Download presentation
Presentation is loading. Please wait.

1
Top 5 papers of Prehospital care Recommended by Torpong

4
Combitube

7
452 Studies reviewed 3 RCT done in urban area

8
Result Compare survival rate between "ET tube Vs Combi-tube" (All operated by physician) Non significant (RR 0.44, 95% CI 0.09 to 1.91) Compare survival disadvantage between "ET tube Vs Esophageal gastric airway” Non significant (RR 0.86, 95% CI 0.39 to 1.9) Compare result & Neurologic outcome in children airway intervention between "Paramedic intubation" Vs "Bag valve mask ventilation+Hospital intubation by Emergency physician“ Non significant ( RR 0.87, 95%CI 0.62 to 1.22)
 Non significant (RR 0.44, 95% CI 0.09 to 1.91) Compare survival disadvantage between ET tube Vs Esophageal gastric airway Non significant (RR 0.86, 95% CI 0.39 to 1.9) Compare result & Neurologic outcome in children airway intervention between Paramedic intubation Vs Bag valve mask ventilation+Hospital intubation by Emergency physician Non significant ( RR 0.87, 95%CI 0.62 to 1.22)")
9
Conclusion Efficacy of emergency intubation depend on "Skill" Non traumatic cardiac arrest not need Intubation at scene Trauma & Pediatric patient in urban area "No evidence need prehospital intubation"

11
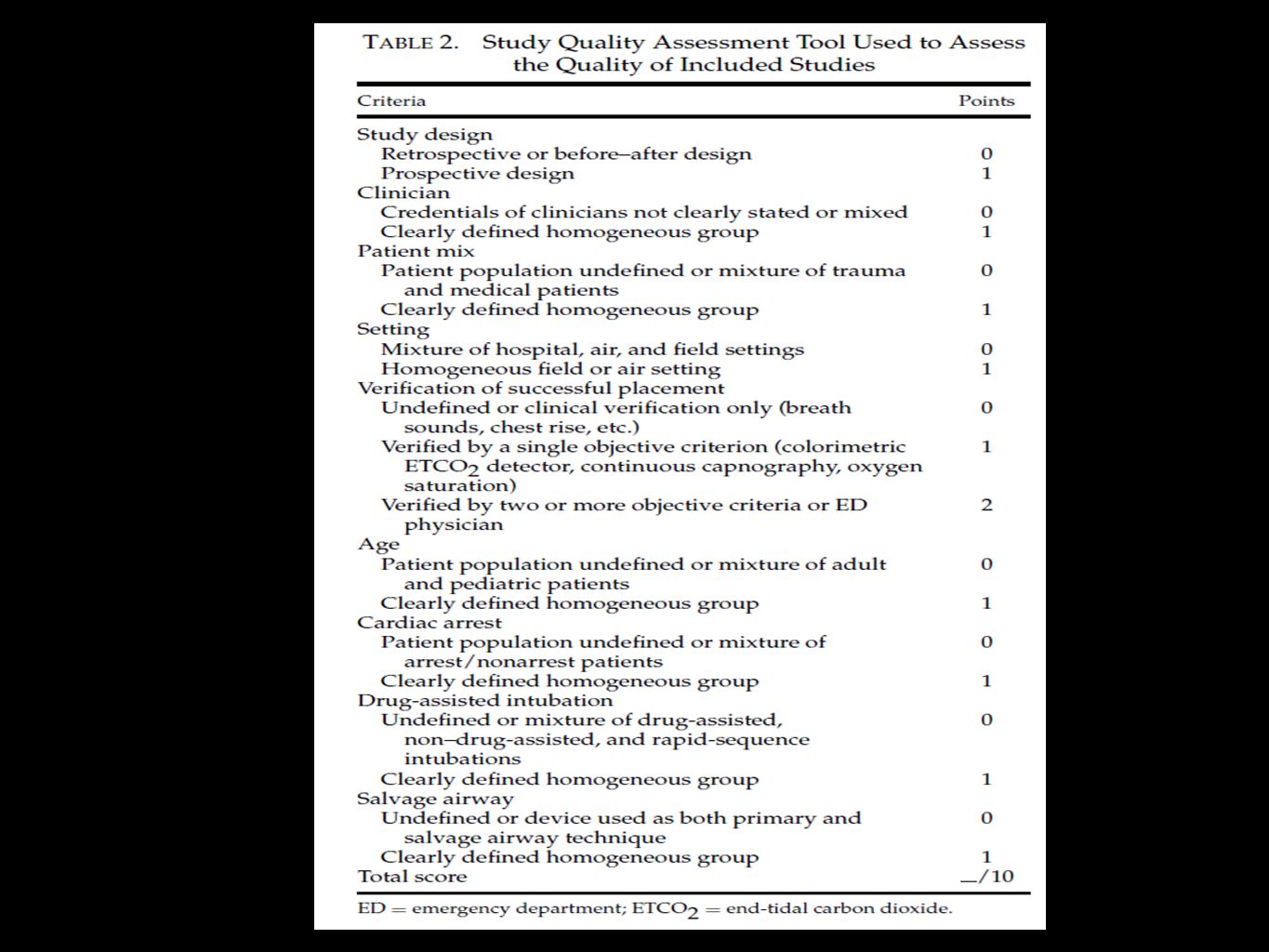
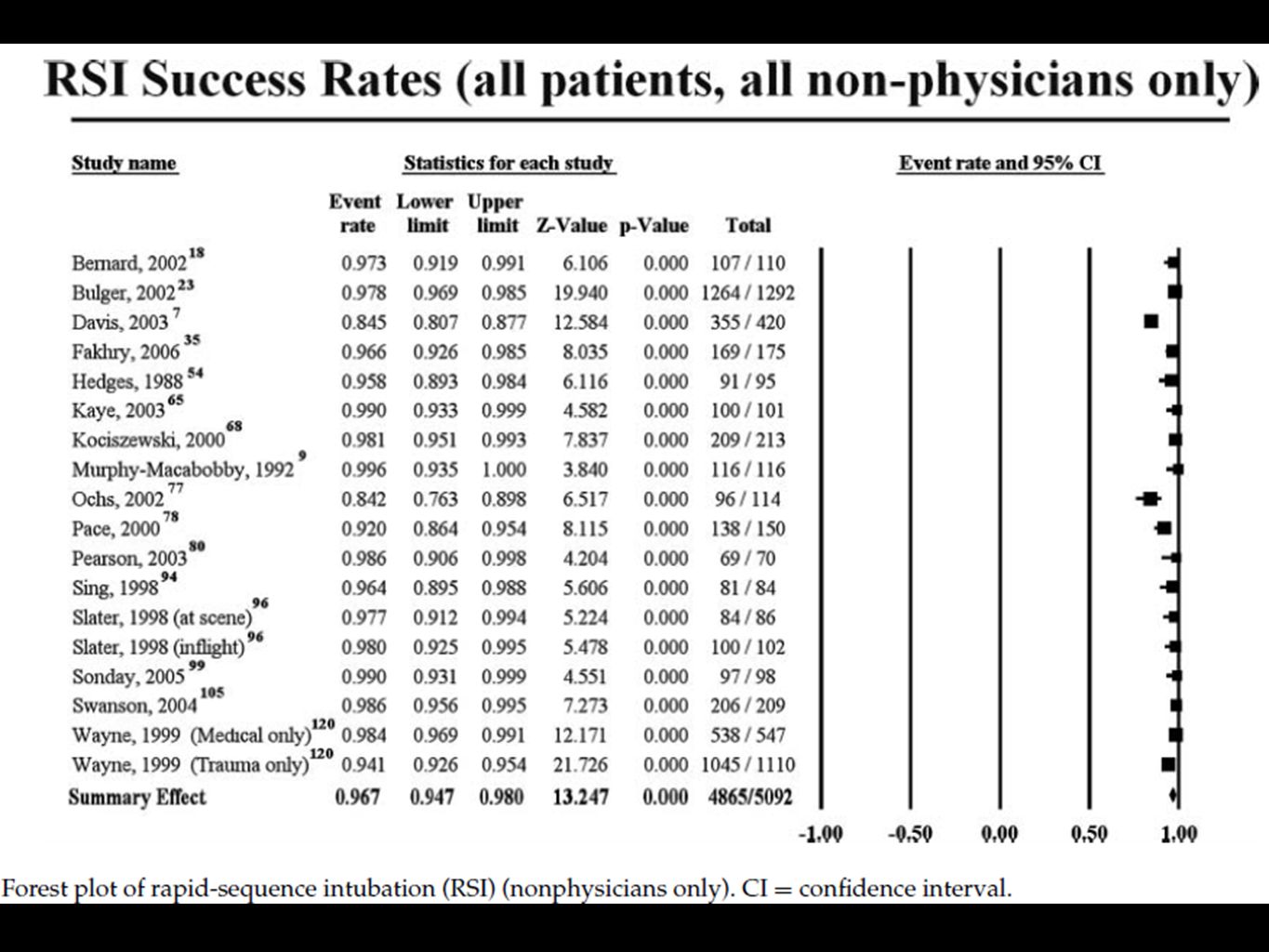
Systemic review, English langue article from Pubmed (November 2008 to July 2009) To determine placement success rates in prehospital patients who received oral endotracheal intubation and nasotracheal intubation. Most studies used clinician self ‐ reported success rates, mostly on the ground PREHOSPITAL EMERGENCY CARE JULY/SEPTEMBER 2010 VOLUME 14 / NUMBER 3

12
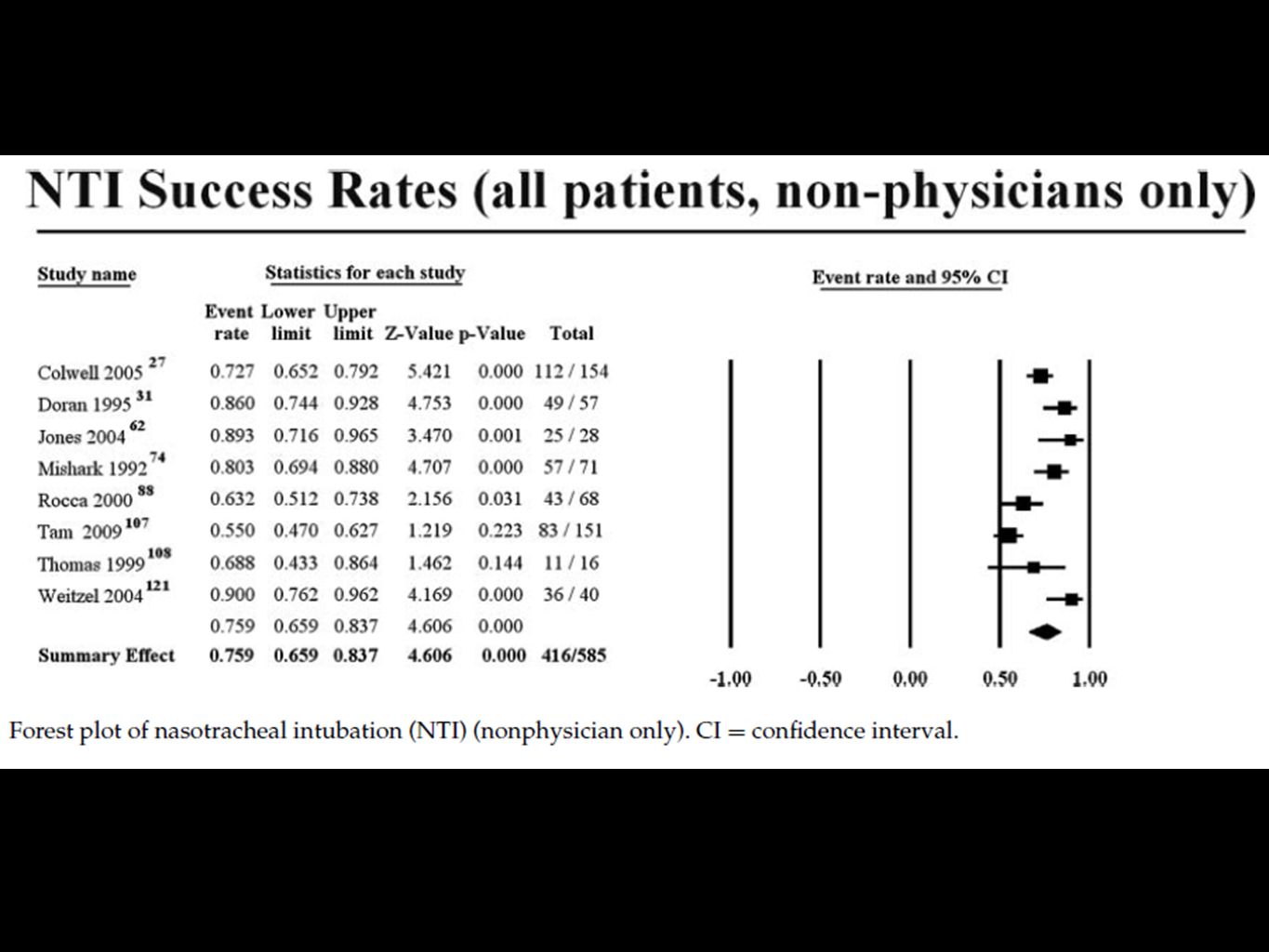
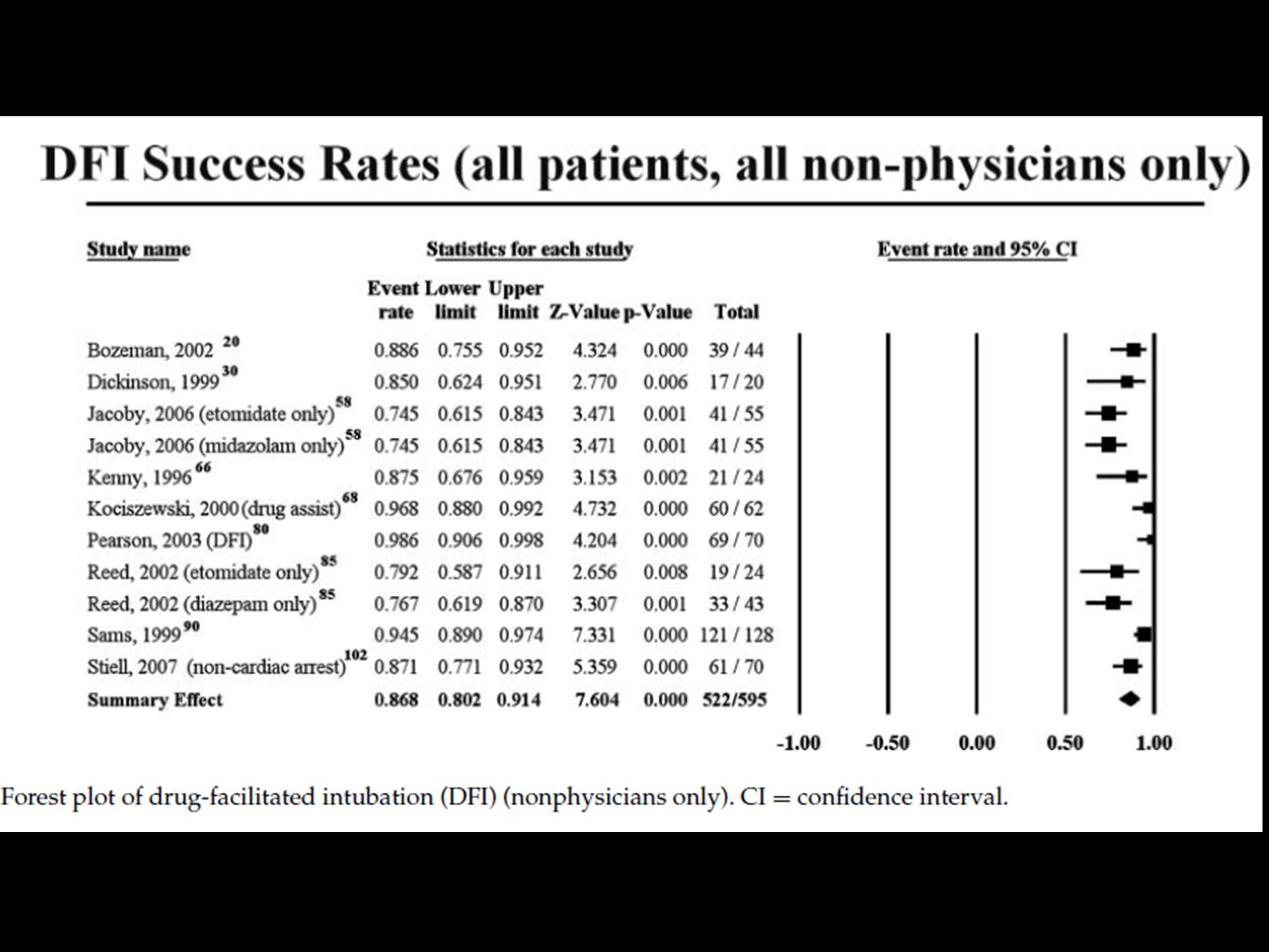
Two reviewers independently performed study selection. Disagreements were resolved by consensus. Two reviewers independently assessed study quality using a 10 ‐ point scale (mean 5.1 for oral endotracheal intubation studies, mean 4.6 for nasotracheal intubation studies). 