Download presentation
Presentation is loading. Please wait.

35
Secondary toxic goiter

37
Retro sternal goiter

39
Recurrence (70% False recurrence)
")
42
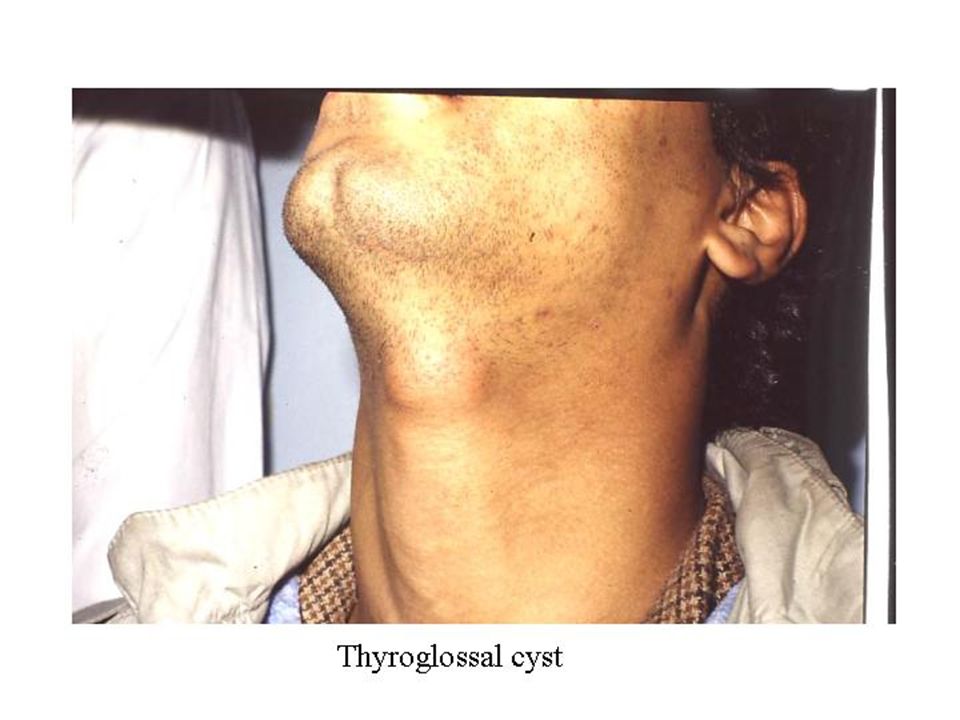
Solitary thyroid nodule

49
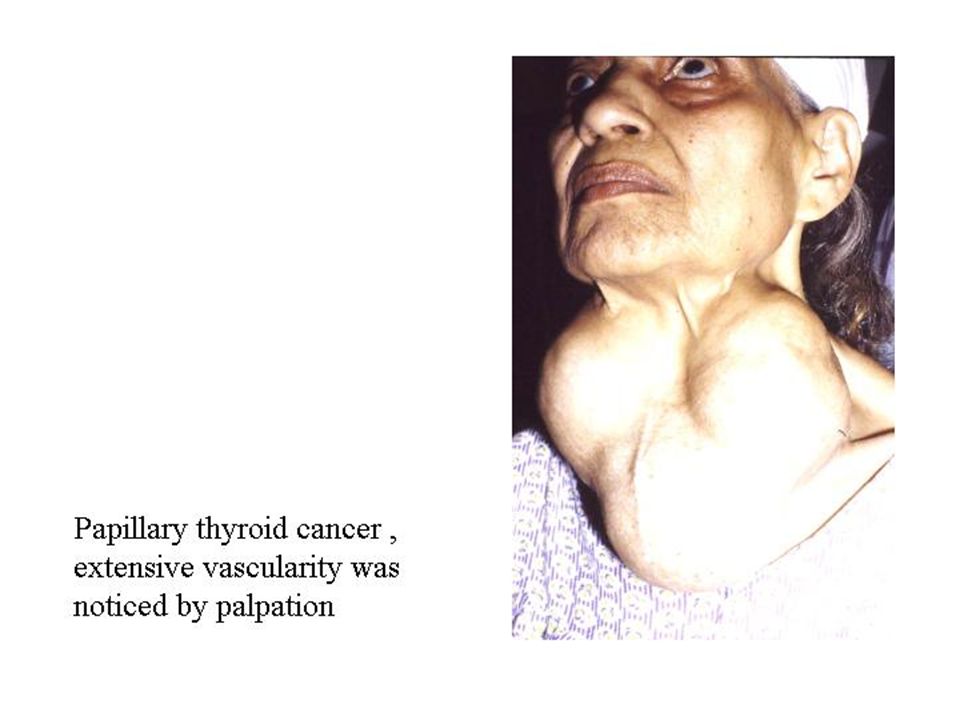
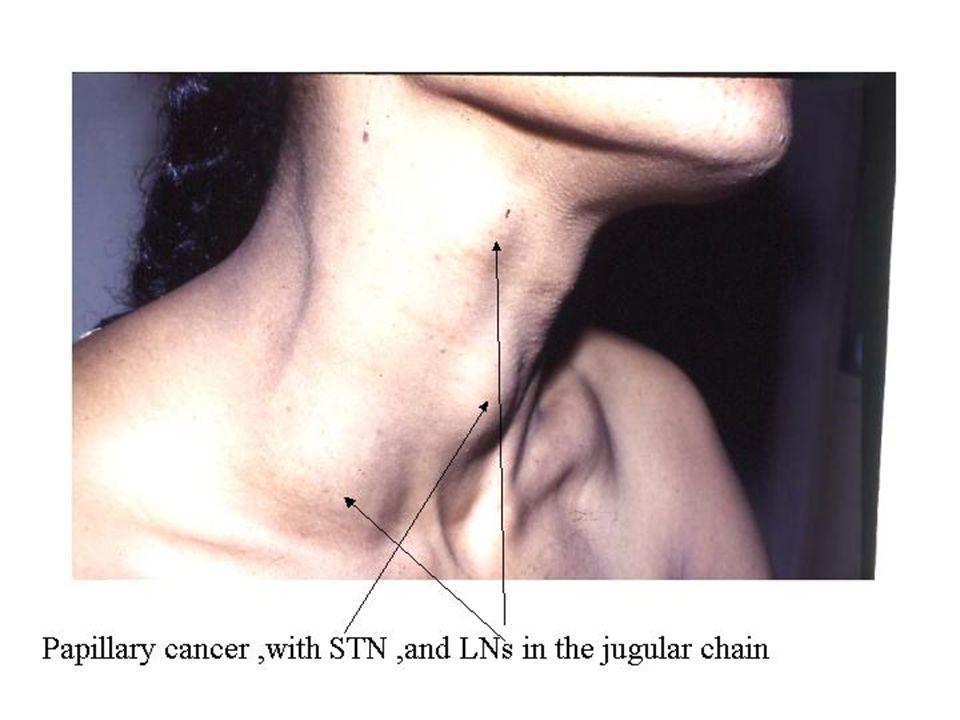
Thyroid Malignancy 4 major types Papillary Folicular Anaplastic Medullary

50
Papillary Huge enlargement STN LN at the side of the neck Pressure manifestations Metastases lung and bone 10%

59
Follicular Bone metastases Recent rapid enlargement of pre exciting goitre STN

60
Follicular carcinoma

61
Change in long standing goitre

62
Anaplastic Carcinoma

64
Thyroid carcinoma Diagnosis Work-up fine needle aspiration most important in evaluating thyroid nodules preoperative diagnosis of most thyroid cancers helps to plan the extent of surgery Results categorized as: cancer follicular neoplasm (suspicious or indeterminate) insufficient (should be repeated, half of repeat specimens are adequate for diagnosis) benign
 insufficient (should be repeated, half of repeat specimens are adequate for diagnosis) benign")
65
Thyroid carcinoma Diagnosis Work-up fine needle aspiration thyroid nodes requiring surgery decrease from 67% to 44% 85% of nodules called malignant on FNA will prove to be malignant only 3% of patients with benign citology will have thyroid cancer suspicious FNA samples – 50% of papillary and 20% of follicular are cancer 20% of nodules that yield an abundance of follicular cells with little or no colloid are minimally invasive follicular cancers

