Download presentation
Presentation is loading. Please wait.

1
0562/SAH/1112/SAH Prostate MRI: A paradigm shift Dr Andrew Stuart Radiologist, Sydney Adventist Hospital.

2
Learning objectives Briefly discuss the incidence, causes and symptoms of prostate cancer (PCa) Assess the traditional role of PCa diagnosis and the new role of mpMRI in the diagnosis Evaluate how mpMRI uses structural and functional imaging to assess for PCa Show examples of what PCa looks like on MRI and discuss biopsy options
 Assess the traditional role of PCa diagnosis and the new role of mpMRI in the diagnosis Evaluate how mpMRI uses structural and functional imaging to assess for PCa Show examples of what PCa looks like on MRI and discuss biopsy options")
3
Prostate MRI at the SAN – background Strong urological interest and a radiological desire to accommodate this was the initial driver. The service was initially offered in 2013 on our 1.5 T magnet With the hospital and radiology redevelopment and investment in new equipment the service was ramped up This was achieved by the investment in two GE 3T MRI`s and the collaboration with the prestigious Radbound University Nijmegen Medical Centre under the guidance of the world renowned expert in prostate MRI, Prof. Jelle Barentsz This collaboration was achieved by two radiologists and two radiographers training on site in Nijmegen, with initial supervision with double reads back in Sydney and ongoing double reading as required

4
What is the paradigm? Shifting away from a random, blind biopsy approach towards an image guided approach

5
Pity.. we can’t

6
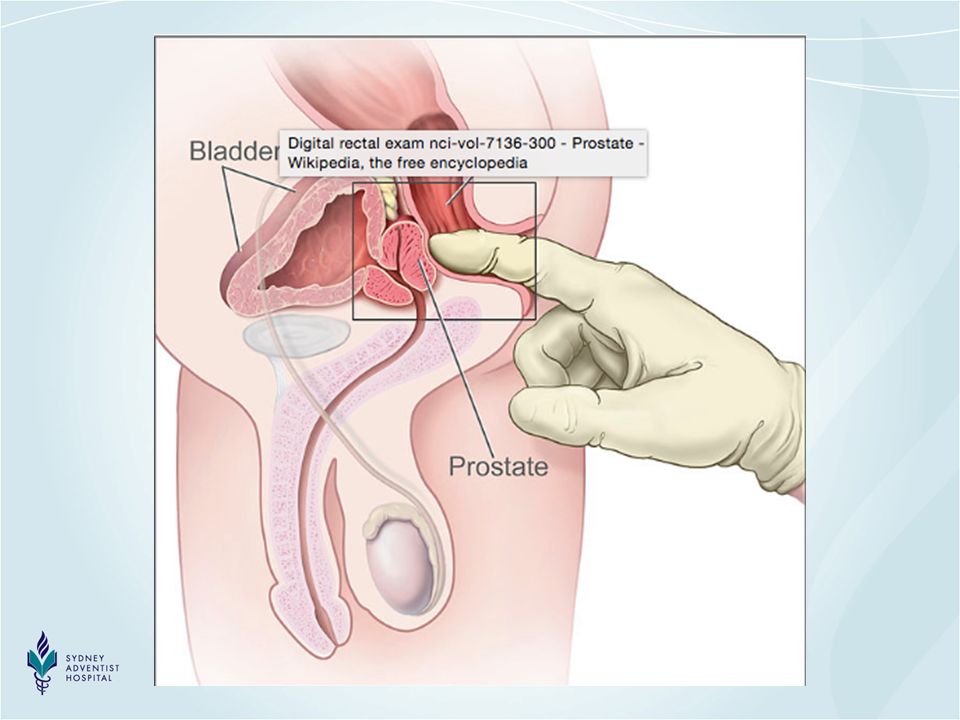
The prostate gland lying below the bladder

7
Prostate Cancer Prostate Cancer is the most common cancer diagnosed in Australia. ~20 000 new cases 2012. 30% of all cancers in Australian men. Third commonest cause of cancer death. 3112 deaths in 2013 (13 % of all cancer deaths in men). Commoner in elderly - 85% of cases in men >65 yrs. 1:5 men by age 85.
. Commoner in elderly - 85% of cases in men >65 yrs. 1:5 men by age 85..")
8
Causes of Prostate Ca Increasing age- risk increases rapidly > 50 yrs Family history- role of genetics ? diet- some assoc. with diet high in fat, low in fruit and veg. Race- African descent Association with High Testosterone levels.