117 Studies Oral endotracheal intubation(OETI), 23 Studies Nasotracheal tube(NTI), 57,132 Prehospital patients PREHOSPITAL EMERGENCY CARE JULY/SEPTEMBER 2010 VOLUME 14 / NUMBER 3
. 117 Studies Oral endotracheal intubation(OETI), 23 Studies Nasotracheal tube(NTI), 57,132 Prehospital patients PREHOSPITAL EMERGENCY CARE JULY/SEPTEMBER 2010 VOLUME 14 / NUMBER 3.")
19
Conclusion Oral ET intubation relative low success rates for non arrest patient Drug facilitated intubation & Rapid sequence induction increase success rate Nasotracheal tube has lower success

21
Academic Emergency Medicine.2006;13(1):84 ‐ 89.
:84 ‐ 89.")
22
Aim: Prehospital 12-lead electrocardiogram (PHECG) interpretation and advance emergency department (ED) notification, reduces deaths in comparison with standard care Methods: Search MEDLINE (1985 to 2003), EMBASE (1980 to 2003), Current Contents (1993 to 2003), Dissertation Abstracts (1981 to 2003), the Cochrane Library and the Index to Scientific and Technical Proceedings (1991 to 2003) Only studies reported in the English language were included
 interpretation and advance emergency department (ED) notification, reduces deaths in comparison with standard care Methods: Search MEDLINE (1985 to 2003), EMBASE (1980 to 2003), Current Contents (1993 to 2003), Dissertation Abstracts (1981 to 2003), the Cochrane Library and the Index to Scientific and Technical Proceedings (1991 to 2003) Only studies reported in the English language were included")
23
Two authors independently screened studies, blinded to the author, year of publication, journal, results and conclusions. Any disagreements were resolved by consensus. Agreement between reviewers was assessed using a weighted kappa statistic

24
Results: Only 5/1,283 met the inclusion criteria. The weighted kappa for selection was 0.61 (standard error [SE], 0.045) for titles, 0.63 (SE, 0.051) for abstracts, and 0.79 (SE, 0.146) for full articles. Mean study quality measures by two independent reviewers were 6.0/15 and 5.5/15 (correlation coefficient, 0.85; p = 0.06).
 for titles, 0.63 (SE, 0.051) for abstracts, and 0.79 (SE, 0.146) for full articles. Mean study quality measures by two independent reviewers were 6.0/15 and 5.5/15 (correlation coefficient, 0.85; p = 0.06)..")
25
Mortality One study reported all-cause mortality, with a statistically nonsignificant reduction from 15.6% to 8.4% respectively; P=0.22. Time intervals No statistically significant difference between intervention and control for the on ‐ scene time interval (3 studies; weighted mean difference 1.19 minutes, 95% CI: ‐ 0.84, 3.21). The weighted mean door-to-needle interval was shortened by 36.1 minutes (95% CI = 9.3 to 63.0: range of means, 22–48 minutes vs. 50–97 minutes). There were insufficient data to conduct the planned sensitivity analysis.
