Download presentation
Presentation is loading. Please wait.

1
Intern Report Tony Hung Modified from presentation by Selim Krim, MD, Assistant Professor at TTUHSC

2
Case 1 A 62-year-old male presents to ER complaining of cough, fever, and difficulty breathing, which developed overnight. He has no symptoms of rhinorrhea, sore throat, or earache. He is not a smoker and has no history of asthma or recent antibiotic use. He is a business executive who travels extensively and just returned from Arizona.

3
Case 1 On physical examination, he appears flushed but otherwise alert and oriented. He is 5-11,180 lbs and has a blood pressure of 110/70 mmHg, a heart rate of 90 beats per minute, a respiratory rate of 24 breaths per minute, and a body temperature of 39 ºC. Lung sounds reveal a mild dullness in right base, no increased tympany, and coarse breath sounds with mild rales in right posterior lung base. He is not wheezing. The rest of his exam is normal.

4
Based on your history and physical exam what is your diagnosis?

6
Diagnosis of Pneumonia Signs and symptoms

7
Diagnosis of Pneumonia Signs and symptoms Subjective fever Cough with or without sputum Dyspnea Chest discomfort Sweats Rigors Fever/ hypothermia Tachypnea Tachycardia Increased tactile fremitus Dullness to percussion Decreased breath sound Presence of rales or crackles

8
Diagnosis of Pneumonia Signs and symptoms Subjective fever Cough with or without sputum Dyspnea Chest discomfort Sweats Rigors Fever/ hypothermia Tachypnea Tachycardia Increased tactile fremitus Dullness to percussion Decreased breath sound Presence of rales or crackles Overall, physician judgment is moderately accurate for diagnosis of pneumonia, especially for ruling it out (LR+ = 2.0, negative likelihood ratio [LR–] = 0.24)
![Diagnosis of Pneumonia Signs and symptoms Subjective fever Cough with or without sputum Dyspnea Chest discomfort Sweats Rigors Fever/ hypothermia Tachypnea Tachycardia Increased tactile fremitus Dullness to percussion Decreased breath sound Presence of rales or crackles Overall, physician judgment is moderately accurate for diagnosis of pneumonia, especially for ruling it out (LR+ = 2.0, negative likelihood ratio [LR–] = 0.24)](http://images.slideplayer.com/42/11324322/slides/slide_8.jpg "Diagnosis of Pneumonia Signs and symptoms Subjective fever Cough with or without sputum Dyspnea Chest discomfort Sweats Rigors Fever/ hypothermia Tachypnea Tachycardia Increased tactile fremitus Dullness to percussion Decreased breath sound Presence of rales or crackles Overall, physician judgment is moderately accurate for diagnosis of pneumonia, especially for ruling it out (LR+ = 2.0, negative likelihood ratio [LR–] = 0.24)")
9
Diagnosis of Pneumonia Signs and symptoms Subjective fever Cough with or without sputum Dyspnea Chest discomfort Sweats Rigors Fever/ hypothermia Tachypnea Tachycardia Increased tactile fremitus Dullness to percussion Decreased breath sound Presence of rales or crackles Atypical pneumonia??

10
Diagnosis of Pneumonia Signs and symptoms Subjective fever Cough with or without sputum Dyspnea Chest discomfort Sweats Rigors Fever/ hypothermia Tachypnea Tachycardia Increased tactile fremitus Dullness to percussion Decreased breath sound Presence of rales or crackles Atypical pneumonia Headaches (CNS symptoms) Diarrhea (GI symptoms) High fever Male sex Multli-lobar
 Diarrhea (GI symptoms) High fever Male sex Multli-lobar")
11
Diagnosis of Pneumonia Signs and symptoms Subjective fever Cough with or without sputum Dyspnea Chest discomfort Sweats Rigors Fever/ hypothermia Tachypnea Tachycardia Increased tactile fremitus Dullness to percussion Decreased breath sound Presence of rales or crackles What about older patient?? COPD?? HIV?? Recent Travel?? Cruise Ships?? Fall/Winter Season??