9
Symptoms of Prostate Ca Non- specific urinary symptoms- frequent urination esp. at night, pain on urination, weak stream. Widespread disease- weight loss, fatigue and bone pain.

10
Prevention No known proven measures to prevent P CA Early diagnosis and treatment thus important

11
Treatment options Active surveillance- “watch and wait”- low grade disease Radical prostatectomy- surgery with curative intent (possible complications- impotence and incontinence) Radiotherapy Hormone therapy- reduce testosterone levels- widespread disease. Cryotherapy Vaccine treatment

13
Prostatectomy complications Impotence and incontinence Injury to the nerves and sphincter mechanism

14
Traditional diagnosis of Prostate Ca Digital Rectal exam- nodule, firmness, asymmetry PSA- Prostate Specific Antigen Multiple TRUS needle biopsies- usually “blind”, standard 12 or more needle biopsies.

15
Problems with Accurate Diagnosis DRE (digital rectal examination) Only as sensitive as your finger! Can only feel the back surface of gland

18
Problems with accurate diagnosis PSA- False positive ie other diseases causing raised PSA- inflammation (prostatitis), BPH. Only 25% of men with increased PSA (4-10) have cancer i.e. 3 OUT OF 4 WILL NOT HAVE CANCER False negative ie normal PSA but have cancer estimated at around 2%
 have cancer i.e. 3 OUT OF 4 WILL NOT HAVE CANCER False negative ie normal PSA but have cancer estimated at around 2%.")
19
Problems with accurate diagnosis TRUS biopsy- cannot usually see the tumour- “blind” so multiple random biopsies needed. may miss the tumour eg if in front of gland or small May find only low grade tumour and miss high grade tumour or may not find the high grade part of the tumour. May find only “insignificant” tumour and lead to over-treatment and risk of complications Associated risk of infection

20
TRUS biopsy Back of gland closest

22
Problems with accurate diagnosis The tumour itself ie biology “insignificant” cancer- cancer which will not kill you Heterogeneity of tumour- high and low grade mixed Important to find the high grade lethal tumour

23
Problems with Biopsy Non-agressive tumour biopsied

24
Problems with Biopsy Wrong / non- aggressive part of tumour biopsied

25
Problems with biopsy Needle does not reach tumour

26
So what`s new?

27
Multiparametric MRI(mpMRI) How we use multiple parameters of MRI i.e. morphology, enhancement characteristics and diffusion to evaluate for prostate cancer