. The weighted mean door-to-needle interval was shortened by 36.1 minutes (95% CI = 9.3 to 63.0: range of means, 22–48 minutes vs. 50–97 minutes). There were insufficient data to conduct the planned sensitivity analysis..")
26
Conclusions: For patients with AMI, the literature would suggest that PHECG and advanced ED notification reduces in hospital time to fibrinolysis. One controlled trial found no difference in mortality with this out-of-hospital intervention.

29
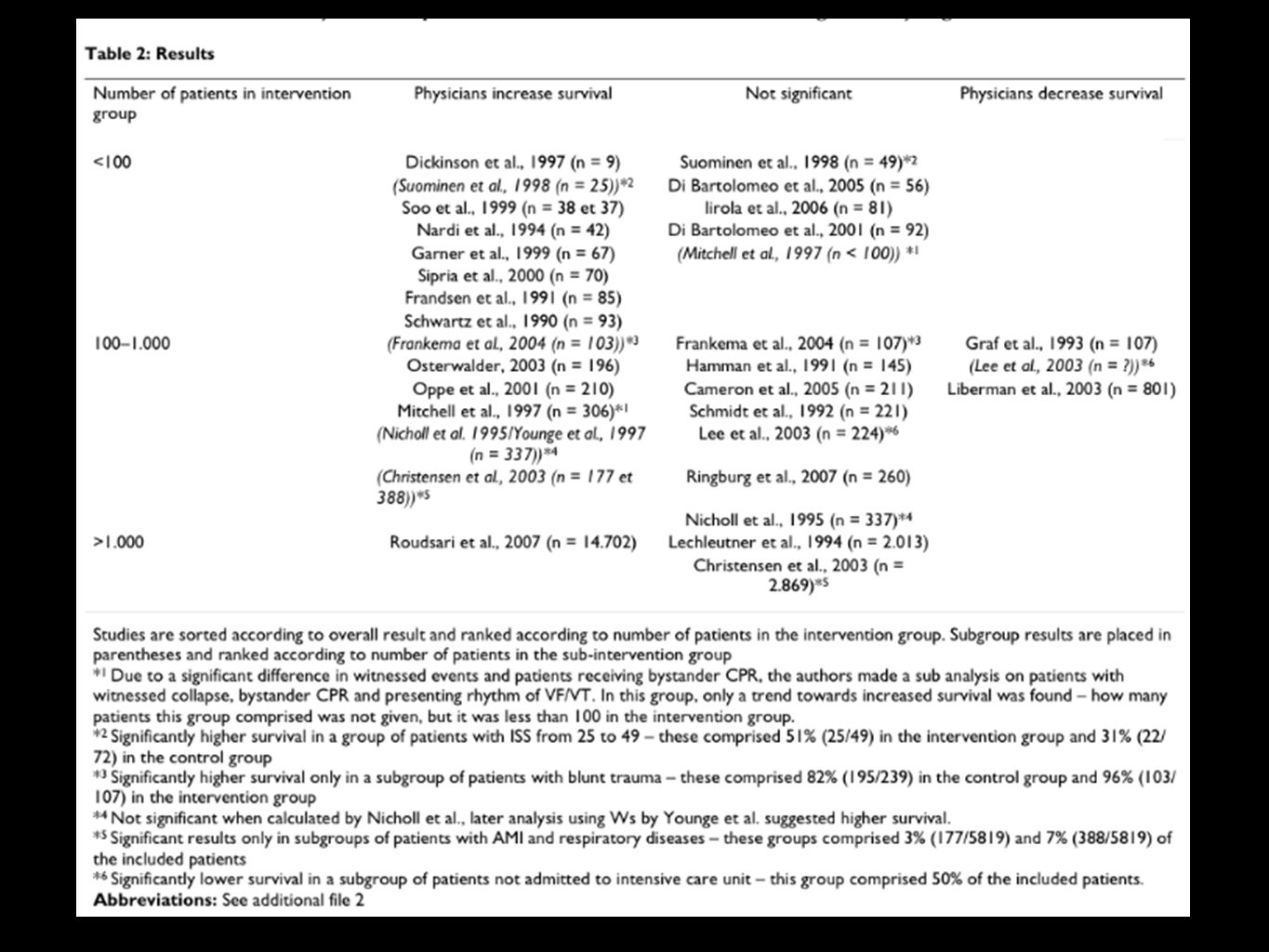
AIM: Comparing patient survival with prehospital physician treatment Vs Treatment by paramedic Systemic review in databases PubMed, EMBASE, Cochrane from January 1, 1990 to November 24, 2008 26 from 1,359 studies met inclusion criteria Of 26 reviewed studies as 16 “Cohort studies”, 5 “Systemic comparison studies”, 5 “before and after studies”.