12
Epidemiology

13
MCQ Which of the following statements is true about community- acquired pneumonia? Pneumonia and influenza combined is the eighth leading cause of death in the United States and the most common cause of infection-related mortality Only 400 cases of community-acquired pneumonia (CAP) occur each year The estimated annual economic burden of CAP in the United States exceeds $17
 occur each year The estimated annual economic burden of CAP in the United States exceeds $17.")
14
MCQ Streptococcus pneumoniae is identified in up to what percentage of community-acquired pneumonia cases? 40% 60% 80%

15
Identified Pathogens in Community-acquired Pneumonia Pathogen Percentage Streptococcus pneumoniae 20-60% Haemophilus influenzae 3-10% Staphylococcus aureus 3-5% Gram-negative bacilli 3-10% Legionella species 2-8% Mycoplasma pneumoniae 1-6% Chlamydia pneumoniae 4-6% Viruses 2-15% Aspiration 6-10% Others 3-5%

16
MCQ What is the most likely pathogenic mechanism in this patient's pneumonia? Aspiration of oropharyngeal contents Hematogenous deposition Reactivation Inhalation of infectious particles

17
Pathogenetic mechanisms in Pneumonia Inhalation of infectious particles Common Aspiration of oropharyngeal or gastric content Common Hematogenous deposition Uncommon Invasion from infection in contiguous structures Rare Reactivation More common in Immunocompromised hosts

18
MCQ What is the next most important step in this patient's care? Empiric therapy with a fluoroquinolone Chest x-ray Sputum culture Hospitalization CBC, glucose, BUN, Na tests

19
An infiltrate on lung imaging, usually CXR, is required for the diagnosis of CAP; therefore, the test should be performed in patients with clinically suspected CAP

20
Extent of radiographic findings may help identify the severity of illness and assist with initial point-of-care decisions

23
Diagnostic tests Chest x-ray essential (AP and Lateral) – Lobar consolidation, cavitation, and pleural effusions suggest a bacterial etiology – Diffuse parenchymal involvement is more often associated with Legionella or viral pneumonia.
 – Lobar consolidation, cavitation, and pleural effusions suggest a bacterial etiology – Diffuse parenchymal involvement is more often associated with Legionella or viral pneumonia.")
24
Diagnostic tests

25
What about labs?

26
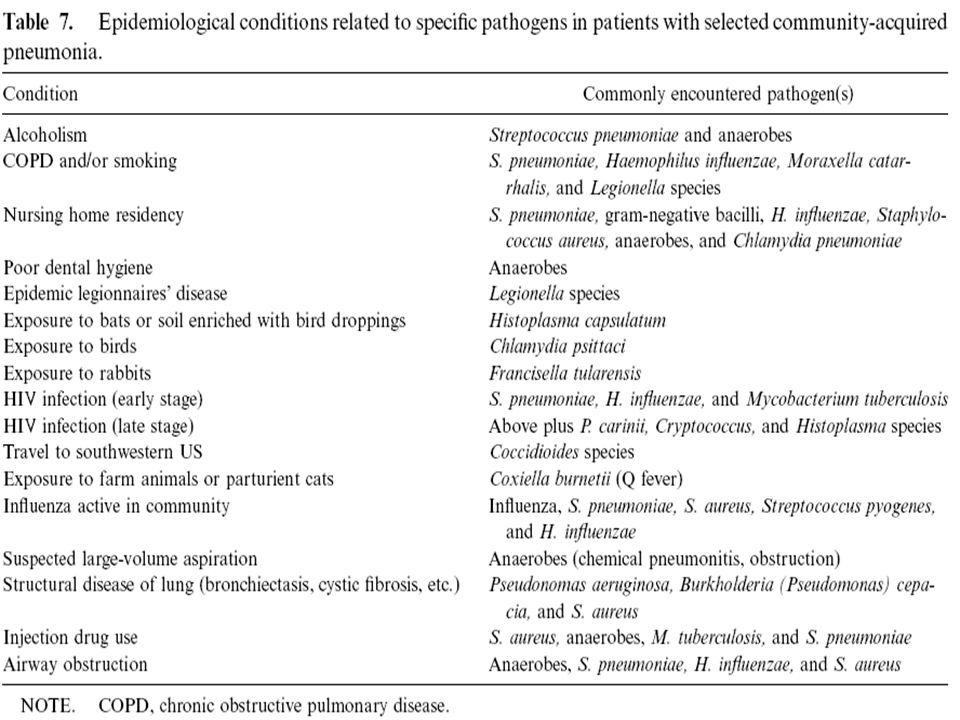
Routine laboratory testing to establish an etiology in outpatients with CAP is usually unnecessary HOWEVER evaluation for specific pathogens that would alter standard empiric therapy should be performed when the presence of such pathogens is suspected on the basis of clinical and epidemiologic clues