28
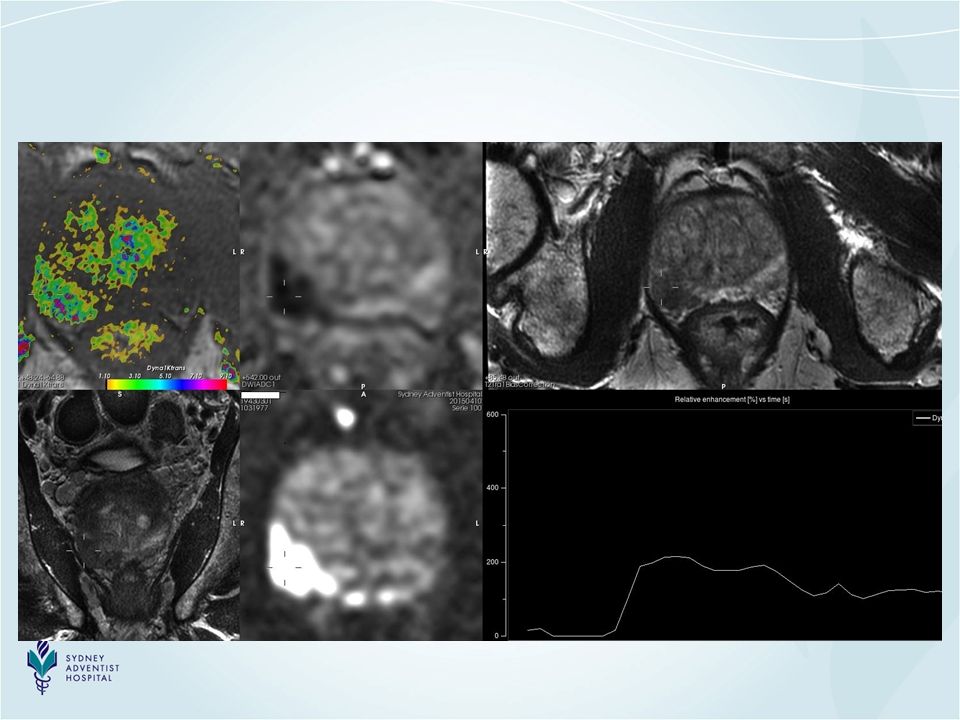
What is multi parametric MRI (mpMRI) Strong magnet- causes nuclei in atoms of tissues to align in magnetic field. When nuclei re-align( following a burst of radio waves) the radio waves are re-emitted and measured using the computing capability of the MRI scanner. The MRI computer calculates the position of the emitted radio source and formulates an image based on numerous discrete sources(pixels) of radio frequency. mpMRI uses 3 parameters a) T2 weighting for anatomy and structure b) DWI(diffusion) to create a `tissue density map` and c) DCE(contrast enhancement) to assess for the rapid enhancement of most tumours due to neo-vascularity.
 the radio waves are re-emitted and measured using the computing capability of the MRI scanner. The MRI computer calculates the position of the emitted radio source and formulates an image based on numerous discrete sources(pixels) of radio frequency. mpMRI uses 3 parameters a) T2 weighting for anatomy and structure b) DWI(diffusion) to create a `tissue density map` and c) DCE(contrast enhancement) to assess for the rapid enhancement of most tumours due to neo-vascularity..")
29
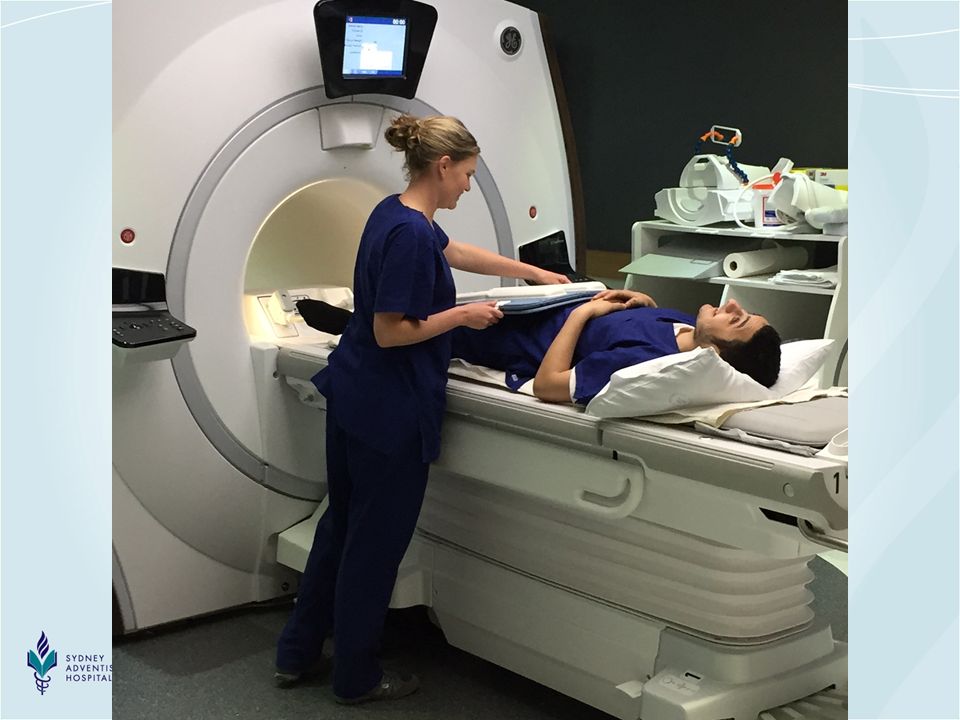
MRI- what’s involved? Around 30-40 min study Injection of buscopan (anti-spasmotic) Injection of contrast (gadolinium) to show blood flow May need light sedative if claustrophobic Slight noise during scanning- ear protection.
 Injection of contrast (gadolinium) to show blood flow May need light sedative if claustrophobic Slight noise during scanning- ear protection..")
31
How does MRI do all this? The anatomical and functional aspects of mpMRI enables its use as a biomarker to distinguish life threatening from non life threatening prostate cancer Small volume and low grade lesions are not detected …..advantage