66
Thyroid carcinoma Diagnosis Work-up TSH measurement neck ultrasound: (size, borders, solid, cystic,uni/multicentri c, lymphnodes, guides FNA)
")
67
Thyroid carcinoma Diagnosis Work-up scintigraphy: capacity to concentrate radioisotope, cold nodules Are 15-20% malignant essential in postoperative follow-up (remnant tissue, metastatic tumors, WBS)
")
68
Thyroid carcinoma Diagnosis Work-up scintigraphy:

69
Thyroid carcinoma Diagnosis Work-up barium swallowing

70
Thyroid carcinoma Diagnosis Work-up computed tomography

71
Thyroid carcinoma Diagnosis Work-up computed tomography

72
Thyroid carcinoma Diagnosis Work-up magnetic resonance imaging

73
Thyroid carcinoma Diagnosis Work-up chest X-ray

74
Bone metastases pathological fracture

75
Brain metastases Treat like any other brain tumor: steroids, dextran, under close observation by a neurologist or neuro surgeon

76
I-123 Whole Body Scan

77
Tc-99m sestaMIBI

78
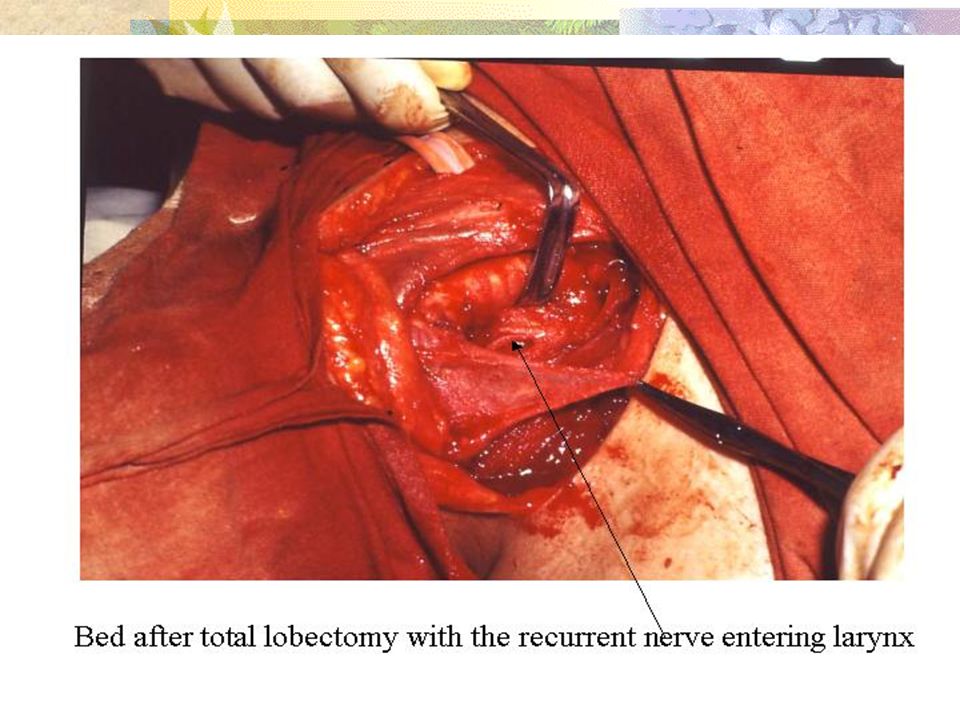
Standard Initial Treatment Usual Pathway Total Thyroidectomy Remove the thyroid with all cancerous tissue Radioactive Iodine Treatment Destroy any microscopic residual thyroid tissue Completely dependent on exogenous levothyroxine Without any functional thyroid tissue

79
Levothyroxine Therapy Thyroid Cancer Normalize TSH Prevent Symptoms of Hypothyroidism Suppress TSH Decreased Risk of Recurrence of Thyroid Cancer Without any functional thyroid tissue

80
Thyroid carcinoma Postoperative period Whole body scan

81
Thyroidectomy

Similar presentations

























































>")






>")



. Anatomy Anatomy.>")