27
Hypoglycemia (blood glucose level less than 70 mg per dL [3.89 mmol per L]) at presentation is associated with increased 30-day mortality even after adjustment for other variables, including comorbid illness and Pneumonia Severity Index (PSI) score WBC? CRP? Pro-Calcitonin? Blood Cultures?
![Hypoglycemia (blood glucose level less than 70 mg per dL [3.89 mmol per L]) at presentation is associated with increased 30-day mortality even after adjustment for other variables, including comorbid illness and Pneumonia Severity Index (PSI) score WBC.](http://images.slideplayer.com/42/11324322/slides/slide_27.jpg "CRP. Pro-Calcitonin. Blood Cultures .")
28
Blood cultures are not recommended for most hospitalized patients with CAP Unless… severe CAP A study comparing 125 patients with CAP caused by pneumococcal bacteremia and 1,847 patients with nonbacteremic CAP found no increase in poor outcomes among those with bacteremia false-positive blood culture results have been associated with prolonged hospitalization and more vancomycin use

29
Adapted with permission from Mandell LA, Wunderink RG, Anzueto A, et al. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin Infect Dis. 2007;44(suppl 2):S40 Sputum culture?
:S40 Sputum culture .")
30
Adapted with permission from Mandell LA, Wunderink RG, Anzueto A, et al. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin Infect Dis. 2007;44(suppl 2):S40 Infectious Diseases Society of America/American Thoracic Society (IDSA/ATS) guidelines recommend that sputum specimens be obtained before the initiation of antibiotic therapy in inpatients.
:S40 Infectious Diseases Society of America/American Thoracic Society (IDSA/ATS) guidelines recommend that sputum specimens be obtained before the initiation of antibiotic therapy in inpatients..")
31
Adapted with permission from Mandell LA, Wunderink RG, Anzueto A, et al. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin Infect Dis. 2007;44(suppl 2):S40
:S40.")
32
Urine antigen tests are helpful when an adequate sputum culture is unobtainable or when antibiotic therapy has already been started. Urine antigen test only detects Legionella serogroup 1, is that a problem??

33
Adapted with permission from Mandell LA, Wunderink RG, Anzueto A, et al. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin Infect Dis. 2007;44(suppl 2):S40 Serogroup 1 causes 80 to 95 percent of CAP from Legionella; the test is 70 to 90 percent sensitive and 99 percent specific for serogroup 1. Urine antigen test results are positive on the first day of illness and remain positive for several weeks.
:S40 Serogroup 1 causes 80 to 95 percent of CAP from Legionella; the test is 70 to 90 percent sensitive and 99 percent specific for serogroup 1. Urine antigen test results are positive on the first day of illness and remain positive for several weeks..")
34
Adapted with permission from Mandell LA, Wunderink RG, Anzueto A, et al. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin Infect Dis. 2007;44(suppl 2):S40 The sensitivity of the pneumococcal urine antigen test is ??? with a specificity ???
:S40 The sensitivity of the pneumococcal urine antigen test is . with a specificity .")
35
Adapted with permission from Mandell LA, Wunderink RG, Anzueto A, et al. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin Infect Dis. 2007;44(suppl 2):S40 The sensitivity of the pneumococcal urine antigen test is ??? with a specificity ??? In general, urine antigen tests are better at ruling in disease when positive; a negative test result does not rule out infection with a specific pathogen given its somewhat limited sensitivity.
:S40 The sensitivity of the pneumococcal urine antigen test is . with a specificity . In general, urine antigen tests are better at ruling in disease when positive; a negative test result does not rule out infection with a specific pathogen given its somewhat limited sensitivity..")
36
Should this patient be admitted?