32
How and why does cancer behave differently? Cancer tissue is more dense than normal tissue- cells are more numerous and tightly packed. We can measure this quantitatively with MRI with the diffusion sequence which in part measures tumour density. This cellular density correlates with aggressiveness of the tumour. So with a measurement we can get a good idea of tumour grade/ aggressivity.

33
How and why does cancer behave differently? To grow cancer needs nutrients. The cancer cells induce neovascularity. By injecting contrast we assess for early and abnormal enhancement to help detect a neoplastic focus. The enhancing properties of prostate cancer have recently been given lesser importance on MRI Pi- Rads criteria although are often still helpful, hence the routine administration of contrast

35
Prostate MRI - indications The detection of prostate cancer The local staging prostate cancer

36
Indications - generally accepted indications local staging (? beyond capsule) in the setting of high/rising PSA ( negative biopsy)…. and now prior to biopsy radiotherapy planning treatment detection local recurrence
 in the setting of high/rising PSA ( negative biopsy)…. and now prior to biopsy radiotherapy planning treatment detection local recurrence.")
37
Prostate MRI - questions to be answered Is there a cancer in the prostate gland? Where exactly in the gland is the cancer and can we guide the urologist to the correct area? Is it likely lethal/ high grade or is it low grade ie is it a “significant cancer” likely to kill? Is there more than one cancer? Has it spread outside the prostate already? Can be used to show local recurrence after treatment

38
A recent study at St Vincents Hospital found MRI of the prostate can exclude significant cancer in 97% of patients A recent study at Brisbane Wesley Hospital showed : *51% reduction in number men needing biopsies *Reduced problem of over diagnosis of non life threatening cancer by 90% *92% sensitivity in diagnosing life threatening prostate cancer

39
Prostate MRI - questions to be answered Is there a cancer in the prostate gland? Where exactly in the gland is the cancer and can we guide the urologist to the correct area? Is it likely lethal/ high grade or is it low grade ie is it a “significant cancer” likely to kill? Is there more than one cancer? Has it spread outside the prostate already? Can be used to show local recurrence after treatment

40
Prostate MRI - questions to be answered Is there a cancer in the prostate gland? Where exactly in the gland is the cancer and can we guide the urologist to the correct area? Is it likely lethal/ high grade or is it low grade ie is it a “significant cancer” likely to kill? Is there more than one cancer? Has it spread outside the prostate already? Can be used to show local recurrence after treatment

41
A study in the BJU by Egevad et al showed that the long term prognosis for prostate cancer on deferred treatment is predicted well by Gleason score. Gleason score= assessment of biological aggressiveness of the prostate cancer under the microscope Correlation in most instances between the Gleason score and the ADC values on the diffusion scan i.e. lower ADC values with higher Gleason score and higher grade cancer

