Download presentation
Presentation is loading. Please wait.

3
Annual Report 2012 Sharp Injuries and Body Fluid Exposure:- NumberPercentage Physicians2736% Nursing Staff3546.7% Technicians56.6% HK Staff810.7% TOTAL75***

4
H B V Hapedna Virus double stranded DNA

5
Risk for Occupational Transmission of HBV ► HBsAg& HBeAg-positive blood : The risk of developing clinical hepatitis is 22%– 31%; The risk of developing serologic evidence of HBV infection is 37%–62%. ► HBsAg-positive, HBeAg-negative blood The risk of developing clinical hepatitis is 1%–6%; The risk of developing serologic evidence of HBV infection is 23%–37%

6
H C V Flavi virus. It is a single stranded RNA

7
Risk for Occupational transmission of HCV HCV-positive source is 1.8% (range: 0%–7%) rarely occurs from mucous membrane.
 rarely occurs from mucous membrane.")
8
H I V Retrovirus with 2 single stranded RNA

9
Risk for Occupational Transmission of HIV The risks for occupational transmission of HIV vary with the type and severity of exposure: ♦ In percutaneous exposure 0.3% ( 0.2%–0.5%) ♦ In mucous membrane exposure, approximately 0.09% ( 0.006%–0.5%)
 ♦ In mucous membrane exposure, approximately 0.09% ( 0.006%–0.5%)")
10
A percutaneous injury or contact of mucous membrane or nonintact skin WITH Blood,tissue and body fluids Semen and vaginal secretions, CSF, synovial, pleural, peritoneal, pericardial& amniotic fluid Feces, nasal secretions, saliva, sputum, sweat, tears, urine, and vomitus are not considered potentially infectious unless they contain blood. Contact without barrier protection to concentrated virus in lab Human bites: evaluation of HCP + Patient.

11
Treatment of an Exposure Site Wash needle stick and cuts with soap and water Flush splashes to the nose, mouth, or skin with water Irrigate eyes with clean water, saline THEN Report the incident to your supervisor Immediately seek medical treatment

14
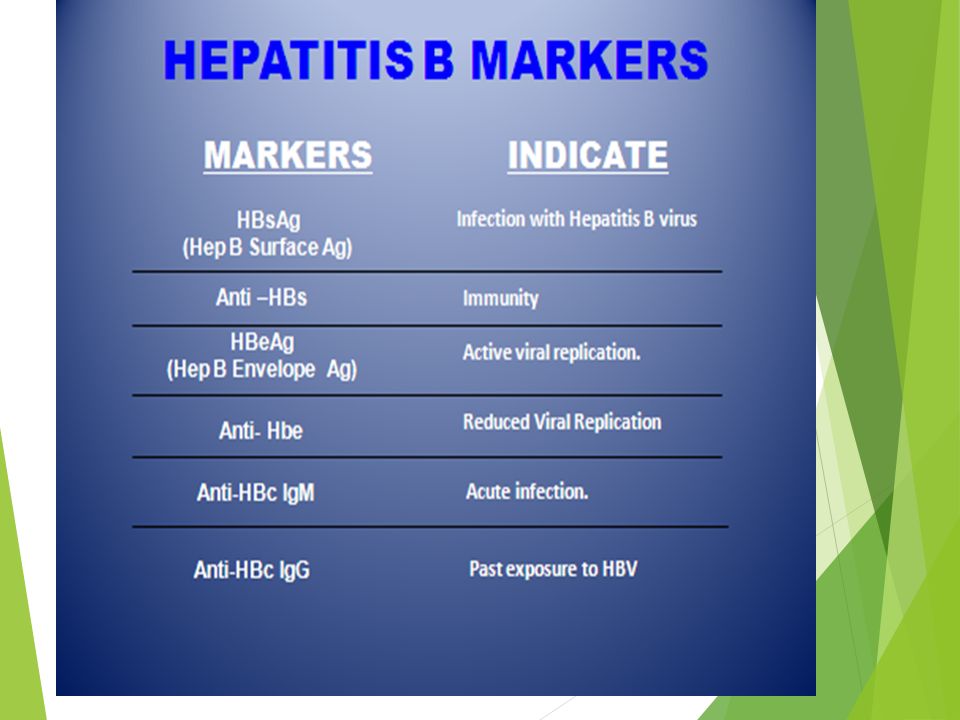
Evaluation of the Source HEPATITIS B MARKERS ANTI- HCV ANTI - HIV

15
Evaluation of the HCW HEPATITIS B MARKERS ANTI- HCV ANTI – HIV LFT in HCV Source

17
A.HBs Ag +ve source. a.Unvaccinated HCW Hepatitis B immunoglobulin (HBIG) 10-12 IU/Kg(500 IU) + Hepatitis B vaccine series ≈ PEP should be administered as soon as possible after exposure(preferably within 24 hours). The effectiveness of HBIG when administered >7 days after is unknown.
 IU/Kg(500 IU) + Hepatitis B vaccine series ≈ PEP should be administered as soon as possible after exposure(preferably within 24 hours). The effectiveness of HBIG when administered >7 days after is unknown..")
18
b. In previously vaccinated HCW i. Known responder (HBs Ab > 10 ml U/ml); no treatment. ii. If non-responder HBIG within 24 hours + Hepatitis B vaccination at the same time. OR Second dose of HBIG can be given 1month later.

20
HCV Positive Source A short course of interferon started early in the course of acute hepatitis C is associated with a higher rate of resolution.

21
≈Perform baseline testing for anti-HCV and ALT ≈ Earlier diagnosis of HCV infection is desired, testing for HCV RNA (R-T PCR QUALITATIVE AND QUANTITAVE ) ≈ Perform follow-up testing (e.g., at 4 & 6 months) for anti-HCV and ALT. ≈ Confirm all anti-HCV positive results.

22
HIV Positive Source Several Factors may increase the risk of transmission:- a. If HCW is exposed to a large quantity of blood. b. A procedure that involved a needle is placed directly in a vein or artery or a deep injury. c. If the source patient is in the terminal illness. d. If the injury is deep with hollow-bore needles or penetrating sharps-related event.

23
PEP in Percutaneous Exposure Class 1 asymptomatic HIV infection or known low viral load (e.g., (<1,500 RNA copies.ml). Class 2 symptomatic HIV infection, AIDS, acute zero conversion, or known high viral load.

24
PEP in Mucous Membrane Exposure Class 1 asymptomatic HIV infection or known low viral load (e.g., (<1,500 RNA copies.ml). Class 2 symptomatic HIV infection, AIDS, acute sero conversion, or known high viral load.

25
Antiretroviral Agents for PEP ≈ Nucleoside reverse transcriptase inhibitors (NRTIs). ≈ Nucleotide reverse transcriptase inhibitors (NtRTIs). ≈ Nonnucleoside reverse transcriptase inhibitors (NNRTIs), ≈ Protease inhibitors(PIs), and a single fusion inhibitor. HIV PEP should regimen (zidovudine (AZT) + lamivudine (3TC) complete a full 4-week )
. ≈ Nonnucleoside reverse transcriptase inhibitors (NNRTIs), ≈ Protease inhibitors(PIs), and a single fusion inhibitor. HIV PEP should regimen (zidovudine (AZT) + lamivudine (3TC) complete a full 4-week ).")
26
HCP Follow-up ≈ Anti- HIV test at 6 weeks, 3 months, 6 months Extending follow-up to 12 months ≈ EIA standard test ≈ direct virus assays not recommended

Similar presentations











 Additional Project Director Delhi State AIDS Control Society.>")