37
Case 1 A 62-year-old white male presents complaining of cough, fever, and difficulty breathing, which developed during the night. He has no symptoms of rhinorrhea, sore throat, or earache. He is not a smoker and has no history of asthma or recent antibiotic use. He is a business executive who travels extensively and just returned from California.

38
Case 1 On physical examination, he appears flushed but otherwise alert and oriented. He is 5-11,180 lbs and has a blood pressure of 110/70 mmHg, a heart rate of 90 beats per minute, a respiratory rate of 24 breaths per minute, and a body temperature of 39 ºC. Lung sounds reveal a mild dullness in right base, no increased tympany, and coarse breath sounds with mild rales in right posterior lung base. He is not wheezing. The rest of his exam is normal.

39
Management of CAP depends on the patient's severity of illness; underlying medical conditions and risk factors, such as smoking; and ability to adhere to a treatment plan.

40
British Thoracic Society

41
A SMART-COP score of 3 or more points identifies 92 percent of those who will receive intensive respiratory or vasopressor support

42
How would you treat this patient? What if he has … Chronic heart, lung, liver, renal disease. DM, etoh. Cancer. Asplenia. Antibiotics use in the past 3 month?

44
Case 1 (Part 2) Empiric therapy with an oral macrolide was prescribed, and the patient was sent home. Two days later, he presents at the emergency room with shaking chills and fever, increasingly productive cough, and difficulty breathing. His vital signs are as follow: BP 110/60 mmHg, body temperature 40.5° C, pulse rate 126 beats/min, and respiration rate 28 breaths/min. He is alert and oriented. His exam again reveals rales and dullness in the right lower posterior lung fields without wheezing. Chest x-ray shows a focal infiltrate in the right lower lung and a small pleural effusion.

45
Would you admit this patient now?

47
What is the typical duration of therapy?

48
Duration of therapy for patients with CAP has traditionally been 10 to 14 days, but more recent evidence suggests a shorter course of up to seven days is equally effective. Hospitalized patients may be switched from intravenous to oral antibiotic therapy after they have clinical improvement and are able to tolerate oral medications. An early switch from intravenous to oral antibiotics after three days in patients with severe CAP has been shown to be effective and may decrease length of hospital stay.

49
When would you consider discharging your patient?

50
Discharge Criteria Candidates for discharge should have no more than one of the following poor prognostic indicators: Temperature > 37.8 degrees Celsius Pulse > 100 beats per minute Respiratory rate > 24 per minute Systolic blood pressure < 90 mmHg Oxygen saturation < 90 percent Inability to maintain oral intake

52
Thank You

54
Key Points Community-acquired pneumonia can be treated empirically with oral antibiotics in the outpatient setting (in patients with low risk category) Patients younger than age 50 who have no comorbid health problems and who present with minimal signs and symptoms of possible pneumonia can safely be treated without the need for further testing. A macrolide or doxycycline is the treatment of choice for healthy patients younger than age 60 who have presumed pneumonia. Fluoroquinolones are not recommended in these patients because of increasing problems with antibiotic resistance.

55
Key Points In all patients in whom pneumonia is suspected, a chest x-ray should be ordered to provide diagnostic evidence with which to distinguish different patterns of infiltrates. The need for in-patient care can be determined by professional judgment, based on the patient's signs and symptoms; however, a risk factor calculation can be helpful in determining those with high predicted mortality. Obtaining blood cultures within 24 hours of admission and starting antibiotics within 4 hours of admission have been shown to reduce 30-day mortality and are considered quality indicators.

56
Key Points Because 30% to 50% of patients with community-acquired pneumonia never have a pathogen identified, it is recommended that empiric therapy selection be based on presumed organisms and their sensitivities, history of exposure, other comorbid health conditions, and x-ray findings. Aggressive testing including cultures, serology testing, and other rapid assays to determine the causative pathogen are appropriate for most inpatients. More invasive testing, including bronchoscopy, should be reserved for deteriorating patients in whom no etiology has been determined.

Similar presentations












, ranging in severity: Acute bronchitis - an acute respiratory tract infection in.>")