42
Problems with biopsy Needle does not reach tumour

43
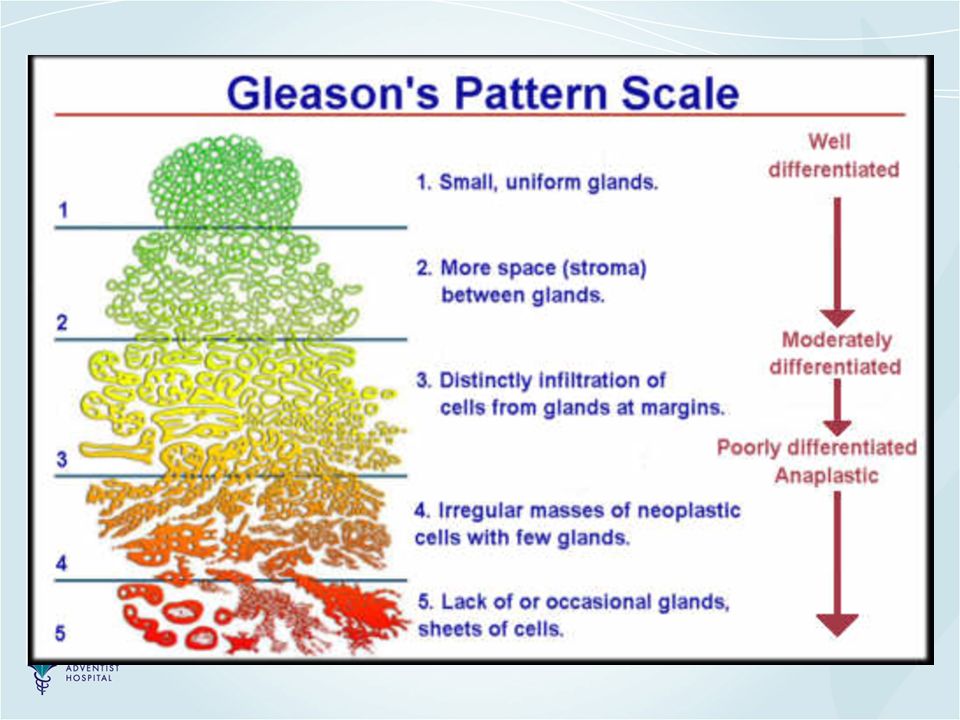
Grading Prostate Ca Gleason score- looks at structure under microscope 2 numbers added- primary and secondary pattern < 4- low cancer aggression 5 & 6- mildly aggressive 7- moderately aggressive 8-10- highly aggressive

45
Prostate MRI - question to be asked Is there a cancer in the prostate gland? Where exactly in the gland is the cancer and can we guide the urologist to the correct area? Is it likely lethal/ high grade or is it low grade ie is it a “significant cancer” likely to kill? Is there more than one cancer? Has it spread outside the prostate already? Can be used to show local recurrence after treatment

46
Prostate cancer is often multifocal The lesion with the lowest ADC values generally reflects the highest Gleason score i.e. grade Biopsy should be directed at this index lesion

47
Prostate MRI - question to be asked Is there a cancer in the prostate gland? Where exactly in the gland is the cancer and can we guide the urologist to the correct area? Is it likely lethal/ high grade or is it low grade ie is it a “significant cancer” likely to kill? Is there more than one cancer? Has it spread outside the prostate already? Can be used to show local recurrence after treatment

48
Evaluate for enlarged lymph nodes and focal bony lesions Asses for signs of focal extra-capsular extension

49
Prostate MRI - question to be asked Is there a cancer in the prostate gland? Where exactly in the gland is the cancer and can we guide the urologist to the correct area? Is it likely lethal/ high grade or is it low grade ie is it a “significant cancer” likely to kill? Is there more than one cancer? Has it spread outside the prostate already? Can it be used to show local recurrence after treatment?

50
In the setting of a radical prostatectomy any enhancing mass like area in conjunction with a rising PSA is highly suspicious of a local recurrence

51
What does cancer look like on mpMRI ? Different signal to normal tissue due to different structure Nodule/ mass Alteration of normal shape/ outline of tissues Masses and nodules outside the prostate that should not be there.