32
Conclusion A systematic review revealed only few controlled studies examining survival with prehospital physician treatment. Increased survival with physician treatment was found in the groups most extensively studied (trauma patients, patients with cardiac arrest, respiratory diseases, acute myocardial infarction). The quality and strength of the included studies was variable and many conditions remain unexamined.
. The quality and strength of the included studies was variable and many conditions remain unexamined..")
35
ALS vs BLS ALS Using invasive methods(intravenous fluids, medications and intubation) Transfer by ground ambulance (GA) or helicopter Implemented by physicians or paramedics BLS used to assure patient's vital functions until the patient has been transported to definitive care Implemented by paramedics or emergency medical technicians
 Transfer by ground ambulance (GA) or helicopter Implemented by physicians or paramedics BLS used to assure patient s vital functions until the patient has been transported to definitive care Implemented by paramedics or emergency medical technicians")
36
Aim: to compare the effectiveness of ALS- and BLS-level prehospital care. Search: PubMed, preMEDLINE OVID Medline, CRD databases, Cochrane database of systematic reviews, EBM reviews, CINAHL. 46/1,333 studies met inclusion criteria(1 RCT, 15 prospective follow-up studies, 30 retrospective design)
.")
37
*ALS & transport by HA, 2/5 harmful from on awake intubation by paramedic **Confounding from treatment level of Hospital and type of transportation ALSDrawBLS Prehospital thrombolysis for myocardial infarction 5(1 Sig)00 Cardiac arrest711 Penetrating and unselected traumas 05 5 Blunt head injury 5*10 Multiple Blunt injury 1**52 Respiratory distress200 Other diseases1 (Epileptic) 1 (Stroke,Hypoglycemia)
00 Cardiac arrest711 Penetrating and unselected traumas 05 5 Blunt head injury 5*10 Multiple Blunt injury 1**52 Respiratory distress200 Other diseases1 (Epileptic) 1 (Stroke,Hypoglycemia)")
38
Conclusion: ALS seems to improve survival in patients with myocardial infarction BLS seems to be the proper level of care for patients with penetrating injuries. Some studies indicate a beneficial effect of ALS among patients with blunt head injuries, multiple injuries, epileptic seizures, respiratory distress. Need for high quality controlled clinical studies & the development of prehospital care requires uniform and full documentation and follow-up of patients as well as register studies based on real- life data.

39
การนำไปใช้จริงใน รพ.มหาราชนครศรีธรรมราช การใส่ท่อช่วยหายใจที่จุดเกิดเหตุควรทำโดยแพทย์ การใช้ยานำสลบทำให้การใส่ท่อช่วยหายใจที่จุดเกิดเหตุได้ง่ายขึ้น Combitubeไม่ใช่อุปกรณ์ที่จำเป็นในรถEMS ในกรณีผู้ป่วยอาการหนักควรเป็นทีมALSออกปฏิบัติการ การทำEKG12Leadที่Sceneยังไม่จำเป็น ดังนั้นยังไม่ต้องมี EKG ในรถ EMS ในกรณีผู้ป่วยถูกแทง หากทีมALSไม่พร้อมที่จะออกปฏิบัติการ อาจให้ ทีมFR(ที่มีEMT-Bร่วมปฏิบัติการด้วย)นำส่งได้เลย
นำส่งได้เลย")
Similar presentations

























. The relationship between emergency department.>")



