Cyanosis Raised JVP prominent ‘a’ wave R. ventricular heave, gallop, widely splits2 The chest is usually clear

15
Clinical Presentation 3-Multiple recurrent pulmonary emboli: Increased breathlessness over weeks or months Weakness, syncope occasional angina (exertion) O/E (pulmonary hypertension) Right ventricular heave Loud P2
 O/E (pulmonary hypertension) Right ventricular heave Loud P2")
16
Clinical Presentation

17
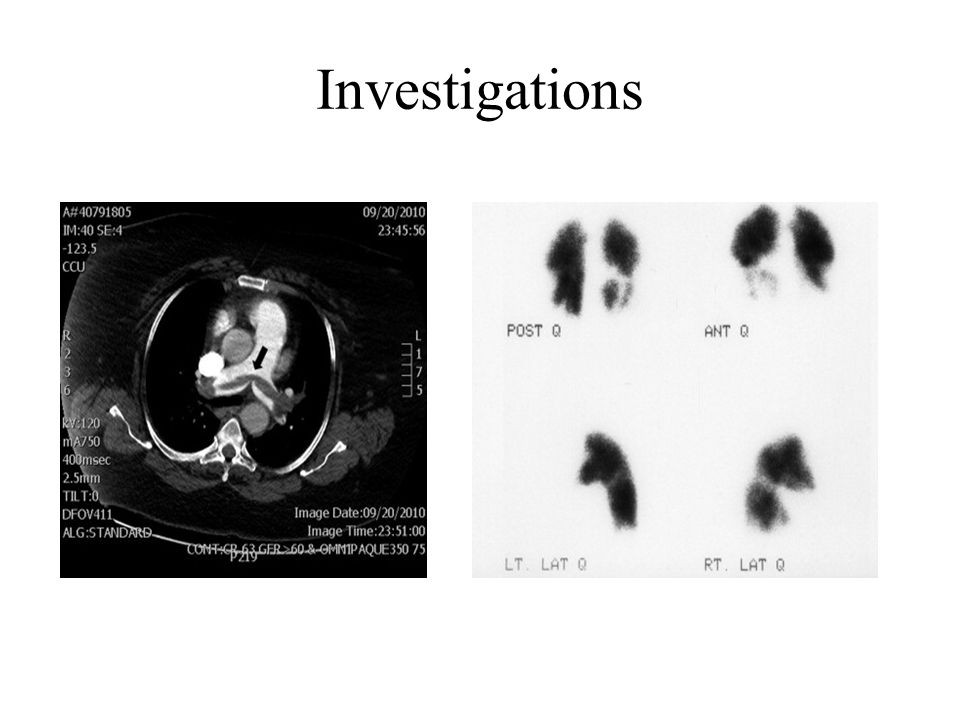
List of Investigations Non imaging tests: 1.Plasma D-dimers ( -ve result excludes diagnosis) 2.ECG (SI, QIII,TIII) Non invasive imaging tests: 1.Chest radiography 2.CT angiography (the BEST diagnostic test) 3.Ventilation / Perfusion scan ( -ve result excludes diagnosis) 4.Doppler ultrasonography 5.Echocardiography
 2.ECG (SI, QIII,TIII) Non invasive imaging tests: 1.Chest radiography 2.CT angiography (the BEST diagnostic test) 3.Ventilation / Perfusion scan ( -ve result excludes diagnosis) 4.Doppler ultrasonography 5.Echocardiography")
18
List of Investigations Invasive imaging tests 1.Pulmonary angiography 2.Contrast venography ABG: Low PCO2 Low PO2

19
Investigations

21
Diagnostic Approach 2-Clinical prediction score 3- Select appropriate test 1- Symptoms & signs suggestive of PE

22
Diagnostic Approach Clinical prediction score : I.Revised Geneva score II.Wells score Revised Geneva score: low risk 0- 3 Intermediate risk 4- 10 High risk >10

23
Diagnostic Approach Revised Geneva score Items of the Revised Geneva ScorePoints for Revised Version Age > 65 years old 1 Previous history of PE or DVT 3 Surgery or fracture within 1 month 2 Active malignancy 2. Unilateral leg pain 3 Hemoptysis 2. Heart rate (bpm) 75-94 3 ≥ 95 5 Pain on lower-limb deep venous palpation and unilateral oedema 4
 ≥ 95 5 Pain on lower-limb deep venous palpation and unilateral oedema 4.")
24
Diagnostic Approach

25
Differential Diagnosis Myocardial infarction Pericarditis Aortic dissection Pneumonia Pleurisy Chest wall pain Congestive heart failure

26
Treatment Treatment goals Stabilize the patient i.Oxygen for hypoxia ii.Analgesics for chest pain Prevent extension of current thrombus (short term) i.Parenteral anticoagulants – heparin ii.Oral anticoagulants - warfarin
 i.Parenteral anticoagulants – heparin ii.Oral anticoagulants - warfarin")
27
Treatment Prevent recurrent VTE (long term) i.Continue anticoagulation (warfarin) for 6 weeks- 6month- indefinitely ii.Life style changes iii.Graduated compression stockings iv.IVC Filter Lysis or removal of a thrombus in case of haemodynamic instability (massive PE): i.Thrombolytic therapy e. g. streptokinase ii.Pulmonary embolectomy

28
Prevention Avoid prolonged immobilization Smoking cessation Contraception (non hormonal) Obesity should be treated Thromboprophylaxis in high risk patient
 Obesity should be treated Thromboprophylaxis in high risk patient")
29
Other Rare Causes of Pulmonary Embolism Fat embolism (long bone fractures, acute pancreatitis) Air embolism (decompression sickness, iatrogenic) Amniotic fluid embolism (postpartum) Septic embolism (sepsis) Tumor embolism
 Air embolism (decompression sickness, iatrogenic) Amniotic fluid embolism (postpartum) Septic embolism (sepsis) Tumor embolism")
30
Summary Pulmonary embolism is usually caused by a thrombus in the deep proximal veins of the legs that breaks off and lodges in the lungs Patient may be a symptomatic or may present with typical symptoms including dyspnoea & chest pain. Massive pulmonary embolism may present with hypotension, shock or sudden death. An integrated diagnostic approach involving clinical prediction rules and non invasive testing can be used to evaluate patients. The aggressiveness of treatment is dependent on the severity of pulmonary embolism. Prevention of DVT in hospitalized patient is crucial to preventing embolism.

31
References Kumar & Clark’s Clinical Medicine 8 th edition /https://www.clinicalkey.com

Similar presentations







 around valves propagation Virchow’s triad.>")




 F.R.C.P. (E) F.R.C.P. (LONDON) F.A.C.C DESIGNED AT A.V. DEPT F.J.M.C.>")