53
From MRI to tissue diagnosis Any focal lesion is described by the radiologist using Pi-Rads nomenclature to convey the level of concern to the referring doctor The position within the prostate is noted using a standard diagrammatic model The urologist will then if indicated proceed to biopsy

55
What is the PI-RADS score Structured reporting system for evaluating the prostate for prostate cancer It uses the multi parametric sequences i.e. T2 and diffusion to stratify a level of suspicion with a numerical value (1-5) and contrast enhancement (present or absent) the peripheral zone (where 70 % of cancers occur) is largely influenced by diffusion properties and the more central transition zone by morphological features (T2 properties). Contrast enhancement carries lesser weighting under Pi-RADS criteria
 and contrast enhancement (present or absent) the peripheral zone (where 70 % of cancers occur) is largely influenced by diffusion properties and the more central transition zone by morphological features (T2 properties). Contrast enhancement carries lesser weighting under Pi-RADS criteria.")
56
What is the PI-RADS score PI-RADS 1: very low risk of Ca (clinically significant Ca highly unlikely) PI-RADS 2: low risk (clinically significant Ca unlikely) PI-RADS 3: intermediate risk(presence Ca equivocal) PI-RADS 4: high risk(clinically significant cancer likely present) PI-RADS 5: very high risk( clinically significant cancer highly likely)
 PI-RADS 2: low risk (clinically significant Ca unlikely) PI-RADS 3: intermediate risk(presence Ca equivocal) PI-RADS 4: high risk(clinically significant cancer likely present) PI-RADS 5: very high risk( clinically significant cancer highly likely)")
57
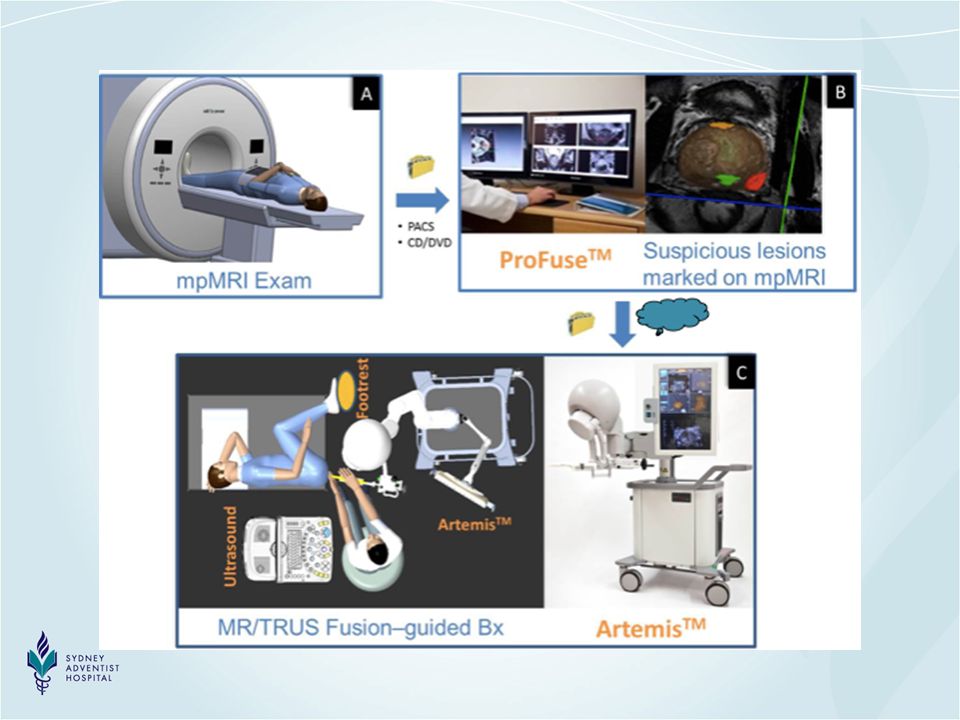
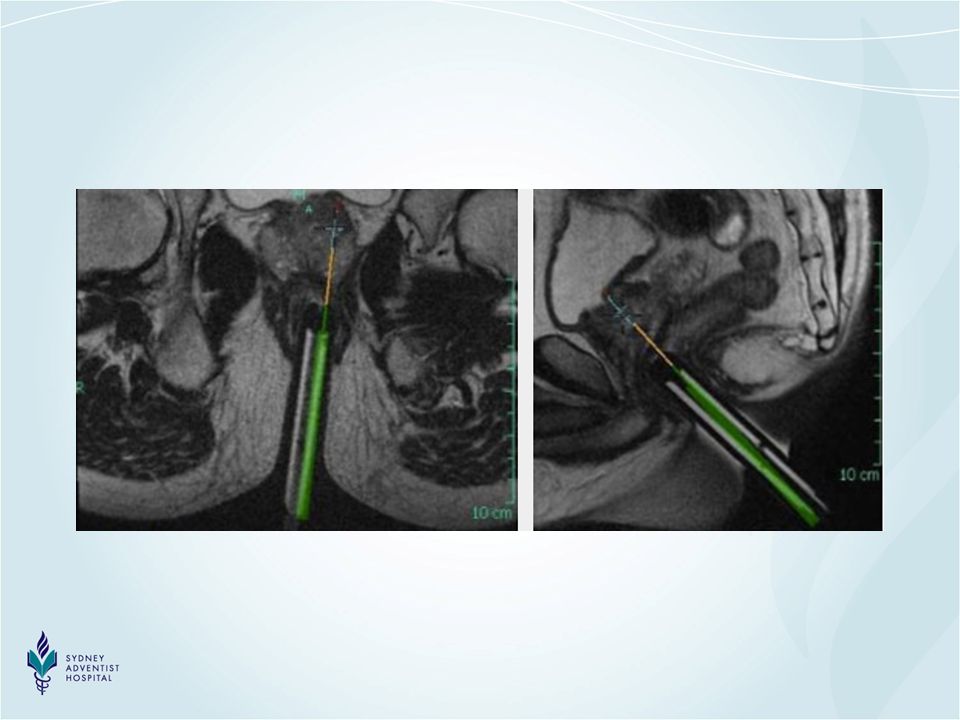
Biopsy options available following an MRI identified lesion requiring tissue diagnosis MRI-ultrasound cognitive fusion TRUS/MRI fusion imaging techniques MR-guided biopsy

59
Biopsy options available following an MRI identified lesion requiring tissue diagnosis MRI-ultrasound cognitive fusion TRUS/MRI fusion imaging techniques MR-guided biopsy

61
Biopsy options available following an MRI identified lesion requiring tissue diagnosis MRI-ultrasound cognitive fusion TRUS/MRI fusion imaging techniques MR-guided biopsy

63
Anticipated change of GP practice in the future wrt prostate Ca Availability of a powerful risk stratification tool which will reduce patient anxiety and need for biopsy Potential for reduction in number of biopsies Will hopefully make the role of PSA testing less controversial when used in conjunction with mpMRI

64
Comparison of available risk stratifiers for detecting prostate Ca AUC(computed index combing sensitivity and specificity) (perfect test is 1.0) PSA = 0.56-0.59 PSA F/T = 0.63 PHI = 0.7 PCA3 = 0.59- 0.9 PSA density = 0.74 (if PSA < 4) MRI/MRGB = 0.9
 (perfect test is 1.0) PSA = PSA F/T = 0.63 PHI = 0.7 PCA3 = PSA density = 0.74 (if PSA < 4) MRI/MRGB = 0.9")
65
The future ? Prostate MRI for all/ screening ? Normal MRI- no biopsy ? Biopsy only MRI- visible lesions ? Focal therapy for localised disease ?

Similar presentations







 Bob White, AIM-IRS ABMTS Milwaukee, WI.>")
















